RESEARCH ARTICLES
Socioepidemiological profile of clients with limited mobility and of their caregivers
Rebeca Ainoã de Souza VianaI; Fernanda Bonatto ZuffiII; Rosali Isabel Barduchi OhlIII; Suzel Regina Ribeiro ChavagliaIV
INurse. Clinics Hospital of the Federal University of the Minas Gerais Triangle. Uberaba, Minas Gerais State, Brazil. E-mail: rebecasouza_mg@yahoo.com.br.
IINurse. Master in Nursing. Assistant Professor from the Graduation Nursing Course at the Federal University of the Minas Gerais Triangle. Uberaba, Minas Gerais State, Brazil. E-mail: fbzuffi@yahoo.com.br.
IIINurse. PHD in Nursing. Adjunct Professor from the Department of Clinical and Surgical Nursing of the Paulista Nursing School at the Federal University of São Paulo. São Paulo, São Paulo State, Brazil. E-mail: rosali.ohl@unifesp.br.
IVNurse. PHD in Nursing. Associated Professor from the Graduation Nursing Course at the Federal University of the Minas Gerais Triangle. Uberaba, Minas Gerais State, Brazil. E-mail: suzel.ribeiro@yahoo.com.br.
VWork developed as part of a project funded by the Research Support Foundation of the Minas Gerais State.
ABSTRACT: This study aimed at characterizing the socioepidemiological profile of clients with limited mobility and of caregivers monitored by the teams of Family Health Strategy of a Sanitary District of Uberaba, Minas Gerais State. It is a descriptive and cross-sectional study, with quantitative approach. The results showed that the majority of the 101 identified users were older than 60 years, female and retired; had incomplete Elementary School, low family income, multiple self-reported comorbidities and dependence on caregivers. According to the Braden Scale, the majority of the users showed moderate and high risk for developing pressure ulcers, and 22 (21,8%) of them had these ulcers. The predominant characteristics of the 95 caregivers were: age between 40 and 60 years old, female, housewife, incomplete Elementary School, low family income, kinship to the user, living with it and performing multiple tasks. Health services must support and monitor users with limited mobility and caregivers, aiming at the empowerment to better face the daily difficulties.
Keywords: Limited mobility; Caregivers; Pressure ulcer; Nursing.
INTRODUCTION
The Brazilian Health Ministry has striven to promote the development of modalities of careV aimed at the desinstitutionalization of patients. For this purpose, it has deployed the Family Health Strategy (FHS) and the Home Care Program (HCP), among others, as alternatives to improve the quality of health care of the population1. The increased life expectancy and the consequent population aging, coupled with the increased incidence of chronic diseases, which mainly affect the elderly people, brought the growing demand of health services as a result. In this context, there are family caregivers who, along with FHS teams, have become a component of the public health actions to meet this share of the population2.
The world's population aging has originated specific health policies, which have sought to minimize the effect of the limitations that this condition of chronicity determines in the daily lives of people. Some health problems, common to the aging process, generate functional disability for the completion of daily activities, thereby affecting the decision-making, causing loss of their autonomy and future dependence on different levels.
Functional disability is defined as any restriction or lack of ability that an individual undergoes to conduct its functions, faced by what one considers acceptable for a human being. The assessment of these limitations is important because of its close relationship with the health disorders and chronic conditions that might arise as a result of this process3. It might be assessed by means of the indication of difficulty or the need for help in relation to basic tasks and/or more complex activities, necessary to independently live in the community. Mobility measures are also part of this assessment of functional decline and have proven to be valuable in the study of the relationship of the functional status, with demographic characteristics, chronic conditions and health-related behaviors4.
In general, limited mobility is seen as the inability of the individual to freely move itself, and might vary between individuals with similar conditions, or in the same subject, in different periods of life. It might be manifested in a sudden or slow manner, according to its extent and duration, and is a contributing factor to variable health problems, ranging from the self-care deficit to impaired social interaction5.
Thus, the knowledge of the profile of users with impaired physical mobility and of their caregivers might provide with subsidies for planning local services aimed at the attendance of this population, thereby meeting the individual requirements of clients and of their family members.
Accordingly, this study aimed at characterizing the socioepidemiological profile of clients with limited mobility and of caregivers monitored by the staffs of Family Health Strategy of a Sanitary District of Uberaba, Minas Gerais State.
LITERATURE REVIEW
Impaired physical mobility is a nursing diagnosis defined as the status in which the individual experiences a limitation in independent and/or voluntary physical movements of its body or of one or more extremities6.
The clinical picture for impaired physical mobility provokes problems such as change in gait, thereby increasing the risk of falls, besides causing greater dependence on the Daily Life Activities (DLAs), inability to return to working activities, difficulty in moving in the household itself, in around house and in other community locations7.
People with impaired mobility, especially those restricted to beds or wheelchairs, are subject to greater likelihood of developing cardiovascular, respiratory, musculoskeletal and skin disorders, associated to the degree and duration of immobility. Among the most common complications, one could mention the pressure ulcers (PUs)8,9.
All health professionals must have knowledge about prevention measures, risk factors and characteristics of PUs, aiming at the implementation of more effective preventive and treatment measures, as well as keeping detachment from practices based on myths, tradition and common sense10-12.
By assessing the risk for development of PUs in individuals of a community, it was concluded that, frequently, the client, in its household, receives care actions from an informal caregiver, but it is a task of nursing professionals to guide and monitor these procedures. The nurse as a health professional must include the caregiver as the focus of its daily praxis and involve it as an integral part of caring, thus using health education and preparing it to preserve its health with a view to keeping a healthy life, so that it might take care of relatives or dear ones in an expressive way12.
It is understood by caregiver who has full or greater responsibility for the care shares provided to a dependent person, both within the household and in health institutions. The home care, in turn, is understood as the one developed with patients and family members in the context of their homes, aiming at the monitoring, treatment and rehabilitation of individuals, in response to their needs and the needs of their families11.
The informal caregiver suffers wear in its physical, emotional and social health, mainly due to the burden arising from the task of caring, since, in many cases, remains in full-time together with the person under care, and might provide essential information about the user's health status for the health team.
In foreign countries, this caregiver is the object of attention and researches; however, usually it is ignored in our country, being a portion that is not attended by the health system in force, which has not adequately visualized its importance in the recovery and rehabilitation of health of sick individuals13.
In Brazil, there is lack of resources and political structure to help the informal caregiver. Often, the community gives an insignificant value to this function, which is generally focused on a single person, consequence of the difficulties to diversify caregivers. Furthermore, it should be perceived the low production of researchers on this issue, partly due to the shortage or lack of partnerships to conduct studies or by the difficulty in glimpsing prospects for the use of such results12.
Thus, it is believed that knowledge of the socioepidemiological characteristics of these subjects might allow health professionals to think of new ways of operation and assistential technologies to meet the health needs of users, their relatives and caregivers, as well as the development of strategies that ease the achievement of self-care.
METHODOLOGY
It is a descriptive and cross-sectional study, with quantitative approach, performed in a Health District of Uberaba, Minas Gerais State. The project was approved by the Research Ethics Committee (REC) from the Federal University of Minas Gerais Triangle (UFTM), according to the Opinion nº 1.204/2008.
The sample consisted of 101 users and 95 caregivers, identified according to records of families in FHS units belonging to the aforementioned district, who agreed to participate in the study by signing the Free and Informed Consent Form (FICF).
Data collection was conducted through interviews and clinical examination, in the period from February to August 2010, during home visits. On the first visit, the objective was to know the socioepidemiological profile of the user with impaired physical mobility and of its caregiver. To that end, it was applied, together with the subjects, a tool consisting of two parts: the first consisting of demographic data (gender, age, color, work/occupation, schooling, family income, marital status and housing conditions) and the second composed of investigation regarding the presence of self-reported comorbidities, cause (s) of limited mobility, limitation time, level of dependency, risk assessment score of the Braden Scale, presence of PU (s) and its (their) location (s).
The research tool for collecting data of caregivers was composed of two parts: the first including sociodemographic data (gender, age, work/occupation, schooling and family income) and the second with identification data of the caregiver: degree of relationship with the user, distance from the user’s home, performed activities, care time, accomplishment or not of the PU (s) dressing (s).
At the second home visit, it was conducted the orientation of user, caregivers and family members, based on an educational booklet called Guidelines for people with impaired physical mobility, elaborated by professors and students who were members of the Wound League of the UFTM (LiFe-UFTM).
The data were organized in the spreadsheet of the program Microsoft Excel® and, then, the descriptive analysis thereof was held, with the statistical software Statistical Package for Social Science (SPSS), version 16.0.
RESULTS AND DISCUSSION
Health users
Of the 101 users, 54 (53,5%) were female, aged between 6 and 98 years and an average age of 62,12 years. The larger number of subjects, 63 (62,3%) is above the age of 60 years. White skin color was predominant, totaling 61 (60,4%) users.
Most users were elderly and female, which is justified by the fact that women, in Brazil, have longer survival than men. Population aging has been a global realty and, particularly, there is in our country, among many characteristics, the feminization of the old age13,14, as shown in Table 1.
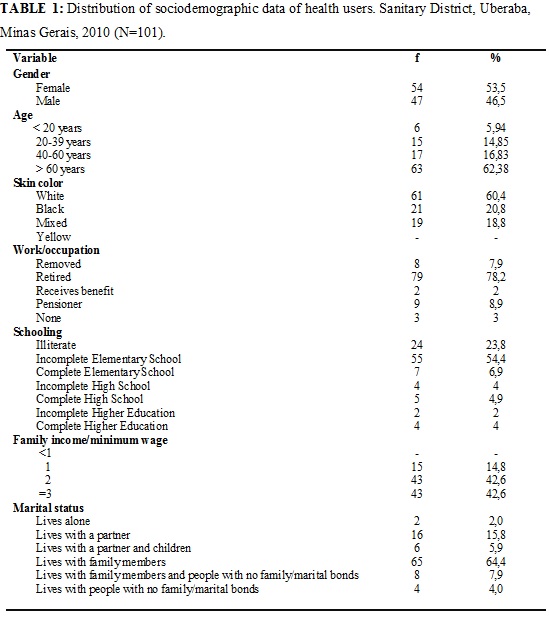
Regarding the work/occupation, 98 (97%) of subjects received government proceeds through retirement, benefits, sick-pay allowances or pensions, thus having, at that time, no occupation; 79 (78,2%) users were retired, while only 3 (3%) did not develop any activity and neither received any kind of proceeds.
The prevalent level of schooling was comprised of users with incomplete Elementary School, with 55 (54,4%) subjects, while 24 (23,8%) were illiterate. As for family income, 58 (57,4%) were receiving between 1 and 2 minimum wages.
Low income, coupled with the low level of schooling, provokes a negative impact on the ability to care of users, since there is involvement of environmental support, understood as physical, human and material resources to which people have access8.
Most of the time, restricted mobility disables the user for professional practices, resulting in a major expense, by the government, with the payment of pensions, allowances and benefits, in addition to requiring comprehensive care and constant health care shares15.
Only 2 (2%) subjects lived alone and 65 (64,4%) lived with family members. All users lived in brick houses, of which 96 (95%) had four or more rooms.
The presence of family in caring of the user was evident in this study. It is noteworthy to highlight that the relationship between the user and caregiver, which, in most cases, is a family members, must be reliable. Moreover, a favorable relationship must be established with the FHS team, thereby providing a good monitoring of the user with impaired physical mobility.
Regarding self-reported comorbidities, it was observed that 57 (56,4%) investigated users had systemic arterial hypertension (SAH) alone or associated to other chronic condition. Among them, the most common was diabetes mellitus, with 16 (28.7%) subjects, followed by Alzheimer's disease, with 3 (5,9%); 33 (32,6%) did not present any other morbid condition.
The World Health Organization (WHO) defines as chronic cardiovascular diseases (cerebrovascular and ischemic), neoplasms, chronic respiratory diseases and diabetes mellitus, and this list includes those diseases that contribute to the suffering of individuals, families and society at large, such as mental and neurological disorders, oral, bone and joint diseases, genetic disorders and eye and hearing pathologies16.
The complications arising from SAH and Type 2 diabetes mellitus compromise tissue perfusion, predisposing the individual to the development of PUs.
Chronic non-communicable and chronic health conditions, such as cerebral palsy and paraplegia, might also involve other deficits, such as emotional instability, depression, decreased tolerance to stressful situations and lack of cooperation in treatment, which puts patients at the risk for secondary complications17.
Several factors were causes of restricted physical mobility, and the most frequent was cerebral vascular accident (CVA), with 37 (36,6%) users, of which 34 (91,8%) were elderly.
As the second most frequent of the mentioned causes of limited mobility, there are car and motorcycle accidents, with 9 (8,9%) users, followed by cerebral palsy and femoral neck fracture, with 8 (7,9% ) subjects each. Investigations in similar conditions indicate the underlying disease itself as a causative factor of the limited mobility, especially those with neurological and musculoskeletal origins and CVA18.
For subjects aged between 20 and 59 years, there was predominance of car and motorcycle accidents as self-reported causes of limited mobility.
As for care dependence, 95 (94,0%) users were dependent or semi-dependent on caregivers, needing help in some daily life activities, such as body hygiene and for putting clothes, and showed a condition of impaired physical mobility for approximately 5 years. Only 5 (4,9%) subjects were independent and had no caregivers.
The limitation of the individual's ability to perform daily life activities, such as bathing, dressing, evacuate and urinate, eat, walk, sit, stand up without assistance, is a factor that contributes to the increased risk for developing PUs, which might be worsened by the lack of suitable interventions19.
By assessing the risk for the development of PUs according to the Braden Scale, 60 (59,4%) users showed moderate risk, 23 (22,8%) had high risk and 18 (17,8%) users have not revealed risk. Of total of users, 22 (21,8%) subjects had ulcers. Of these, 14 (63,6%) were elderly. In considering the subjects with ulcers, 11 (50,0%) showed high risk for the development of PUs, while the remaining 11 (50,0%) were classified as people with moderate risk.
The recognition of individuals at risk for PUs depends on the clinical skill of the professional and the use of appropriate assessment tools. Among these, the Braden Scale is considered the most appropriate tool, due to being a tool with predictive validity, with the largest number of assessment items and parameters with adequate specificities, and it is translated and validated for the Portuguese language19.
The decreased functional capacity in the elderly and the very physiology of the aging process contribute to increase the risk of developing ulcers. Accordingly, the aging process affects all healing stages, regardless of comorbidities that, alone, also interfere in the process of tissue repair20,21.
The sacral was the body region with highest prevalence of PUs, with 7 (31,8%) subjects, followed by the trochanteric region, with 5 (22,7%) subjects. Other 5 (22,7%) users have concomitantly shown ulcers in sacral and trochanteric regions.
Other studies also highlight these regions as body areas of excellence for the development of PUs, because of the greater presence of bony prominences associated to the dorsal positioning that is mainly held by the person bedridden or restricted to a wheelchair7,22-24.
Caregivers
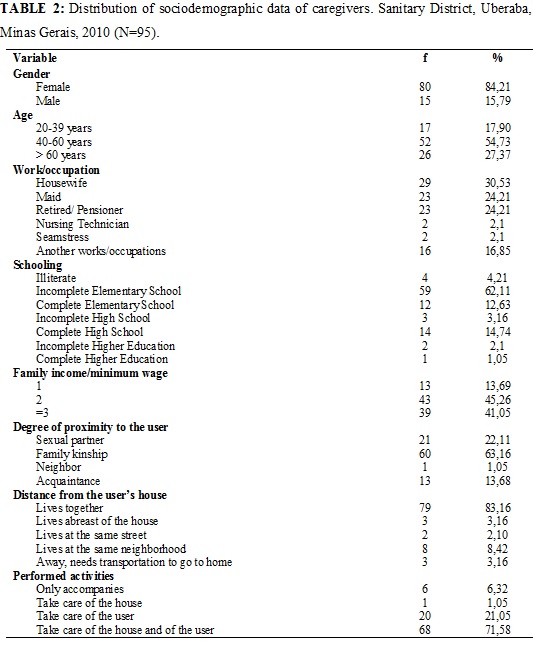
Participants were 95 (100%) caregivers, of which 80 (84,2%) were female. Most caregivers, 78 (82,1%), were aged over 40 years, of which, 26 (27,3%) had more than 60 years old, as shown in Table 2.
The predominance of women in care shares, also realized in other studies, stems from historical and social trends, which reproduce the female figure as the main responsible for health care procedures within the home. Women received this cultural and social role of caring for children, husbands and family members. Women have been considered generators of care and, to exercise such care, organize themselves, make internal arrangements, leaving other activities, generally asking for help from other women and, in that way, assuming control of situations, especially in cases of diseases and of daily care shares with small children and elderly people8,18,25,26.
In relation to work/occupation, 29 (30,5%) caregivers were housewives, not having their own income, 23 (24.2%) were maids, 23 (24.2%) were retirees/ pensioners, 2 (2,1 %) were nursing technicians, 2 (2,1%) were seamstresses and 16 (16,8%) had other varied occupations, such as a watchman, woodworker, secretary, among others.
The caregiver establishes an important link among the family, the user and the health services; however, there is lack of economic, social and health policies involving their valuation, the increase of their skills and the identification of their health needs, allowing it to take care of other people, without prejudice to its own self-care12,18,25.
The predominant level of schooling was incomplete Elementary School, with 59 (62,1%) caregivers. Only 1 (1,0%) caregiver had finished the Higher Education. The low educational level of the caregivers and the lack of specific training must be considered as important characteristics for the performance of nurses, with regard to the development of educational interventions along with this population. Many factors are closely related to the success of the therapeutic process, as the commitment of caregivers, the good relationship among the health care staff, patients and caregivers, as well as family and social supports27.
Regarding family income, 43 (45,2%) caregivers received, on average, two minimum wages. Concerning the degree of proximity to the user, it is noteworthy to emphasize that 60 (63,1%) caregivers had family kinship and 79 (83,1%) lived together with the user. Most caregivers, 68 (71,5%), besides to take care of the user, played other activities, such as household tasks of cleaning the house, preparing meals and washing clothes.
As for care time of the user, 64 (67,3%) caregivers were doing this function for 3 years or more. Of the 95 caregivers, only 17 (17,8%) performed PU dressings in the user. Of these, 14 (82,3%) did it two times a day, 5 (29,4%) of them considered like correct the way in which the bandage was held.
The findings point to the lack of qualifications of caregivers and the shortage of support for offering them, highlighting the importance of training activities and support from a multidisciplinary health team. Furthermore, they must provide health care for caregivers, taking into account that the activity of caring of a dependent elderly subject is exhausting and involves health risks for whose takes care28.
CONCLUSION
The results of this study have shown that people restricted to beds or wheelchairs are mostly elderly, female, white, with a low level of schooling, family income between 1 and 2 minimum wages and live with family members. They showed a predisposition for the development of ulcers and were affected by multiple comorbidities, especially systemic arterial hypertension and Type 2 diabetes mellitus, besides other chronic conditions that lead to a decrease in the functional ability and the future need for care shares, thereby becoming dependent on assistance from caregivers.
As for the assessment risk by the Braden Scale and presence of PUs, the surveyed subjects showed lower scores, meaning a higher risk for developing ulcers and a higher prevalence of these disorders in the sacral region.
As for caregivers, there was predominance of female, aged between 40 and 60 years, housewives, with incomplete Elementary School, family income equal to 2 minimum wages, family kinship with the users and residents with these subjects, being responsible for the care of homes and users for a period greater than 3 years.
As limitation of this study, one could highlight the fact that the survey was conducted only in a Sanitary District of Uberaba. The findings represent only a portion of the population served by the teams of the Family Health Strategy of the municipality at stake, highlighting the need that further studies like this are also developed in two other districts of Uberaba, so that one might expose a broader reality of situation of the municipality.
It is believed that the teams of the Family Health Strategy and the health services must provide support for users with impaired physical mobility, their family members and caregivers, through a permanent and continuous process of health education that respects the needs, limitations and skills of each person and fosters an empowerment of these subjects for the self-care, with safety and quality, as well as social and family interaction.
REFERENCES
1. Ministério da Saúde (Br). Portaria 2.527 de 27 de outubro de 2011. Redefine a Atenção Domiciliar no âmbito do Sistema Único de Saúde. Brasília (DF): Editora MS; 2011.
2. Fernandes JM. O papel do cuidador frente ao paciente acamado e a responsabilização da equipe de saúde da família. [monografia]. Araçuaí (MG): Universidade Federal de Minas Gerais; 2010.
3. Costa AJL. Metodologias e indicadores para avaliação da capacidade funcional: análise preliminar do Suplemento Saúde da Pesquisa Nacional por Amostra de Domicílios – PNAD, Brasil, 2003. Ciênc saúde coletiva. 2006; 11:927-40.
4. Parahyba MI, Veras R. Diferenciais sociodemográficos no declínio funcional em mobilidade física entre os idosos no Brasil. Ciênc saúde coletiva. 2008; 13:1257-64.
5. Costa AGS, Oliveira ARS, Alves FEC, Chaves DBR, Moreira RP, Araujo TL. Diagnóstico de enfermagem mobilidade física prejudicada em pacientes acometidos por acidente vascular encefálico. Rev esc enferm USP. 2010; 44:753-58.
6. Diagnósticos de enfermagem da NANDA: definições e classificação 2009-2011. Porto Alegre (RS): Artmed; 2010.
7. Chayamiti EMPC, Caliri MHL. Úlcera por pressão em pacientes sob assistência domiciliária. Acta Paul Enferm. 2010; 23:29-34.
8. Brito MAGM, Bachion MM, Souza JT. Diagnósticos de enfermagem de maior ocorrência em pessoas com lesão medular no contexto do atendimento ambulatorial mediante abordagem baseada no modelo de Orem. Revista Eletrônica de Enfermagem. [Internet]. 2008; [citado em 20 mai 22013] 10:13-28. Available at: http://www.fen.ufg.br/revista/v10/n1/v10n1a02.pdf.
9. Figueiredo MLF, Luz MHBA, Brito CMS, Sousa SNS, Silva, DRS. Diagnósticos de enfermagem do idoso acamado no domicílio. Rev Bras Enferm. 2008; 61: 464-9.
10. Araújo CRD, Lucena STM, Santos IBC, Soares MJGO. A enfermagem e a utilização da Escala de Braden em Úlcera por Pressão. Rev enferm UERJ. 2010; 18:359-64.
11. Fernandes LM, Caliri MHL, Haas VJ. Efeito de intervenções educativas no conhecimento dos profissionais de enfermagem sobre prevenção de úlceras por pressão. Acta Paul Enferm. 2008; 21:305-11.
12. Souza LM, Wegner W, Gorini MIPC. Educação em saúde: uma estratégia de cuidado ao cuidador leigo. Rev Latino-Am Enfermagem. 2007; 15:337-43.
13. Rech V, Teixeira L, Sachetti A, Fontana C, Romano A. Pressão arterial após atividades físicas orientadas em idosos hipertensos. SaudPesq. 2013; 6:75-83.
14. Tavares DMS, Martins NPF, Diniz MA, Dias FA, Santos NMF. Qualidade de vida de idosos com hipertensão arterial. Rev enferm UERJ. 2011; 19:438-44.
15. Marques GQ, Freitas IBA. Experiência-piloto de assistência domiciliar: idosos acamados de uma Unidade Básica de Saúde. Rev esc enferm USP. 2009; 43: 825-32.
16. World Health Organization. Global status report on non communicable diseases 2010. Geneva (Swi): WHO; 2011.
17. Smeltzer SC, Bare BG. Brunner & Suddarth: Tratado de enfermagem médico-cirúrgica. 10ª ed. Rio de Janeiro:Guanabara Koogan; 2008.
18. Pimenta GMF, Costa MASMC, Gonçalves LHT, Alvarez AM. Perfil do familiar cuidador de idoso fragilizado em convívio doméstico da grande Região do Porto, Portugal. Rev esc enferm USP. 2009; 43:609-14.
19. Lucena AF, Santos CT, Pereira AGS, Almeida MA, Dias VLM, Friedrich MA. Perfil clínico e diagnósticos de enfermagem de pacientes em risco para úlcera por pressão. Rev Latino-Am Enfermagem. 2011; 19:523-30.
20. Stotts NA, Hopf HW. Facilitating positive outcomes in older adults with wounds. Nurs Clin North Am. 2005; 40: 267-79.
21. Souza DMST, Santos VLCG. Incidência de úlceras por pressão e fatores de risco em idosos institucionalizados. Estima. 2006; 4:45.
22. Achutti A, Azambuja MIR. Doenças crônicas não transmissíveis no Brasil: repercussões do modelo de atenção à saúde sobre a seguridade social. Ciênc saúde coletiva. 2004; 9: 833-40.
23. Irion G. Feridas: novas abordagens, manejo clínico e atlas em cores. Rio de Janeiro: Guanabara Koogan; 2005.
24. Costa MP, Sturtz G, Costa FPP, Ferreira MC, Barros Filho TEP. Epidemiologia e tratamento das úlceras de pressão: experiência de 77 casos. Acta Ortop Bras. 2005; 13:124-33.
25. Moreira MD, Caldas CP. A importância do cuidador no contexto da saúde do idoso. Esc Anna Nery. 2007; 11:520-5.
26. Thober E, Creutzberg M, Viegas K. Nível de dependência de idosos e cuidados no âmbito domiciliar. Rev Bras Enferm. 2005; 58:438-43.
27. Abrahão SS, Ricas J, Andrade DF, Pompeu FC, Chamahum L, Araújo TM. Estudo descritivo sobre a prática da diálise peritoneal em domicílio. J Bras Nefrol. 2010; 32:45-50.
28. Rocha MPF, Vieira MA, Sena RR. Desvelando o cotidiano dos cuidadores informais de idosos. Rev Bras Enferm. 2008; 61:801-8.