ORIGINAL RESEARCH
Analysis of cardiovascular risk factors among men practicing unsupervised physical activity
Ieda Carla CandidoI; Guilherme Oliveira de ArrudaII; Adriana Gallego MartinsIII; Sonia Silva MarconIV
I
Professor of Physical Education. Master in Health Sciences. State
University of Paraná. Paranavaí Unit. Paranavaí, Paraná, Brazil. E-mail:
iedacarlacandido@hotmail.com
II
Nurse. Master in Nursing. State University of Maringá, Graduate Nursing
Program. Maringá, Paraná, Brazil. E-mail: enfgoa@gmail.com
III
Professor of Physical Education. PhD in Biological Sciences. State
University of Paraná. Paranavaí, Paraná, Brazil. E-mail:
adrianagallegomartins@gmail.com
IV
Nurse. PhD in Philosophy of Nursing. State University of Maringá. Maringá,
Paraná, Brazil. E-mail:
soniasilva.marcon@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2016.9128
ABSTRACT
Objectives: to estimate the prevalence of cardiovascular risk factors and determine the association between these factors and sociodemographic variables. Methods: cross-sectional study of 128 men practicing unsupervised physical activity in northwest Paraná State, in 2012. Data were collected by structured interview and analyzed descriptively and by test of association. The project was approved by a research ethics committee (CAAE: 0326.0.093.000-11). Results: the most prevalent risk factor was overweight/obesity (71.9%). At least one cardiovascular risk factor was found in 97.7%. Having a female companion increased the likelihood of overweight, and the opposite situation was associated with smoking. Lower levels of education were found to associate with alcohol use. Age group, and higher income and education were associated with hypertension. Conclusion: overweight/obesity was most prevalent factor, almost all men displayed at least one risk factor and these factors were found to associate with marital status, education, age and income.
Keywords: Cardiovascular diseases; motor activity; men's health; risk factors.
INTRODUCTION
Cardiovascular diseases (CVD) have high social and economic costs. In Brazil, they are responsible for about 30% of deaths and 50% of these occur in adults, especially among those aged between 30 and 69 years, a period of life that is characterized by intense productive activity in several senses 1. It must be emphasized that cardiovascular diseases have a significant impact on the morbidity/mortality profile, life expectancy at birth and quality of life of the male population2. Moreover, the prevalence of insufficiently active individuals is lower among men, which indicates higher frequency of physical activity among this population, but without evaluation and monitoring3.
Given the above, the goals defined for the present study were to estimate the prevalence of cardiovascular risk factors and to determine the association of these factors with socio-demographic variables among men who practice unsupervised physical activity.
LITERATURE REVIEW
Among the current risk factors, there are the modifiable, which are characterized by certain habits and conditions such as alcoholism, smoking, overweight or obesity, physical inactivity and hypertension, and the non-modifiable such as age (structural and functional changes of the cardiovascular system) and family history of CVD (heredity), which predispose the occurrence of these diseases and their complications4.
In this context, in order to serve as a strategy for health promotion and prevention of CVD, regular physical activity, especially under professional supervision, emerges as a strong ally in reducing risk factors and consequent CVD, avoiding hospitalizations and premature mortality5. Studies emphasize that physical activity attenuates the development of obesity by raising energy expenditure and reflecting on the cardiovascular performance, mainly through increase of the heart rate6.
Thus, the literature indicates that the collection of information on symptoms, comorbidities and cardiovascular risk factors makes it possible to identify individuals that are prone to develop these diseases, and this may help with effective interventions in these cases7. The practice of physical activity by individuals who are prone to risks may potentiate the occurrence of acute cardiovascular events such as arrhythmia and myocardial ischemia. For this reason, the initial health assessment and continuous monitoring of physical exercise is necessary8.
METHODOLOGY
This is an observational cross-sectional study carried out with men who practice unsupervised physical exercise in a recreational club located in the city of Paranavaí, Northwest region of the State of Paraná, which has a population of 81,595 inhabitants and a population density of 67.88 inhabitants/km2.
The target population of the research consisted of 350 men, frequenters of a private recreational club and participants of an amateur soccer league. All were called through a written invitation delivered during the competition and during lectures on health promotion held at the club on previously scheduled dates. Among the target population, 128 men agreed to participate and they met the following inclusion criteria: be practitioners of physical activity not supervised by a health professional and attend to the game scheduled for the league early enough so that the data could be collected before the game.
Data were collected through the Inventory of Health Conditions in a private place in the club in order to respect the privacy of participants, before they initiate any physical activity. Data collection was carried out between the months of June and November 2012. The variables sex, skin color, marital status, education, family income and health insurance plan (dichotomous) were analyzed as independent variables for each risk factor (response variables).
To calculate body mass index (BMI), the weight and height of participants were recorded as follows: for height measurements, we used a tape previously fixed on rigid and rectilinear platform, and individuals were measured in an upright position, barefoot and with the feet together on a uniform basis, upper limbs extended along the body and head oriented in the Frankfurt plane. Body weight was measured using a Sunbeam scale. To obtain weight, the subject was also instructed to stand barefoot and with as little clothing as possible. BMI was calculated dividing the weight value by the squared value of the height. Then this was classified according to cutoff points: eutrophic (between 18.5 and 24.9 kg/m2 for people younger than 60 years old and between 22 and 26.9 kg/m2 for people aged at or older than 60 years), overweight (between 25 and 29.9 kg/m2 for people younger than 60 years old and 27 kg/m2 for people aged at or older than 60 years) and obese (equal to or above 30 kg/m2)9. None of the participants were underweight. Thus, for purposes of analysis, the variable BMI was categorized in a dichotomous way, distributed into normal and overweight/obesity.
Blood pressure (BP) was measured three times, in the right arm supported at heart level with the individual seated and after five minutes of rest, with an interval of one minute between the measurements, considering only the mean of the last two measurements. If the systolic and/or diastolic pressures presented a difference greater than 4 mmHg, further measurements were performed until differences reached a value equal or below 4 mmHg, and the average of the two closest measurements were used. This followed the recommendations of the Brazilian Society of Cardiology, the Brazilian Society of Hypertension, the Brazilian Society of Nephrology, and the VI Brazilian Guidelines on Hypertension. BP was considered high or altered when above 140 mm/Hg for systolic BP and 90 mm/Hg for diastolic BP 10. The patients in this study were also asked about the diagnosis of hypertension and this is, therefore, a self-reported data as well it is the data on family history of CVD, irregular physical activity, alcohol consumption and smoking.
Data were compiled in the Microsoft Excel 2010, with subsequent migration to IBM SPSS version 20, in which descriptive and inferential statistics (association test) were used. Statistical analysis for associations between variables was performed using chi-square test with Yates correction when necessary, and Odds Ratio (OR) as a measure of association, presented with respective confidence intervals (95%). The level of significance was set at p <0.05.
This study was approved by the Standing Ethics Committee on Research Involving Human Subjects of the signatory institution, following the ethical principles contained in the Declaration of Helsinki, under Opinion nº 0326.0.093.000-11. All participants signed the Informed Consent (IC) in two identical copies.
RESULTS AND DISCUSSION
In the Brazilian scientific scenario, it is clear that studies investigating the prevalence of risk factors for CVD have focused their attention especially to large cities in the Southeast Region11. Efforts have been employed to learn the distribution of mortality and risk factors in the population of small towns in the South Region12.
Regarding socioeconomic and demographic characteristics, among the 128 participants of this study, the mean age was 49.5 years, and nine (7%) of them were aged between 26 and 35 years, 27 (21.1%) between 36 and 45 years, 60 (46.9%) between 46 and 55 years and 32 (25.0%) individuals were aged between 56 and 66 years.
The majority, that is, 96 (75%) subjects declared themselves white skinned, 104 (81.3%) had a partner, 69 (53.9%) had completed high school, 73 (57%) had health insurance plan and 76 (59.4%) had a maximum income of four minimum wages.
Regarding the socio-demographic characteristics of the subjects, no similar studies were found for comparison because the research participants of the present study represent a very specific context which is little studied, that is, the men practicing unsupervised physical activity, which is the differential of the study. However, a research on risk factors for CVD conducted with men in Juiz de Fora Municipality showed similarity in relation to some characteristics such as increased frequency of white men, aged around 50 years, with a companion and education level corresponding up to complete high school13.
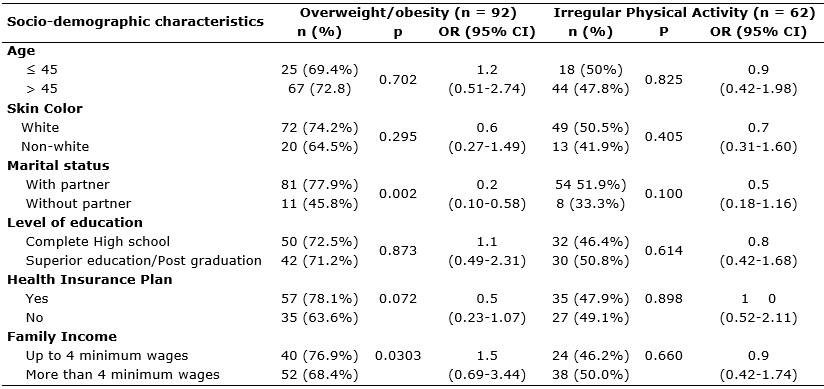
It was observed that 92 (71.9%) men had BMI featuring overweight/obesity, and this risk factor for cardiovascular disease was identified as the most frequent in this study. At the time of the interview, 42 (32.8%) men had abnormal blood pressure. Regarding self-reported factors, it was observed in order of frequency: 78 (60.9%) men reported family history of CVD, 62 (48.4%) reported irregular physical activity, 18 (14%) reported hypertension, 26 (20 3%) reported alcohol abuse and 12 (9.4%) reported smoking.
In this study, overweight/obesity was the most prevalent risk factor, presumably due to two reasons, as already evidenced in the literature: first, because, usually, adults seek physical activity only when they have problems arising from overweight or obesity14; second, because, with advancing age, eating habits, insufficient physical activity, genetic and metabolic factors can considerably hamper the control of body weight15.
It is noteworthy that the prevalence of overweight has increased over the past 35 years, especially among men, from 18.5% in 1974 to 50.1% in 2009. The same happens to obesity, which increased from 2.8% to 12.4%. Such rates are significantly higher among men than among women16. In a study conducted in Switzerland with 18,156 adults, a higher prevalence of overweight was found among men compared to women. However, women were the ones who were more dissatisfied with such a condition, which suggests greater concern of women with health care17.
It was demonstrated that 125 (97.7%) men had at least one risk factor. Fifty (39.06%) men reported two risk factors, 41 (32.03%) reported three factors, 23 (18%) reported one factor and 10 (7.8%) had four risk factors for CVD.
Almost all of the participants have at least one risk factor, which sets a worrying finding, especially because 36 (28.1%) of them are 45 years old or younger. This is, theoretically, a more protected age group with respect to the occurrence of cardiovascular diseases and events18. A study carried out with men aged between 20 and 49 years, and thus young adults, also found high prevalence of at least one risk factor among participants13. Among elderly practitioners of unsupervised physical activity, it was evidenced in São Paulo the prevalence of at least one risk factor in of 70%, thus reinforcing the need for attention mainly geared at adult individuals16.
With regard to findings of the present study, these also showed the relevant fact that most of the men had between two - 51 (39.8%) - and three - 40 (32%) - risk factors. In the city of Pelotas, it was demonstrated that the prevalence of up to two risk factors was higher among women, while the accumulation of three or more factors is common among men19. It is noteworthy that the study carried out in Pelotas considered also the habitual consumption of visible fat and canned food as risk factors.
These findings suggest that many men, practitioners of physical activity, may present some risk factor and when this is associated with lack of proper monitoring of the exercise practice, it can predict problems to male cardiovascular health. Thus, special professional attention, particularly through systemized actions of health promotion and individualized assistance is necessary.
It was possible to identify the status of the men participating in this study regarding overweight/obesity and physical inactivity. There was a significant difference in the distribution of the population as to marital status, and the frequency of men with overweight/obesity who had no partner was significantly lower than men who had partner, with an OR of 0.2. This indicates a chance ratio suggestive of protection against overweight/obesity for men without a partner, that is, men without partner have less chance of developing overweight, as shown in Table 1.
Table 1: Obesity/overweight and irregular physical activity among men according to
socio-demographic characteristics. Paranavaí, Paraná, 2012.
In this line, the knowledge about the characteristics of these men and the contexts in which they live can reinforce taking effective measures aimed at each individual profile. More specifically, with respect to men with overweight/obesity, the fact of having a partner can be decisive for the occurrence of this factor. While there is no consensus in the literature, a study reveals significant differences between marital states with regard to overweight, where the prevalence of this event is lower in unmarried individuals20.
Marital status was presented as significant variable for smoking, that is, the fact of having or not a partner increased the chances for tobacco use in about five times (OR = 5.4). As for level of education, complete high school seemed to be relevant as a factor (OR = 3.6) associated to the occurrence of alcohol consumption among these men, which was almost three times the observed prevalence in men with higher education or postgraduate level, as shown in Table 2.
Table 2: Alcohol consumption and smoking among men practicing unsupervised
physical activity according to socio-demographic characteristics,
Paranavaí, Paraná, 2012. 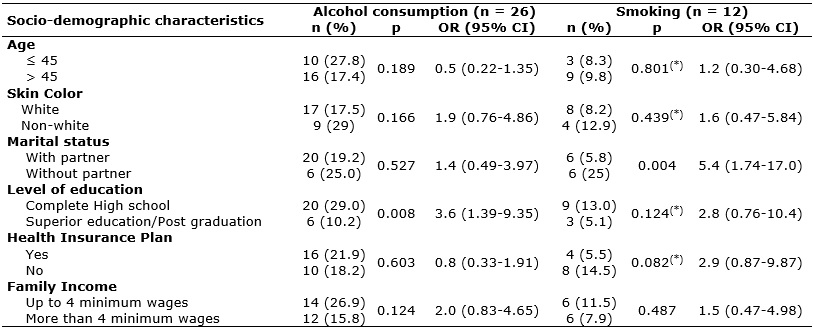
(
*)Chi-square test with Yates correction.
As regards the consumption of alcoholic beverages, the literature is still contradictory in many social segments. It is noted that there is a tendency to the claim that higher alcohol consumption occurs in social strata with lower income and education level21. Among men who are users of alcohol, the association of alcohol consumption with low level of education is reported in the literature. A survey conducted in the metropolitan region of São Paulo found that 42.6% of individuals who did not complete high school had had one episode of drunkenness in the last year, with a significant majority corresponding to men22.
As for tobacco use, while this habit is strongly linked to the male figure, it is worth mentioning the important association pointed in literature between increased income and the decreased prevalence of smoking among men 23. However, the present study showed that marital status has an important association with smoking, and the absence of a partner can be decisive for the development or maintenance of this habit.
In this context, it is necessary to highlight the importance of aspects that go beyond what was shown in this study, whether the subjective well-being or the family environment that pervade the life of the individual24. Thus, this raises the hypothesis that the presence of a partner, especially if this does not make use of cigarettes, can be a positive influence for men, so as not to create this habit or to abandon it in favor of the own health and of the comfort of the people living with him, mainly because women play important role in the care of man 25.
With regard to hypertension, it was found that being older than 45 years increased by eight times the chance of men to have hypertension. It was also observed that men who studied up to High school and who had incomes of up to four minimum wages were less susceptible to hypertension, as shown in Table 3.
Table 3:
Hypertension among men practicing unsupervised physical activity according
to socio-demographic characteristics. Paranavaí, Paraná, 2012 (N = 128).
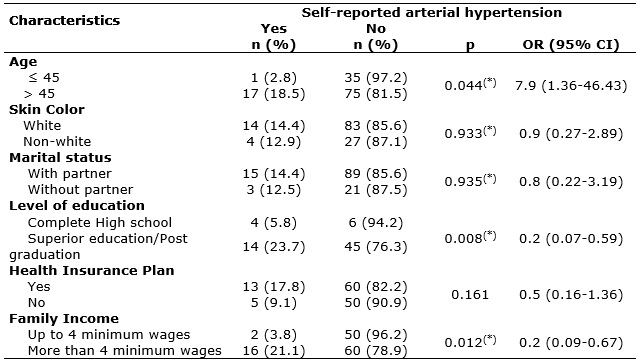
(
*)Chi-square test with Yates correction.
On hypertension, the prevalence found in this study was lower than that identified in other studies: 24% of men from 20 to 49 years old in Juiz de Fora,13 and 42.4% among adults of 100 municipalities 26. However, a study conducted in Goiânia reported a lower prevalence of hypertension among males engaged in physical activity. Even so, it is emphasized that this finding should be interpreted with caution because the possibility of reverse causality in cross-sectional studies cannot be eliminated27.
The increase in the prevalence of hypertension among the male population, especially after 45 years of age, requires proper management of modifiable risk factors for hypertension itself and for other CVD, with immediate adoption of preventive measures, representing an important investment in the field of public health28. A study carried out with men between 18 and 49 years old found that the level of knowledge translated into a significant improvement on Hypertension, reinforcing the importance of prevention and the adoption of healthy behaviors, including the practice of regular physical activity29.
The association between high blood pressure and higher levels of income and education evident in the study, in the sense of protection, finds no support in the literature, as the association with lower levels of these variables is what most commonly occurs28. It is suggested that men with higher income and education seek in physical activity, even without supervision, one option for disease control and consequent improvement in quality of life. This study also found a high prevalence of family history for CVD, which should be considered when assessing the level of risk and the ability for physical activity.
In broader terms, the epidemic of CVD has characteristics that differ between the sexes: increased survival among women, higher male mortality in almost all age groups, greater concern for the health among women and the existence of consolidated specific policies that aim at women's health. In this sense, the Brazilian Society of Cardiology contributed to the implementation of the National Policy of Integral Attention to Men's Health in Brazil, indicating the need to prioritize appropriate approaches geared at risk factors for CVD30.
Thus, based on the results presented and discussed, non-pharmacological measures should be implemented with a view to reducing the prevalence of risk factors for CVD, especially because a significant prevalence of these factors was detected among men who are practitioners of physical activity without proper supervision. A study comparing interventions with and without supervision found that a supervised program of combined training (aerobic and resistance) led to substantial improvement of cardiovascular health parameters, showing the effectiveness of this modality31. It is also noted in the literature that supervised programs are associated with higher levels of physical activity, compared with non-supervised programs32.
The inclination to a pattern of irregular life substantially interferes on the risk of development of CVD, which requires changes and monitoring of the new measures33. In this sense, group activities on health education help to maintain healthy practices and encourage overcoming the potential difficulties that its members may have to face to modify their lifestyle34.
It is necessary to stress the importance of an exercise program, designed and supervised by a competent professional, installed after evaluation of health and physical fitness and based on pre-existing risk factors and predisposition to perform physical activity. Encouraging supervised physical activity to men in different forms of exercise can be decisive for men in combating the risk factors for CVD and their serious consequences. Nurses, especially when acting in the context of primary care, can develop the follow up of men who practice physical activities and may strengthen guidelines on the prevention of risk factors. Therefore, bring the men's health directly to nursing education, addressing issues of gender and expanding the discussion on promotion and prevention of the health of this population can significantly contribute to the preparation of this professional to monitor men who practice physical activities35.
The results of this study indicate that it is fundamental that managers and health professionals be concerned about the need to reduce risk factors for CVD among adult men. Supervised programs of physical activity stand out as an option to be implemented with men, among other strategies for promotion and prevention developed by the public health system in the city.
CONCLUSION
It is considered that the objectives of this study were achieved. The vast majority of individuals present at least one risk factor for CVD, especially modifiable factors. Regarding the change of habits, the regular and supervised physical activity may translate into considerable benefits for these men. They may reduce the prevalence of overweight/obesity and minimize the risk for acute cardiovascular events.
The findings of the present study reinforce the need for educational practices and longitudinal attention to the male population, with a focus on reducing cardiovascular risk. Therefore, as the study suggests, it is necessary to pay attention to the socio-demographic characteristics that are associated with each risk factor, such as age, marital status and education, in order to direct the actions. These findings may subsidize studies aimed at the evaluation of interventions with different populations.
This study had methodological limitations such as small sample size, non-probabilistic selection of participants, risk of reverse causality inherent in cross-sectional studies and the fact that this is a single-center study restricted just a group of practitioners of unsupervised physical activity.
REFERENCES
1.Ministério da Saúde (Br). Secretaria de Vigilância em Saúde. Indicadores de mortalidade. Brasil: Ministério da Saúde; 2006. [cited 2016 Feb 12]. Available from: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?Idb2006/c04
2.Abreu DMX, César CC, França EB. Diferenciais entre homens e mulheres na mortalidade evitável no Brasil (1983-2005). Cad Saúde Pública [Scielo-Scientific Electronic Library Online] 2009 [cited 2016 Mar 05] 25(12):2672-82. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0102-311X2009001200014
3.Costa LC; Thuler LC. Fatores associados ao risco para doenças não transmissíveis em adultos brasileiros: estudo transversal de base populacional. Rev Bras Estud Pop. 2012;29(1):133-45.
4.Malta DC, Cezário AC, Moura L, Neto OLM, Silva Júnior JB. Construção da vigilância e prevenção das doenças crônicas não transmissíveis no contexto do sistema único de saúde. Epid Serv Saúde. 2006; 15(1):47-64.
5.Patterson CM, Dunn-meynell AA, Levin BE. Three weeks of early-onset exercise prolongs obesity resistance in DIO rats after exercise cessation. Am J Physiol Regul Integr Comp Physiol. 2008; 294(2):290-301.
6.Mazini Filho ML, Rodrigues BM, Aidar FJ, Reis VM, Polito MD, Venturini GP, et al. Influência dos exercícios aeróbio e resistido sobre perfil hemodinâmico e lipídico em idosas hipertensas. Rev Bras Cienc Mov. 2011;19(4):15-22.
7.Schmidt MI, Duncan BB, Silva GA, Menezes AM, Monteiro CA, Barreto SM, et al. Health in Brazil 4. Chronic non-communicable diseases in Brazil: burden and current challenges. The Lancet, 2011; 377.
8.Luz LGO, Maranhão Neto GA, Farinatti PTV. Validade do questionário de prontidão para a atividade física (par-q) em idosos. Rev Bras Cineantropom Desemp Hum. 2007; 9(4):366-71.
9.National Institutes of Health. The practical guide identification, evaluation, and treatment of overweight and obesity in adults. Bethesda, MD: National Institutes of Health, National Heart, Lung, and Blood Institute and North American Association for the study of Obesity; 2000.
10.Sociedade Brasileira De Cardiologia/Sociedade Brasileira De Hipertensão/Sociedade Brasileira De Nefrologia. V Diretrizes Brasileiras De Hipertensão. Arq Bras Cardiol 2006; 95:1-50.
11.Bloch KV, Rodrigues CS, Fiszman R. Epidemiologia dos fatores de risco para hipertensão arterial: uma revisão crítica da literatura brasileira. Rev Bras Hipert. 2006; 13(2): 134-43.
12.Medeiros CRG, Meneghel SN, Gerhardt TE. Desigualdades na mortalidade por doenças cardiovasculares em pequenos municípios. Ciênc saúde coletiva. 2012; 17(11):2953-62.
13.Eyken EBBD`OV, Moraes CL. Prevalência de fatores de risco para doenças cardiovasculares entre homens de uma população urbana do Sudoeste do Brasil. Cad Saúde Pública. 2009; 25(1):111-23.
14.Fermino RC, Pezzini MR, Reis RS. Motivos para prática de atividade física e imagem corporal em frequentadores de academia. Rev Bras Med Esporte. 2010; 16(1):18-23.
15.Iser BPM, Claro RM, Moura EC, Malta DC, Neto OLM. Fatores de risco e proteção para doenças crônicas não transmissíveis obtidos por inquérito telefônico – VIGITEL. Brasil - 2009. Rev Bras Epidemiol. 2011;14(1):90-102.
16.Mendonça TT, Ito RE, Bartholomeu T, Tinucci T, Forjaz CLM. Risco cardiovascular, aptidão física e prática de atividade física de idosos de um parque de São Paulo. Rev Bras Ciênc Mov. 2004;12(2):19-24.
17.Forrester-Knauss C, Stutz EZ. Gender differences in disordered eating and weight dissatisfaction in Swiss adults: Which factors matter? BMC Public Health. 2012; 12:809.
18.Sociedade Brasileira de Hipertensão. Consenso Brasileiro de Hipertensão Arterial. Campos de Jordão (SP); 2011.
19.Muniz LC, Schneider BC, Silva ICM, Matijasevich A, Santos IS. Fatores de risco comportamentais acumulados para doenças cardiovasculares no sul do Brasil. Rev Saude Publica. 2012;46(3):534-42.
20.Eloi D, Aurélie F, Yolande E. Cardiovascular diseases and psychosocial factors at work. Archiv Cardiovasc Disease. 2012; 105(1):33-9.
21.Iser BPM, Yokota RTC, Sá NNB, Moura L, Malta DC. Prevalência de fatores de risco e proteção para doenças crônicas nas capitais do Brasil – principais resultados do Vigitel 2010. Ciênc saúde coletiva. 2012; 17(9):2343-56.
22.Cavariani MB, Oliveira JB, Kerr-Correa F, Lima MCP. Expectativas positivas com o uso de álcool e o beber se embriagando: diferenças de gênero em estudo do Projeto GENACIS, São Paulo, Brasil. Cad Saúde Pública, 2012; 28(7):1394-404.
23.Dias-Damé JL, Cesar JA, Silva SM. Tendência temporal de tabagismo em população urbana: um estudo de base populacional no Sul do Brasil. Cad Saúde Pública. 2011;27(11):2166-74.
24.Abreu MNS, Souza CF, Caiaffa WT. Tabagismo entre adolescentes e adultos jovens de Belo Horizonte, Minas Gerais, Brasil: influência do entorno familiar e grupo social. Cad Saúde Pública. 2011;27(5):935-43.
25.Gutierrez DMD, Minayo MCS, Oliveira KNLC. Homens e cuidados de saúde em famílias empobrecidas na Amazônia. Saúde Soc. 2012; 21(4):871-73.
26.Piccini RX, Facchini LA, Tomasi E, Siqueira FV, Silveira DS, Thumé E, et al. Promotion, prevention and arterial hypertension care in Brazil. Rev Saude Publica. 2012; 46(3):543-50.
27.Cunha IC, Peixoto MRG, Jardim PCBV, Alexandre VP. Factors associated with physical activity in Goiania's adult population: surveillance through telephone interviews. Rev Bras Epidemiol. 2008; 11(3):495-504.
28.Cipullo JP; Martin JFV; Ciorlia LAS; Godoy MRP; Cação JC, Loureiro AAC, et al. Prevalência e fatores de risco para hipertensão em uma população urbana brasileira. Arq Bras Cardiol. 2010; 94(4): 519-26.
29.Leite DF, Ferreira IMG, Souza MS, Nunes VS, Castro PR. A influência de um programa de educação na saúde do homem. Mundo Saúde. 2010; 34(1):50-6.
30.Chagas ACP, Zilli EC, Ferreira JFM, Moretti MA, Ramos RF. Saúde cardiovascular do homem brasileiro – visão da sociedade brasileira de cardiologia. Arq Bras Cardiol. 2009; 93(6):584-587
31.Stefanov T, Vekova A, Bonova I, Tzvetkov S, Kurktschiev D, Bluher M, et al. Effects of supervised vs non-supervised combined aerobic and resistance exercise pragramme on cardiometabolic risk factors. Cent Eur J Public Health. 2013; 21(1):8-16.
32.Gobbi S, Menezes E, Tanaka K. Programas supervisionados de atividades físicas estão associados a maior nível de atividade física comparados com não supervisionados. Rev Bras Ativ Fis Saúde. 2007;12(1):3-7.
33.Han Y, Han M, Lee S, Sarkar AMJ, Lee YK. A framework for supervising lifestyle diseases using long-term activity monitoring. Sensors. 2012; 12(5):5363-79.
34.Soares LC, Santana MG, Thofehm MB, Dias DG. Educação em saúde na modalidade grupal: relato de experiência. Ciênc Cuid Saúde. 2009; 8(1):118-23.
35.Ribeiro DB, Terra MG, Lacchinni AJB, Camponogara S, Beuter M, Silva CT. Saúde dos homens: abordagem na formação dos enfermeiros. Rev enferm UERJ. 2014; 22(4):540-5.