(*) two users declined to respond
Source: Direct research.
ORIGINAL RESEARCH
Care for people living with AIDS: focus on health education actions
Oriana Deyze Correia Paiva LeadebalI; Leidyanny Barbosa de MedeirosII; Kalline Silva de Morais LinsIII; Rebeca Bezerra ChavesIV; Aline Aparecida MonroeV; Jordana de Almeida NogueiraVI
I
Nurse. PhD. Adjunct Professor. Federal University of Paraiba. João Pessoa,
Brazil. E-mail: orianadcpl@gmail.com
II
Nurse. Master. PhD student. Federal University of Paraíba. João Pessoa,
Brazil. E-mail:
leidyannymedeiros@hotmail.com
III
Nurse. Specialist. Federal University of Paraiba. João Pessoa, Brazil.
E-mail: kallinemorais@gmail.com
IV
Nurse. Specialist. Master student. Federal University of Paraíba. João
Pessoa, Brazil. E-mail: rebeca.bz@hotmail.com
V
Nurse. Adjunct Professor. School of Nursing of Ribeirão Preto-USP. Ribeirão
Preto, Brazil. E-mail: amonroe@eerp.usp.br
VI
Nurse. Associate Professor. Federal University of Paraíba. João Pessoa,
Brazil. E-mail: jalnogueira31@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2017.9524
ABSTRACT
Objective: to examine the supply of health education actions in care for people living with AIDS. Method: a cross-sectional study was conducted with 150 people with AIDS at a specialized outpatient referral clinic in Paraíba State, using a structured form that contemplating nominal and interval variables. Data were collected from July 2011 to July 2012, after ethics approval of the project, and analyzed by descriptive statistics. Results: emphasis was found to be placed on aspects of health promotion regarding adherence to therapy, particularly the taking of antiretroviral drugs and preventing transmission of infection, but to the detriment of educational actions addressing defense of the social and reproductive rights of people in treatment. Conclusion: weaknesses in the provision of health education actions undermine the service users' skill-building for co-responsibility, autonomy and proactivity in caring for their health and controlling the infection.
Keywords: Acquired immunodeficiency syndrome; health promotion; health services; health education.
INTRODUCTION
In view of the chronic nature of the infection/disease, the care to people living with human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) requires interventions aimed at lifestyle changes, self-management of health, permanent follow-up, and offer of clinical management actions, which include the provision of antiretroviral therapy (ART) and other care measures to prevent complications, and psychosocial support in the face of the conflicts inherent to the condition of living with the infection1,2.
HIV/AIDS Special Assistance Services (SAS) represent an outpatient care modality that provides integral and quality care to the persons and their families, where a multiprofessional team offers diagnostic, treatment and prevention actions, including exams, medical check-up, distribution and control of ARV drugs, support to self-care, and educational activities to adhere to treatment and prevention of comorbidities3. Health education must be an indispensable activity in the care offered in these services with a view to the development, together with the users, of skills to improve their quality of life, and prevent complications associated with the infection and the antiretroviral treatment3.
It is known that the performance of teams with advanced communication skills and critical-reflexive potential fosters dialogic interactions in the construction of knowledge, motivation and skills for the self-management of health4. In the specialized outpatient service, where regular and prolonged contact between health professionals and users is required3, the provision of health education actions should be implemented as a precautionary action essential to the management of the infection/disease. Therefore, this study aimed to analyze the offer of health education actions in the care for people living with AIDS.
LITERATURE REVIEW
Since the beginning of the epidemic in Brazil, intense social mobilization has contributed to the formulation and implementation of public policies, which have given the country a prominent place in the world scenario, investing in technologies in the areas of diagnosis, internal production of antiretroviral drugs and prevention material5.
ART has significantly contributed to the improvement of the immune status of people under treatment, with repercussions on the clinical management of opportunistic diseases, increased survival and changes in the meaning of living with the infection, which has assumed a status of chronic condition and requires redirection of the health practices aimed at the infected persons1.
In the context of specialized care, assistance models and protocols have been reorganized with a view to ensuring universal access to diagnosis and timely treatment, early identification of opportunistic manifestations for appropriate clinical management, reduction of side effects and adverse effects of ART, and expanded offer of prevention actions aimed at people, families and communities which are considered vulnerable, or key populations2.
The importance of extended care beyond clinical management, the offer of technically oriented actions for adherence to ART and the monitoring of clinical and immunological conditions of the people under treatment are discussed in the field of professional training and performance. This has contemplated the unfolding of the infection/illness/treatment for the social life, which requires elements that transcend the biologic view and medical focus centered on a resolutive, integral care, with preventive interventions and health promotion6.
In the dialogical perspective of health education, one aspect of health promotion has as assumption the development of practices that value the active stance of the users and focus on the daily routine of living with the infection; the search to understand the determinants of the health-disease process and offer subsidies for the adoption of new habits and behaviors implicated in health4, fundamental to the prevention of secondary complications to viral pathogenesis and the side effects of ART.
It should be emphasized that health promotion in this context involves individual initiatives aimed at identifying risk factors for infection/illness/complications, requiring multidisciplinary, interprofessional and intersectoral action on social determinants of health and on the adoption of health styles, considering the expanded concept of health. Hence the importance to offer health education actions based on the understanding of the subjectivities and social dynamics of the human beings living with HIV/AIDS7.
METHODOLOGY
Cross-sectional study with quantitative approach developed in a specialized outpatient clinic, a reference in Paraíba for HIV/AIDS care, with a population of 1,260 people with AIDS reported in the National Disease Notification System (SINAN) from 1980 to 2011, older than 18 years and resident in the State.
Based on the calculation of samples for finite populations, significance level of 5%, sample error (d) of 0.8, confidence level of 95%, p value of 0.50, expression: n = Z2.p.q.N/d2 (N - 1) + Z 2.p.q, and correction for potential loss of 10%, the sample of 150 people living with AIDS, linked to the SAS, using ART for more than six months, were recruited for accessibility.
Data were collected from July 2011 to July 2012 through interviews using a structured form containing nominal variables and Likert-type response options, covering a sociodemographic characterization and offer of guidance on: family planning, sexuality and the use of condoms, food and nutrition, correct use and side effects of ARV drugs, reduction in the use of alcohol and other drugs, vaccines, information on participation in nongovernmental organizations (NGOs), and criteria/processes to request government benefits..
The instrument was submitted to content validation by the HIV/AIDS Operational Study Group of the Nursing School of Ribeirão Preto and to reliability analysis through the Cronbach's Alpha coefficient (= 0.789).
Data were analyzed using the Statsoft's Statistical Software 9.0 using frequencies and medians, attributing the indicator 5 to the most favorable answers on the scale and 1 to the most unfavorable answers. In the end, indicators 1 and 2 were considered unsatisfactory; 3, regular; and 4 and 5, satisfactory.
The project was approved by the Ethics Committee of the Federal University of Paraíba under protocol nº 612/10, and obeyed the ethical principles of research involving human beings.
RESULTS AND DISCUSSION
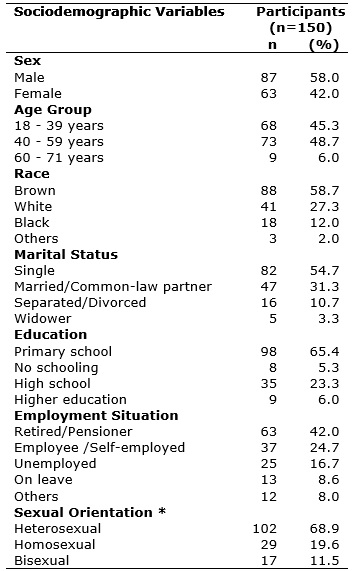
Among the participants, males (58%), aged 40 and 59 years (48.7%), with heterosexual orientation (68%) and brown skin color (58.7%) prevailed. It was also observed that the majority were single (54.7%), with education up to elementary school (65.4%), and retirees or pensioners (42%), as described in Table 1.
Table 1:
Distribution of people living with AIDS according to sociodemographic
variables. Specialized Outpatient Clinic, João Pessoa/PB, Brazil, 2012.
(*) two users declined to respond
Source: Direct research.
Regarding health education actions, the offers of family planning guidelines (51.7%) and information on NGOs in the state (75.3%) were considered unsatisfactory (median value equal to 1). The other variables were evaluated as a satisfactory offer, as shown in Table 2.
Table 2:
Median of the evaluation of the offer of health education actions in an
outpatient clinic specialized in the care of people living with AIDS. João
Pessoa/PB, Brazil, 2012
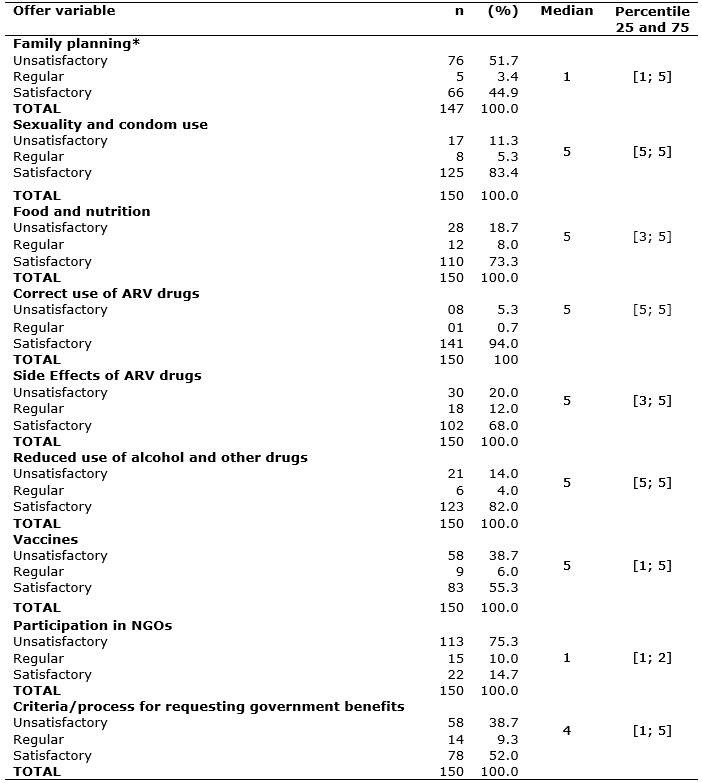
* Situations in which family planning guidelines applied (n = 147)
ARV- Antiretroviral
The sociodemographic characterization of the study participants is consistent with the epidemic transformations observed in the last two decades, corroborating the pattern of dissemination among heterosexual, low schooling and older individuals8.
The increase in the number of cases in men who declare to be heterosexual and the increase in transmission among women has made the heterosexual category as the main modality of exposure to infection8. In 2015, although homosexual exposure was more prevalent, from the total number of reported cases among males aged 13 years or older, 36.8% were heterosexual. Among women, this category accounted for 96.4% of the notifications9.
The current configuration of the epidemic corroborates the urgent need for understanding personal interactions, particularly the sociocultural construction of gender relations in the context of stable union. The sacredness of the family and marriage institutions has weakened the perception of vulnerability and contributed to the transmission of infection mainly among women, whose submission, dependence on their partners, denial/invisibility of their own sexuality represent elements of the feminine identity that impose challenges to preventive actions 10.
The percentage of people with low schooling corroborates the involvement of less educated and economically disadvantaged social strata, factors that are recognized as contributing to the phenomenon of pauperization of the epidemic11. Thinking about this supposedly causal perspective calls for the reflection on the qualification of care to meet the needs and singularities in this dimension.
The expressive percentage of older people draws attention to the need for policies based on the recognition of the existence and specificities of sexual practice at this life stage, on the incorporation of aspects of sexuality, gender, self-care and use of condoms in the practice of health professionals, in living spaces, home visits, and medical and nursing consultations12.
Although living with the disease brings major transformations, especially in affective-sexual relationships, the serological condition does not eliminate the sexuality of people with HIV/AIDS, nor does it prevent the occurrence of these relationships, either among serodiscordant people or otherwise. Therefore, access to information is imperative for conscious and responsible choices regarding the use of condoms, contraceptive methods and pregnancy planning. Besides the informative aspect, educational actions should stimulate the free expression and the experience of sexuality without violence, discrimination and impositions, to guarantee the exercise of the right of these people on the decision and the moment of generating children13,14.
In this perspective, the unsatisfactory classification of family planning guidelines is a fragility of the provision of expanded care by the service. Investment in professional qualification for family planning is necessary, transcending the reductionist perspective of contraceptive protection and ensures the reproductive right of the people being followed-up13 .
It is known that sexual and reproductive rights can be hampered by moral values of professionals who do not create opportunity for dialogue, compromising the preventive and integral quality of care, since reproduction usually involves sexual contact, corroborating the vulnerability of seropositive partners to reinfection; the vulnerability of seronegative partners and children to infection; and the exposure of the infected person to diseases and conditions that could potentially complicate their health status13.
Furthermore, the desire for expression and experiences of sexuality lies in a complex, individual field, surrounded by biological and historical-cultural factors that interfere with thinking, feeling and acting13.Therefore, sexuality deserves to be contemplated in the care health promotion in the context under analysis15.
The offer of guidelines on sexuality and use of condoms was evaluated as satisfactory by 83.4% of the users, with a median value equal to "5", suggesting a service that is sensitive to sexual rights. It should be emphasized that in addition to the transmission of information or distribution of materials, actions should be oriented considering the principle of freedom of choice, subjective individual aspects and respect for autonomy15,16.
Adequate food and nutrition, as a fundamental human right, are crucial to the well-being of people in general. In the context analyzed herein, food and nutrition have greater importance in result of the immunosuppressive repercussions of the infection, the clinical characteristics of AIDS and the influence on the possible adverse effects of ART14,17. Therefore, the satisfactory evaluation of 73.3% of the participants on the provision of guidelines related to food and nutrition represents a positive aspect. Information about healthy eating habits in special conditions (diarrhea, nausea and vomiting, weight loss, fever, lipodystrophy, among others) and on food hygiene and food safety, can contribute to the improvement of the quality of life of people in follow-up17,18.
Diarrhea and fever are common clinical manifestations of the progress of the disease, leading to reduced appetite, decreased nutrient absorption, malnutrition, weight loss, weakening, and increased vulnerability to opportunistic diseases/grievances. An adequate diet to the individual needs in addition to combating the aforementioned symptoms may contribute to increase CD4+ T lymphocytes and to combat the lipodystrophy syndrome (which characterizes the diagnosis and affects the self-image of people with AIDS), positively interfering on the response to treatment and reduction of financial expenses involved in its management14,17,18.
The existence of dietary restrictions associated with some ARV drugs also justifies the provision of guidelines on diet strategies capable of increasing the absorption of these drugs and reducing the side effects, so that people adopt healthier eating practices, with consequent impact on the response to treatment and improved health status19.
It is known that the effectiveness of ARVs in improving clinical conditions is directly related to adherence to ART, which in turn is influenced by how people overcome the complexity of a treatment that involves the continuous use of a varied number of doses and drugs, changes in lifestyle and side effects. These factors are in contrast with the benefits of using ARV drugs in various proportions, creating challenges for therapeutic adherence. Coping with these challenges involve the collaborative action of users, health professionals and family members, through an educational process in the micro space of care provision6. Hence, providing information that is adequate to users' level of understanding, on topics such as posology, schedules, drug interactions, possible adverse reactions and interaction between medications and feeding is important, as previously discussed20.
The offer of guidance on the correct use of drugs was rated by 94% of users as satisfactory. However, the negative evaluation of this aspect by 5.3% of the respondents reflects a failure of the specialized outpatient teams, which is responsible for the promotion of therapeutic adherence, an important step for achieving undetectable viral loads, considered a goal for control of infection20,21.
Educational actions focusing on therapeutic adherence should overcome the strictly prescriptive and controlling objectives of taking medication, and favor the building of bonds between the health team and the people living with HIV/AIDS. This is essential for decision making on the redefinition of routine/lifestyle considering the necessities inherent to the drug treatment, besides favoring the development of abilities and competences to control the own health and autonomy for self-care16.
In the perspective of health promotion, and without disregarding the duties of the State and society in meeting the needs of people living with HIV/AIDS, the autonomy and empowerment of the subjects should be optimized in order to improve their quality of life and health status16. Although not enough to ensure therapeutic adherence, access to information on medicines is a fundamental element of this autonomy.
Also in this context, the provision of guidelines on possible side effects/adverse effects of ARV drugs such as lipodystrophy syndrome, nausea, anorexia and headache, as well as measures to alleviate or reduce these events were evaluated as unsatisfactory or regular by 32% of participants, highlighting a gap in the care offered. Access to information on these topics is considered a right of the user and influences the onset of clinical complications and on therapeutic adherence14.
The use of psychoactive substances such as alcohol and other illicit drugs also predisposes to complications, compromises therapeutic adherence and negatively interferes with the effect of ART14. From the perspective of harm reduction, information should focus on the risk of exposure of drug users (DU) to reinfection or other infections such as those caused by hepatitis B virus (HBV) and hepatitis C virus (HCV) when there is no preventive behavior and preventive methods It is known that the use of certain drugs such as cocaine can potentiate the neurotoxicity of HIV, reduce the effects of certain drugs, either because of failure to take the doses as a consequence of the memory deficit caused by the drug, or by the reduction of the effect itself of the drug, or even by hepatotoxicity potentiated by the concomitant use of ARV, especially in the presence of HCV or HBV co-infection14.
The satisfactory evaluation of guidance on the use of alcoholic beverages and other drugs is a positive aspect of the service, considering the difficult to approach this issue in specialized care, as indicated by a study that mentions professional, personal and technical limitations that contribute to ignoring this issue and hampering the treatment of the patients22.
Also, in the perspective of prevention of opportunistic diseases, the provision of vaccine guidelines needs to be improved considering the existence of special vaccination schedules, as well as age, clinical and immunological parameters to be observed in decision making regarding immunization. In addition, it is known that compromised immunity affects immunogenicity and vaccine efficacy and has an effect on the risks of vaccines with attenuated live agents, aspects implied in the self-management of the health of people living with HIV/AIDS14.
In the scope of strategies to cope with AIDS in Brazil, an articulation of the civil society with health system services has taken place as result of political advances; as well as the implementation of comprehensive care and support measures for affected individuals, families and communities, with emphasis on the role of; NGOs in the creation of groups for adherence and exchange of experiences on living with HIV/AIDS; implementation of workshops to generate income, learn skills and works; the stimulation of awareness on the social rights of users, empowerment, and encouragement to the exercise of citizenship and autonomy23.
The unsatisfactory evaluation of the offer of guidelines on participation in NGOs by 75.3% of users, with the most negative score on the scale (p25 and p75 percentiles equal to 1 and 2, respectively) considering all variables studied highlights the need to approach this theme in order to optimize the access of people living with HIV/AIDS to these institutions, with respect to the voluntary decision of the target people to be linked to them.
It is also the responsibility of health professionals, through an educational process, to increase the access to public policies and the rights in force in the country in order to guarantee the health care and the right to a dignified life24, which includes the provision of information on care benefits and social security designed to support people who, due to illness, experience some level of temporary or permanent incapacity to work.
In this context, 52% of users evaluated the offer of guidelines on the criteria and process to apply for government benefits as satisfactory, while 38.7% evaluated the offer of this guidance as unsatisfactory, thus indicating a fragility of the service in promoting social justice 24.
CONCLUSION
Emphasis on the biological dimension in the care/clinical management/follow-up, especially in interventions aimed at promoting adherence to drug treatment and preventing the transmission, is directly related to the achievement of global goals of control of the epidemic. These aspects were highlighted as the main focuses of health education in the analyzed context because the following aspects were evaluated as satisfactory, in decreasing order: provision of guidelines on sexuality and use of condoms; correct use of drugs; reduced use of alcohol and other drugs; food and nutrition; side effects of drugs and vaccines.
The unsatisfactory evaluation of the provision of counseling on family planning as opposed to guidelines on sexuality and, above all, the use of condoms, strengthens the focus on the prevention of HIV/AIDS contagion, to the detriment of the reproductive rights of these people.
The regular and unsatisfactory assessment of the provision of information about the criteria and processes for applying for government benefits, although indicated by a smaller percentage of participants, also highlights a fragility of the assistance in the light of respect for the social right of these users, directly reflecting on their health conditions.
Gaps in the guidance on family planning, NGOs and, to a lesser extent, on government benefits, here considered as fragilities of the service in the guarantee of reproductive and social rights, hinder the consolidation of users as subjects capable of experiencing their health in a free, safe and responsible manner. Vulnerability, in the light of integral care, is therefore evident, with the potential to compromise the coordination of care, considering the relevance of the autonomous participation of users on their own health care. Actions to foster thoughtful reflection are necessary, as well as to encourage the persons living with HIV/AIDS to endeavor towards the necessary change to improve their quality of life.
The limitations of the study focus on the fact that the assessments only considered the perspective of the users of the service, specifically those living with AIDS, since the immediate treatment after diagnosis and regardless of the CD4 + TL count was instituted as a policy in Brazil after 2014, after the present data collection. Therefore, there is the possibility to explore the perspectives of the professionals and of the management, as well as to evaluate the indicators of outcomes on the object studied, and to expand the analysis to the experiences of people living with the infection and in treatment.
REFERENCES
1. Nunes AA, Caliani LS, Nunes MS, Silva AS, Mello LM. Profile analysis of patients with HIV/AIDS hospitalized after the introduction of antiretroviral therapy. Ciênc saúde coletiva [Scielo-Scientific Electronic Library Online] 2015 [cited on Nov. 30, 2016]. 20(10): 3191-3198. Available from: http://www.scielo.br/pdf/csc/v20n10/en_1413-8123-csc-20-10-3191.pdf
2. Figueiredo LA, Lopes LM, Magnabosco GT, Andrade RLP, Farias MF, Goulart VC, Scatena LM, Nogueira JA, et al. Offering health services and actions for the management of HIV/AIDS, from the perspective of users. Rev esc enferm USP [Scielo-Scientific Electronic Library Online] 2014 [cited on Sep. 15, 2017]. 48: 1026-34. Available from: http://www.scielo.br/pdf/reeusp/v48n6/pt_0080-6234-reeusp-48-06-1026.pdf
3. Abrão FMS, Angelim RCM, Cardoso MD, Queiroz SBA, Freitas RMM, Oliveira DC.
Structural and organizational characteristics of specialized HIV/AIDS care services in the city of Recife, Brazil. Rev baiana public health [Latin American and Caribbean Literature in Health Sciences] 2014 [cited on Sep. 15, 2017]. 38 (1): 140-154. Available from: http://files.bvs.br/upload/S/0100-0233/2014/v38n1/a4436.pdf
4. Reis RK, Melo ES, Galvão MTG, Gir E. Health education among people with HIV/AIDS: proposal for interdisciplinary intervention. Cienc Cuid Saude [Internet] 2014 [cited on Sep. 15, 2017]. 13 (3): 402-410. Available from: http://www.periodicos.uem.br/ojs/index.php/CiencCuidSaude/article/view/21120/pdf_179
5. Villarinho MV, Padilha MI, Berardinelli LMM, Borenstein MS, Meirelles BHS, Andrade SR.
Public health policies in the face of the AIDS epidemic and assistance to people with the disease. Rev Bras Enferm [cited on Sep. 18, 2017]. 66 (2): 271-277. Available from: http://www.scielo.br/pdf/reben/v66n2/18.pdf
6. Leadebal ODCP, Medeiros LB, Morais KS, Nascimento JA, Monroe AA, Nogueira JA. Risk management in providing specialized care for people living with AIDS. Rev esc enferm USP [Scielo-Scientific Electronic Library Online] 2016 [cited on Sep. 30, 2017]. 50(5): 838-845. Available from: http://www.scielo.br/pdf/reeusp/v50n5/pt_0080-6234-reeusp-50-05-0840.pdf
7. Guimarães HC, Borges MS, Souza MCS, Ribeiro MS. Promoting the health of HIV/AIDS patients in prisons applied to the nola pender model: a qualitative study. In: Minutes of the 6th Ibero-American Congress on Qualitative Research; 2017 Jul 12-14; Salamanca, Spain. Salamanca: CIAIQ; 2017. p. 421-430.
8. Furtado FMSF, Santos JAG, Loredanna S, Araújo E, Saldanha AAW, Silva, J. Thirty years later: social representations about AIDS and sexual practices of residents of rural cities. Rev Esc Enferm USP [SciELO-Scientific Electronic Library Online] 2016 [cited on Sep. 18, 2017]. 50 (spe): 074-080. Available from: http://www.scielo.br/pdf/reeusp/v50nspe/pt_0080-6234-reeusp-50-esp-0074.pdf
9. Ministry of Health (Br). Ministry of Health Surveillance Department of STD, AIDS and Viral Hepatitis. Epidemiological Bulletin HIV/AIDS. Brasília (DF): Ministry of Health; 2016.
10. Villela WV, Barbosa, RM. Trajectories of women living with HIV/AIDS in Brazil. Progress and permanence of the response to the epidemic. Ciênc saúde coletiva [SciELO-Scientific Electronic Library Online] 2017 [cited on Sep. 18, 2017]. 22 (1): 87-96. Available from: http://www.scielo.br/pdf/csc/v22n1/1413-8123-csc-22-01-0087.pdf
11. Moraes DCA, Oliveira RC, Costa SFG. Adherence of men living with HIV/AIDS to antiretroviral treatment. Esc Anna Nery [SciELO-Scientific Electronic Library Online] 2014 [cited on Sep. 18, 2017]. 18: 676-681. Available from: http://www.scielo.br/pdf/ean/v18n4/1414-8145-ean-18-04-0676.pdf
12. Nogueira JA, Silva AO, Sá LR, Almeida AS, Monroe AA, Villa TCS. AIDS in adults 50 years of age and over: characteristics, trends and spatial distribution of the risk. Rev Latino-Am Enfermagem [Scielo-Scientific Electronic Library Online] 2014 [cited on Sep. 18, 2017]. 22:355-63. Available from: http://www.scielo.br/pdf/rlae/v22n3/0104-1169-rlae-22-03-00355.pdf
13. Diógenes MAR, Bezerra IP, Sá RC, Valente, MMQP. Sexuality of human immunodeficiency virus patients in face with the disease: integrative review. Rev bras health promotion [Internet] 2014 [cited on Sep. 18, 2017]. 27 (4): 550-559. Available from: http://periodicos.unifor.br/RBPS/article/view/3069/pdf
14. Ministry of Health (Br). Health Surveillance Department of STD, AIDS and Viral Hepatitis. Clinical protocol and therapeutic guidelines for management of HIV infection in adults. Brasília (DF): Ministry of Health; 2015.
15. Assis MR, Silva LR, Lima DS, Rocha CRR, Paiva MS. Knowledge and sexual practices of HIV positive pregnant women attended at a university hospital. Rev Enferm UERJ [Internet] 2016 [cited on Sep. 18, 2017]. 24 (6): 12536. Available from: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/viewFile/12536/20983
16. Heidemann ITSB, Boehs AE, Fernandes GCM, Wosny AM, Marchi JG. . Health promotion and quality of life: conceptions of the Ottawa Charter in scientific production. Cienc Cuid Saude [Internet] 2012 [cited on Sep. 17, 2017]. 11 (3): 613-619. Available from: http://www.periodicos.uem.br/ojs/index.php/CiencCuidSaude/article/view/13554/pdf
17. Gomes TB, Lourival NBS. Nutritional profile of HIV positive patients in the city of Apucarana (PR). Health and Research Journal. 2016; 9 (1): 83-92.
18. Lima RP, Miranda RNA, Guterrez AS. Impact of nutritional status on adherence to diet therapy in people with HIV. Rev for med [Internet] 2015 [cited on Sep. 18, 2017]. 29 (3). Available from: http://files.bvs.br/upload/S/0101-5907/2015/v29n3/a5561.pdf
19. Furini AAC, Lima TAM, Rodrigues JF, Borges MSB, Carmo EGB, Cecchim MC, et al. Analysis of drug and food interactions in AIDS patients using ART associated with rescue therapy. Rev ciênc basic farm apl. 2015; 36 (3): 427-434.
20. Garbin CAS, Gatto RCJ, Garbin AJI. Adherence to antiretroviral therapy in HIV-seropositive patients in Brazil: a literature review. Arch Health Invest [Internet] 2017 [cited on Nov. 30, 2016]. 6(2): 65-70: 3191-3198. Available from: http://www.archhealthinvestigation.com.br/ArcHI/article/viewFile/1787/pdf
21. Paschoal EP, Santo CCE, Gomes AMT, Santos EI, Oliveira DC, Pontes APM. Adherence to antiretroviral therapy and its representations for people living with HIV/AIDS. Esc Anna Nery [Internet] 2014 [cited on Sep. 28, 2017]. 18 (1): 32-40. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1414-81452014000100032&lng=en
22. Ronzani TM, Noto AR, Silveira PS. Reducing stigma among drug users. Guide for professionals and managers. Juiz de Fora (MG): Editora UFJF; 2014.
23. Kadri MR, Schweickardt JC. Civil Society Organizations in the fight against AIDS in Amazonas, Brazil. Ciênc saúde coletiva [SciELO-Scientific Electronic Library Online] 2015 [cited on Sep. 16, 2017]. 20 (5): 1331-1339. Available from: http://www.scielo.br/pdf/csc/v20n5/1413-8123-csc-20-05-01331.pdf
24. Maliska ICA, Padilha MI, Andrade SR. Policies focused on STDS/AIDS and their social and political integration in the SUS context: a study on the municipality of Florianópolis-SC. Text Context-enferm [SciELO-Scientific Electronic Library Online] 2014 [cited on Sep.16, 2017]. 23 (3): 639-47. Available from: http://www.scielo.br/pdf/tce/v23n3/en_0104-0707-tce-23-03-00639