FIGURE 1: Important aspects to have quality of life from the perspective of the elderly with cancer: meaning of life. Petrópolis, Rio de Janeiro, 2011.
ORIGINAL RESEARCH
Quality of life from the perspective of older adults with cancer: primary care nursing implications
Jefferson Afoncio da SilvaI; Cristina Gonçalves Hansel II; Jaqueline da SilvaIII
I
Nurse. Specialist. Coordinator of the Surgical Center Unit and Central of
Materials of Clinics Hospital of Imperatriz. Maranhão, Brazil. E-mail: jeffersonafoncio@me.com
II
Nurse. Doctor. Professor of the Undergraduate Course of the Arthur de Sá
Earp Neto and the Faculty of Medicine of Petrópolis. Rio de Janeiro,
Brazil. E-mail:
cristinahansel@yahoo.com.br
III
Nurse. Doctor. Professor at the Graduate program of Anna Nery Nursing
School. Rio de Janeiro, Brazil. E-mail: jackiedasilva@hotmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2016.9621
ABSTRACT
Objective: to examine quality of life from the perspective of older adults with cancer in primary care. Method: this quali-quantitative study, with data collected through documentary research and interview, from May to July, 2011 at a teaching outpatient unit in Petrópolis, Rio de Janeiro, was approved by research ethics committee (No. 05-2011). From 54 patient files meeting the inclusion criteria, eight older adults answered qualitative questions; data were submitted to descriptive and content analysis. Results: among all older adults seen at the facility, 54 (29.8%) had a confirmed diagnosis of cancer. Core elements highlighted in quality of life were: live well and be happy, pointing out that a cancer diagnosis brings changes in life and in quality. Conclusion: for older adults with cancer, quality of life is multidimensional and constitutes a central challenge to nursing, in developing care plans and interventions that foster patient proactivity and promote potentialities.
Keywords: Elderly; cancer; nursing; primary health care.
INTRODUCTION
Increased life expectancy and population aging are phenomena of global interest and are associated with reduced fertility rates, technological and social advances in health which had resulted in the progressive aging of the population of the world1 and of Brazil2. Thus, population aging is an emerging challenge to public health worldwide with respect to population growth, morbidities, disabilities and use of services and resources.
Statistics indicate that the proportion of young people has fallen and of older people has increased in the Brazilian population. The population aged above 65 years, which was 4.8% in 1991, passed to 5.9% in 2000 and reached 7.4% in 2010² and this fact becomes evident in the progressive enlargement of the top of the age pyramid. At a time of transition from the first to the second decade of this century, partial data published by the Ministry of Health for the year 2012 point to an important growth. In 2010, the elderly accounted for the 10.8% of the whole population. In turn, in 2012, the elderly population showed an increase of at least 3%³.
The study of specific segments such as the group of elderly patients with cancer in the periods of 2010-2012 and 2010-2014 shows even more significant increases regarding the demand for hospitalization; an increase of 16.15% was observed in two years (208,861 in 2010 to 242,605 in 2012), and 24.69% in four years (from 208.861 in 2010 to 260,448 in 2014). Therefore, a clear picture of the socio-demographic reality of Brazilian health is seen and this requires multidimensional demands for healthcare and research priorities.
The significance of the data justifies the importance and necessity of carrying out research studies and disseminating their contributions, aligned and in compliance with the combined priorities of research in nursing; contextualized and guided by social demands and priorities of the National Agenda for Research Priorities in Health (NARPH), in particular non-communicable diseases, highlighting neoplasms; it is worth mentioning also the health of the elderly, with the item - Magnitude, dynamic and understanding of health problems of elderly people, and the sub-items - evaluation of the quality of life the elderly and - studies on alternative care to improve the quality of life of the elderly population; and in line with the National Policy for the elderly5.
Thus, based on the significance of the data, of social care demands and of research priorities, the present study aimed to analyze the quality of life from the perspective of elderly patients with cancer assisted in primary care.
LITERATURE REVIEW
In demographic terms, population aging is not related directly to individuals, or to one generation. It is related to changes in the epidemiological profile, with the age structure of each population group, which determines the onset of aging of a country, or even a city. It varies from society to society and depends on the influence of multiple factors such as biological, economic, social and cultural factors1.
The aging of individuals of a given population is linked to a growing number of health problems5. Thus, it is up to society and to the scientific nursing community to assess and discuss the political, socio-demographic and health demands of the population.
As natural process, the aging of each individual has particular characteristics. Life itself exposes the person to events that have an impact on their physical, cognitive-behavioral and emotional health and quality of life. Likewise, subjects in advanced stages of aging are more likely to develop imbalances in their health. In this sense, although chronic diseases may not be fatal, they certainly compromise the quality of life of elderly people in different degrees2,5,6.
Fragilities, and emerging biological and social imbalances have greater impacts in the daily life of individuals that are in advanced stages of the aging process. Thus, the high incidence of chronic diseases in this group is associated with the greater fragility of the physical body and also to the environment to which they are exposed, which significantly influences their quality of life6,7.
According to the Ministry of Health, among chronic diseases, the cardiovascular and recurrent respiratory diseases and diabetes II were the ones that most affected elderly people by the end of the nineteenth century8. However, in the early twenty-first century, cancer begun to show a particularly significant increase in hospital admissions, and now represents the second cause of death among elderly8,9.
As a phenomenon of diverse complexity and strong impacts of social and economic nature at the population level, cancer causes physical and psychological changes in individuals of different age groups10 and may bring long periods of morbidity and result in impacts that compromise the autonomy, functional independence and quality of life of the elderly6,7,10,11.
As an example of what occurs in the context of chronic diseases, cases of cancer require from health professionals that they offer competent technical support adequate to the continuum of the different levels of care12. Keeping the health balance of the elderly and ensuring good quality of life are protective factors for full longevity and certainly represent a challenge at the macrossystemic level of public policies involving global and national gerontology and at the microssystemic level, encompassing communities, health facilities and families11,13-15.
However, the definition of what is quality of life is varied, broad, complex and should not be solely related to the presence or absence of disease, but also to the socioeconomic and cultural context in which the individual is inserted16. For the World Health Organization, quality of life is "an individual's perception of his position in life in the context of culture and system of values, in which he lives and in relation to his goals, expectations, standards and concerns"17: 583.
The national recommendation of researchers is that services use strategies appropriate to the health needs of the elderly population18, pointing out that:
Although the basic needs of the elderly are the same for anyone anywhere in the world or at any human development stage, some issues of social, physical and mental health, as well as daily life activities related to autonomy, functional independence, and cognitive function interfere decisively in the quality of health8:82.
However, to maintain a good quality of life, it is imperative to develop effective care strategies in the different levels of attention to the health needs of the elderly, especially of the potentially more vulnerable, such as those with cancer. Therefore, researchers and professionals can increase the robustness of the body of knowledge and health care by using and enjoying the voice of experts on the topic elderly with cancer and in assistance to their health in primary care units.
METHODOLOGY
Quantitative and qualitative study with data collected through the techniques of documentary survey and interview, and subjected to content analysis. Inclusion criteria determined: 60 or more yearsof age; clinical diagnosis of cancer; havemedical record in the institution of study and be under monitoring of the state of health in primary care. Exclusion criteria were self-identification of severe depression and/or mild to severe cognitive impairment. Data collection was conducted from May to July 2011, in the teaching unit located in the city of Petrópolis, Serrana region of the state of Rio de Janeiro, Brazil.
This study was approved by the Ethics Committee of the Faculty Arthur de Sá Earp Neto and the Faculty of Medicine of Petrópolis, under the Presentation Certificate for Ethics Assessment (CAAE) number 05-2011, in view of the Resolution of the National Health Council (CNS)19, in force at the time of submiting this project.
After invitation and explanation of the objectives of the study, the Informed Consent (IC) was read and signed in two copies by the eight participants at the moment of starting the collection of qualitative data. In order to maintain anonymity, participants were identified by the vowel I followed by the serial number of the interviews.
In the quantitative study, in the documentary survey, sociodemographic and clinical data were collected from 54 medical records of elderly diagnosed with cancer and these were inserted in spreadsheets of Excel software®. Data were processed and analyzed using descriptive statistics. In the qualitative study, interviews were carried out through a semistructured script to collect data on quality of life. The interviews were transcribed, checked, organized and treated observing the recommendations of Bardin20.
The examination of qualitative data occurred in three phases. At first, they were organized systematically and indicators were established for interpretation. In the second phase, the material was explored through successive cuttings into record units, with coding, classification and reorganization of information in themes. In the third phase, the treatment, inference and interpretation of results took place through juxtaposing the categories analyzed and highlighting similarities and differences, leading to the central categories of the study.
RESULTS AND DISCUSSION
Quantitative analysis
Quantitative data obtained from the documentary analysis of the statistics of the institution and the medical records for the year 2010 showed 2,562 outpatient visits to persons aged at 18 years and older than this, mostly women with 966 (37.8%) counting 60 and more years of age. In the year in the screen, among all the 181 (7%) people with clinical diagnosis of cancer indicated in their records, 54 (29.8%) were elderly.
For the analyzed period, the characterization of the elderly with cancer showed the presence of 31 (57.4%) women and 23 (42.6%) men, with age distribution of 27 (50%) people between 60 to 69 years of age, 17 (31% ) people between 70 and 79 years of age, and 10 (19%) people between 80 and 90 years of age. In studies on analysis of neoplastic disease diagnosis in the elderly, 67 types of cancer were identified, 42 (77.8%) in the digestive organs, which was the type of cancer mostly in women21,22.
The methodological challenge to be reported, that is, the reduced number of 8 (14.8%) testimonies out of 54 (100%) elderly undergoing monitoring and with diagnosis of cancer, was due to the high rate of missed consultations.
In this group of eight respondents, six (75%) were aged between 60 and 69 years, and among them five (62.5%) were men, six (75%) were married, seven (87.5%) were living with the family and seven (87.5%) received some type of financial support from the government.
The large number of women, 31 (57.4%), observed in this study may be associated with cultural factors such as low demand for preventive health care by Latin-american men23. However, men, when they have any symptoms or if there is already an installed and known pathology, in this case they are more assiduous and have greater adherence to treatment 23,24. Therefore, the data from the survey are associated to cultural and gender aspects identified in studies on the health of Brazilian man in primary care.
Among the 54 (100%) medical records of elderly patients with cancer, seven (87.5%) clients had cancer in digestive organs, specifically gastric cancer, followed by one (12.5%) case of malignancy of the skin. Among other comorbidities, there were four (50%) confirmed diagnosis of systemic arterial hypertension (SAH) and four (50%) of Diabetes Mellitus (DM) type I and II.
Qualitative analysis
The organization, analysis and separation by similarities and differences resulted in two main categories of study - Meaning of life and Difficult paths after the unexpected - presented according to the clippings of the statements.
Category 1: Meaning of life
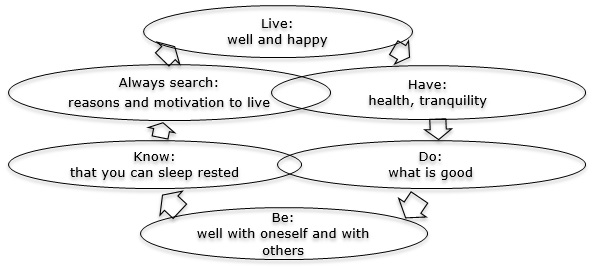
When asked about what is quality of life in their perspectives and what they considered to be important to have quality of life, the elderly said: these are actions to be healthy and tranquil; doing good; being well with themselves and with others; and being able to: sleep soundly; always have: reasons and motivation to live, aligned with a central goal that is to live well and happy, represented in Figure 1.
FIGURE 1:
Important aspects to have quality of life from the perspective of the
elderly with cancer: meaning of life. Petrópolis, Rio de Janeiro, 2011.
In their responses, the elderly consider important the care starting from disease prevention up to the maintenance of health, with adequate food, physical activity and healthy ways to continue life, facing cancer. They highlighted the presence of the family as something that directly contributes to a good quality of life.
Living well with the family. (I3)
Being happy, joyful, spontaneous, having the will to live. (I1)
In the practice of the work in outpatient clinics, the presence of the family is fundamental and necessary to provide support and security to the person that is undergoing treatment, including the treatment of cancer. In the literature, the family is described as an inherent relation of the human being, which he is part, also at the time of the disease when a closer presence of meaningful people is required to cope with the difficulties experienced. In the relationship of help, family support for the elderly with cancer results in strength to cope with the disease, contributes to increased security and tranquility, promotes comfort throughout the post-diagnosis path, including the hospital stay or return to home, and the quality of life23-26.
Answers to open research questions corroborate the literature, where is shown that quality of life is the sum of subjective sensations that are related to well-being, whether physical or mental. Still, expressions such as happiness, better living conditions and satisfaction of living are commonly used to express quality and quality of life27,28. Continuing the testimonies, participants pointed out aspects related to the physical, mental and economic conditions of the elderly with cancer as essential to maintain or achieve quality of life.
Health, tranquility, involving everything, from the emotional to the financial aspects. (I2)
Proper nutrition, exercise to maintain health. (I8)
The perspectives of the elderly are in line with a study where the quality of life was considered an indicator of health. Through it, forms of validation are sought based on the general physical condition, functional capacity to work, development of domestic activities and social interaction in the environment they live29. Whether at work or in family, in addition to the cognitive functions in relation to the concentration and emotional state, the participants highlighted financial demands and challenges beyond the physical and emotional signs that a chronic illness, such as cancer, may bring.
In fact, given the multidimensional character that the quality of life may have for an individual or for the group of elderly people, the statements refer to a view no longer restricted to the absence of disease, but an expanded view that include at least six areas: physical, psychological, level of independence, social relationships, environment and spirituality30.
Category 2: Difficult paths after the unexpected
In this category were grouped the answers about the meaning of having cancer and the change in quality of life after the confirmation of the diagnosis. The responses to questions showed two paths permeated by subjective pain and the process of building resilience of the participants, schematically represented in the Figure 2.
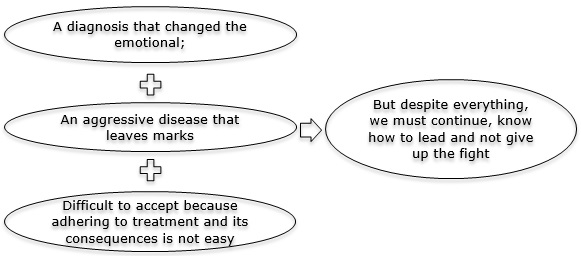
FIGURE 2:
Trajectory and quality of life from the perspective of the elderly with
cancer: difficult paths after the unexpected. Petrópolis, Rio de Janeiro,
2011.
About what is like to have cancer, the majority of the participants said that it is bad, uncomfortable, unacceptable, horrible - that it is impossible not to feel shaken. The participants added that the diagnosis of cancer changed their emotions; it expressed an aggressive disease which leaves marks; it was not easily accepted, and it poses a great challenge to adhere to treatment and overcome its consequences. However, for the respondents, it is necessary to continue, knowing to go ahead, and not giving up the fight.
Unacceptable, I did not like. (I6)
It's bad, but we get used to it, we have to learn to take things as they are. (I4)
In the context of the study, data confirm the illness as a generator of crisis, changes and moments of disorganization in life, leading the elderly to face limitations, frustrations and losses. They add that, when the person receives the diagnosis of cancer, the person experiences feelings of loss, anxiety and depression. But the person also goes through experiences that, when shared, may significantly contribute to the reduction of suffering and to aid health professionals in treating other people suffering from the same disease 31,32.
The testimonies allowed to observe changes in the quality of life of the elderly, from the diagnosis of cancer onwards, when the activities of daily living, once common and easy, are no longer developed as before. The answers showed that after the diagnosis of cancer, the development of daily activities become more difficult, with physiological and psychosocial effects, particularly the increase of the demand for care.
Yes, I stopped sewing and doing housework. (I5)
Little, weight loss and an inability to do things that are common in the work. (I8)
Despite all the technological, biochemical and pharmaceutical advancements and effective treatments, such as the gold line in the customer care to patients with cancer, concrete discomforts and difficulties persist ad interfere with activities of daily living. The statements reiterated that the necessary chemotherapy, causing fatigue, nausea, vomiting, changes in taste and bowel function, results in changes in the eating habits and makes it difficult to follow a normal healthy diet33,34, further compromising the immunity and because of the comprehensive care to those who also have other comorbidities such as hypertension and diabetes.
Therefore, adverse effects of therapeutic resources for cancer may have a negative influence on the quality of life of the elderly35,36.
CONCLUSION
It was possible to analyze the perspective of the elderly regarding the effect of the treatment of cancer on the quality of life. A complex theme, the quality of life can vary significantly between individuals and cultures. For the respondents, quality of life is achieved through intrinsic actions, self-determined, such as searching for good reasons to live with the treatment of cancer; implementing preventive actions to health in order to keep carrying out daily activities that are not necessarily basic activities of daily living; and maintaining mental health through active search for the will to live with inner peace, with joy and well with life.
The statements showed the diagnosis of cancer as a milestone that caused multidimensional impressions in the lives of the participants. Even in a delicate physical and emotional situation, the elderly with cancer, despite undergoing treatment, tried to find reasons to move on and maintain a balanced health and quality life.
In this context, nursing has as a central challenge the development of a multidimensional, stimulating and constructive care plan, transcending the maintenance of basic daily activities towards meaningful activities for each client, that may promote and facilitate the best possible quality of life for these elderly.
Among the study's limitations are the small number of respondents; the sampling by convenience that was composed by clients of only one health unit; and the high rate of missed consultations, which may refer to new questions about the seriousness of the health status and quality of life of the missing patients.
Although advances in science and technology keep causing a significant difference in the health and the quality of life of the elderly with and without cancer, new care demands continue to emerge from the perspectives of different people and groups. Therefore, for purposes of comparison and contrast of results, it is recommended to replicate the study with a representative sample of the universe.
REFERENCES
1.United Nations. Department of economic and social affairs, population division world population ageing 2013. ST/ESA/SER.A/348. [cited in 2015 Nov 25] Available from: http://www.un.org/en/development/desa/population/publications/pdf/ageing/worldpopulationageing2013.pdf
2.Instituto Brasileiro de Geografia e Estatística. Censo demográfico de 2010. [cited in 2015 Nov 21] Available from: http://www.brasil.gov.br/ciencia-e-tecnologia
3.Instituto Brasileiro de Geografia e Estatística. Censo demográfico de 2010. Departamento de população e indicadores sociais, 2010. [cited in 2015 Nov 22] Available from: http://www.ibge.gov.br/home/estatistica/populacao/censo2010
4.Oliveira DC. Prioridades de pesquisa em enfermagem e as linhas de pesquisa: dando continuidade ao debate. Rev enferm UERJ. 2014; 22(5):712-6. [cited in 2015 Nov 25] Available from: http://dx.doi.org/10.12957/reuerj.2014.12771
5.Ministério da Saúde (Br). Departamento de ciência e tecnologia. Agenda nacional de prioridades de pesquisa em saúde / Ministério da Saúde, Secretaria de ciência, tecnologia e insumos estratégicos, 2ª ed. Brasília (DF): Ministério da Saúde; 2008. [cited in 2015 Nov 25]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/agenda_nacional_prioridades_2ed_3imp.pdf
6.Oztürk A, Simşek TT, Yümin ET, Sertel M, Yümin M. The relationship between physical, functional capacity and quality of life (QoL) among elderly people with a chronic disease. Arch Gerontol Geriatr. [periódico na internet] 2011 [cited in 2011 Nov 23]. 53(3):278-83. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21215469
7.Da Silva J. Estar e ser idoso: aspectos geriátricos e gerontológicos. In: Figueiredo NMA, Tonini T, organizadoras. Gerontologia: atuação da enfermagem no processo de envelhecimento. São Caetano do Sul (SP): Yendis; 2006. p. 73-110.
8.Ministério da Saúde (Br). Secretaria de vigilância em saúde. Plano de ações estratégicas para o enfrentamento das doenças crônicas não transmissíveis no Brasil 2011-2022. Brasília (DF): Ministério da Saúde; 2011. [cited in 2015 Nov 20]. Available from: http://portalsaude.saude.gov.br/index.php/
9.Da Silva J., Chernicharo IM. Assistência de enfermagem ao idoso com diabetes, hipertensão e dislipidemia. In: Costa ALJ, Siewert JS, Torres MJF. Programa de atualização para técnicos de enfermagem (PROTENF). Ciclo 8. Porto Alegre (RS): Artmed Panamericana; 2015. p.61-116.
10.Marta GN, Del Nero LG, Nader MG, Mangabeira A, Critchi G, Kovács MJ, et al. Treatment priorities in oncology: do we want to live longer or better? Clinics [Internet] 2014 [cited in 2015 Nov 26]; 69(8): 509-14. Available from: http://www.scielo.br/scielo.php
11.Brown DS, Thompson WW, Zack MM, Arnold SE, Barile JP. Associations between health-related quality of life and mortality in older adults. Prev Sci. 2015 [cited in 2015 Nov 26]. Available from: http://www.ncbi.nlm.nih.gov/pubmed
12.Motta CCR, Hansel CG, Silva, J. Perfil de internações de pessoas idosas em um hospital público. Rev. Eletr. Enf. [Internet]. 2010 [cited in 2015 Nov 25]; 12(3):471-7. Available from: http://www.revistas.ufg.br/index.ph
13.World Health Organization. Noncommunicable diseases country profiles 2014. Geneva, Switzerland: WHO; 2014 [cited in 2015 Nov 25]. Available from: http://www.who.int/nmh/publications/ncd-profiles-2014/en/
14.Moliterno ACM, Faller JW, Borghi AC, Marcon SS, Carreira L. Viver em família e qualidade de vida de idosos da universidade aberta da terceira idade. Rev enferm UERJ. 2012 [cited in 2015 Nov 25]; 20(2):179-84. Available from: http://www.e-publicacoes.uerj.br/index.php
15.Zapponi ALB, Tocantins FR, Vargens OMC. O enfermeiro na detecção precoce do câncer de mama no âmbito da atenção primária. Rev enferm UERJ. 2015 [cited in 2015 Nov 25]; 23(1): 3-8. Available from: http://www.facenf.uerj.br/v23n1/v23n1a06.pdf
16.Da Silva, J. Motivation for self-care in older women with heart disease and diabetes: A balancing act [doctoral thesis]. San Francisco (USA): University of San Francisco; 2003.
17.Organização Mundial de Saúde. Conceito de qualidade de vida: versão em português dos instrumentos de avaliação de qualidade de vida (WHOQOL) 1998. Geneva (Swi): WHO; 2002. [cited in 2015 Nov 20] Available from: http://www.who.int/mental_health/publications/whoqol/en/
18.Honório GJS, Martins HEL, Bassol JF, Alvarez AM, Meirelles BS, Santos SMA. Estratégias de promoção da saúde dos idosos no Brasil: um estudo bibliométrico. Rev enferm UERJ. [periódico na internet]. 2013 [cited in 2014 Nov 20]; 21(1): 121-6. Available from: http://www.facenf.uerj.br/v21n1/v21n1a20.pdf
19.Ministério da Saúde (Br). Resolução nº 196 de 10 de outubro de 1996: Aprova as diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Brasília (DF): Ministério da Saúde; 1996.
20.Bardin L. Análise de conteúdo. Edição revisada e ampliada. São Paulo: Edições 70/Livraria Martins Fontes; 2011.
21.Ministério da Saúde (Br). Instituto Nacional do Câncer. Câncer no Brasil: dados dos registros de base populacional. Rio de Janeiro: Ministério da Saúde; 2011. [cited in 2015 Nov 19] Available from: http://www.inca.gov.br/estimativa/2012
22.World Health Organization. Women and health: today's evidence tomorrow's agenda. Organização Mundial da Saúde; 2009. [cited in 2015 Nov 30] Available from: http://www.who.int/ageing/mulheres_saude.pdf
23. Steptoe A, Shankar A, Demakakos P, Wardle J. Social isolation, loneliness, and all-cause mortality in older men and women. Proc Natl Acad Sci. 2013 [cited in 2016 Jan 25]; 110(15):5797-801. Available from: http://www.pnas.org/content/110/15/5797.full.pdf
24.Ministério da Saúde (Br). Política Nacional de Atenção Integral à Saúde do Homem. Brasília (DF): Ministério da Saúde; 2008. [cited in 2015 Nov 26] Available from: http://portal.saude.gov.br/portal/saude/area.cfm
25.Canieles IM, Muniz RM, Corrêa ACL, Meincke SMK, Soares LC. Rede de apoio à mulher mastectomizada. Rev Enferm UFSM. 2014 [cited in 2015 Nov 29]; 4(2):450-58. Available from: http://cascavel.ufsm.br/revistas/ojs-2.2.2/index.php/reufsm/article/view/10790/pdf
26.Souza MGG, Gomes AMT. Sentimentos compartilhados por familiares de pacientes oncológicos em tratamento quimioterápico: um estudo de representações sociais. Rev enferm UERJ. 2012 [cited in 2015 Nov 29]; 20(2): 149-54. Available from: http://www.e-publicacoes.uerj.br/ojs/index.php/enfermagemuerj/article/view/4009/2778
27.Melchiors AC, Correr CJ, Pontarolo R, Santos FOS, Souza RAP. Qualidade de vida em pacientes hipertensos e validade concorrente do Minichal-Brasil. Arq Bras Cardiol. [periódico na internet]. 2010 [cited in 2015 Nov 20]; 94(3):357-64. Available from: http://www.scielo.br/scielo.phps
28.Aragaki IMM, Silva IA. Percepção de nutrizes acerca de sua qualidade de vida. Rev esc enferm USP. [periódico na internet]. 2011 [cited in 2015 Nov 10]; 45(1):71-8. Available from: http://www.scielo.br/scielo.php
29.Oliveira AJM, Rios LR, Teixeira LS, Vieira FS, Mendes DC, Vieira MA, et al. Influência de fatores socioeconômicos na qualidade de vida de idosos hipertensos. Ciênc saúde coletiva. [periódico na internet]. 2014 [cited in 2015 Nov 30]; 19(8):3497-504. Available from: http://www.scielosp.org/scielo.php
30.Oliveira BM, Mininel VA, Felli VEA. Qualidade de vida de graduandos de enfermagem. Rev Bras Enferm. [periódico na internet]. 2011 [cited in 2015 Nov 21]; 64(1):130-5. Available from: http://www.scielo.br/scielo.php
31.Hartzler A, Pratt WJ. Managing the personal side of health: how patient expertise differs from the expertise of clinicians. J Med Internet Res. 2011 [cited in 2015 Nov 15]; 13(3):1728. Available from: http://www.jmir.org/2011/3/e62/
32.Souza JA, Fortes RC. Qualidade de vida de pacientes oncológicos: um estudo baseado em evidências. Revista de Divulgação Científica Sena Aires. 2012 [cited in 2015 Nov 30]; (2):183-92. Available from: http://revistafacesa.senaaires.com.br/index.php/revisa/article/view/30/25
33.Gozzo TO, Moysés AMB, Silva PR, Almeida AM. Náuseas, vômitos e qualidade de vida de mulheres com câncer de mama em tratamento quimioterápico. Rev Gaúcha Enferm. [periódico na internet]. 2013 [cited in 2015 Nov 30]; 34 enseñanza (3):110-16. Available from: http://www.scielo.br/pdf/rgenf/v3n3/a14v34n3.pf
34.Mansano-Schlosser TC, Ceolim MF. Fadiga em idosos em tratamento quimioterápico. Rev Bras Enferm. [periódico na internet]. 2014 [cited in 2015 Nov 30]; 67(4):623-9. Available from: http://www.scielo.br/pdf/reben/v67n4/0034-7167-reben-67-04-0623.pdf
35.Hansel CG. Envelhecimento do portador de transtorno mental institucionalizado: o viver e o cuidar dos profissionais de enfermagem de um hospital psiquiátrico [dissertação de mestrado]. Rio de Janeiro: Universidade Federal do Rio de Janeiro; 2008.
36. Kai J, Beavan J, Faull C. Challenges of mediated communication, disclosure and patient autonomy in cross-cultural cancer care. Br J Cancer. 2011 [cited in 2016 Jan 25]; 105(7):918-24. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3185938/