RESEARCH ARTICLES
The empathic skill is socially learned: an experimental study with nursing undergraduate students
Celia Caldeira Fonseca KestenbergI
INurse, Psychologist, PhD in Social Psychology. Assistant Professor in the Nursing Graduate Program at the State University of Rio de Janeiro, Coordinator of the Extension Program knowledge and Creative Practices in Health. Interpersonal Relations Group Member of the National Association of Research and Graduate Studies in Psychology. Email: celiaprofuerj@gmail.com
ABSTRACT: This study’s objective was to assess an empathy promotionprogram of for nursing undergraduate students, which was developed and tested according to the experimental model.17 students took part in 16 meetings of group training, with a three-hour duration each, whereas 16 students formed the control group. The conception of empathy adopted followed a multidimensional perspective that involves cognitive, affective and behavioral dimensions. Participants fromboth groups were assessed before the intervention, immediately after and within a 30-40 days follow-up. Cognitive and affective empathy components were assessed using an Empathy Inventory. Role-playing was used to assess the verbal empathic behavior. Results: all the values of the significance tests, p< 0.05, were significant, with higher average values on the experimental group. It is concluded that the program was effective by substantially increasing cognitive and affective empathy aspects, as well as the empathic verbalizing.
Keywords: Empathy; social skills; nursing care, behavioral assessment
INTRODUCTION
Empathy is a socially learnedskill, essential for the construction and maintenance of affective bonds.Although there appears to be a consensus on the importance of empathy in nurse-patient relationship, some gaps are identified in nursing studies with regard to the training of professionals to develop the behavior empathize and include: How one learns to active listening and welcoming? How one learns to increase awareness facing the patient's pain and demonstrate validation of their internal state? Where there is a conflict of interestsas one learns to empathetically,deal in interaction situations with the patient? Reviewed nursing studies1-7 show the concern of researchers in outlining empathetic skills as essential for nursing care. In these studies, a predominance of the concept of empathy in perspective emotional/affective was shown, but different researchers from psychology8-11 have considered empathy a complex phenomenon and to define how a multidimensional social skill that involves cognitive, affective and behavioral, components. They add that there is a degree of relevance between the three, since their integration, which defines the empathic behavior.
Childhood12-14 is the decisive moment in the development of social skills empathetic qualities, although throughout life new opportunities for their development may occur, including the formal/systematized learning11,13,15-17 which has shown to be quite adequate for bringing benefits to both the individual and collective. The importance is emphasized on the training programs to expand the number of people to benefit, since the more socially skilled usually have more ease of dealing with a diversity of relationships in all social spheres. From this context, thinking of the empathy as an ability socially learned and fundamental for nursing, the objective of this study was to evaluate the effectiveness of an empathy promotion program for nursing graduates.
THEORETICAL-METHODOLOGICAL FRAMEWORK
The empathy topic has aroused the interest of researchers from different areas, making it a multidisciplinary study field, covering the areas; evolutionary, social, personality and clinical18.More recently, it has also been explained in the area of neurosciences9,19,20.It is possible to understand the ability to empathize from the understanding of the existence of neural mechanisms, which enable man to feel emotions. Ii is the activation of a nervous circuit type as if, that is, a circuit simulation of body changes induced by an experience of emotions through the activation of sensory maps. In accordance with biology and evolutionary psychology, the ability to experience empathy developed as a resource for survival and perpetuation of genes. Therefore, humans and several species are born biologically predisposed to experience contagion to witness the discomfort of others. On the other hand, such predisposition cannot develop without learning, from the social interactions and emotional bonds20. In the field of psychotherapy, the Rogerian design is pointed out as the most relevant on the topic and his contribution was also great for education7-10,18.
In this study, empathy is understood as a social interaction ability and is a multidimensional phenomenon that encompasses cognitive, affective and behavioral components8,11,21.The cognitive is designed by the adoption of the other's perspective, which is, the ability to interpret and understand the feelings and thoughts of someone. The recognition of emotions is one of the cognitive requirements for empathy. The interpersonal flexibility constitutes another important aspect in cognitive process that is reflected by high capacity to accept perspectives, beliefs and values very different, in addition to tolerance to frustration caused by the attitude of the speaker. The empathy affective component expresses a tendency to experience signs of sympathy and compassion for others, as well as genuine concern with the well-being of another. The empathy behavioral component is characterized by verbal and non-verbal communicating, an explicit recognition of the feelings and the perspective of the other person, so that they will feel truly understood.
Empathy, in this multidimensional perspective, it involves two distinct stages: the first named from empathic understanding consists in an attempt to understand the feelings and perspectives of another, through behaviors that demonstrate attention and listening empathetic qualities; the second step, empathetic expression, understands the empathic verbalization focusing on feelings and the prospect of another15.22.
Method
The program was conducted throughout a study with two typified groups under an experimental design (experimental and control groups), which was attended by 33 students from the 8th period of the Undergraduate Nursing Course at a public university in Rio de Janeiro. The 17 students in the experimental group and 16 in the control group were evaluated before the intervention, immediately after and with a follow-up of 30-40 days. The Empathy Promotion Program was performed in 16 weekly meetings with an average duration of three hours each.
The empathy cognitive andaffective components of were evaluated by means of an Empathy Inventory23 that corresponds to a self-report measurement type constructed and validated in the Brazilian context, which intends to measure the empathic ability of adult individuals. The answers to those questions correspond to the Likert scale type, with five options, ranging from never to always having 23 direct and 17 reverse.
The 40 scale items were grouped into four factors: perspective taking (PT): ability to understand the perspective and feelings of another person, especially in situations in which there is a conflict of interest. Interpersonal Flexibility (IF), a high capacity to accept perspectives, beliefs and values very different, and frustration tolerance caused by the attitude of the speaker. Altruism (AL), ability to sacrifice temporarily their own needs, for the benefit of another person, for the sake of their well-being. Affective sensitivity (AS) is the tendency to experience feelings of compassion and concern for the emotional state of another. The first two correspond to cognitive dimension and the last two the affective dimension of empathy.
The ability to verbalize emphatically was assessed using the Empathic Verbal Behavior Assessment Instrument(EVBAI)23, created for this study. Aims to assess the verbal empathic behavior from role-playing. There are six situations for empathic responses, three help without conflict of interest (the numbers of 3, 5 and 6) and three help with conflict of interest (1, 2 and 4). The answers are categorized from 1 to 5 on a Likert Scale - since the answer totally inadequate to fully empathetic. The individual score totals may vary from 6 to 30. The individual scores for each situation may vary from 1 to 5, being the cut-off point for the assessment of verbal behavior empathy, score 4.
The procedures used aimed to enhance participants' ability to identify emotional signals in nonverbal behavior of others; hear and understand the perspective and feelings of others, without judging, demonstrate empathic behavior by nonverbal communication; verbalize empathically understanding the feelings and the perspective of the other.
Of the 16 meetings, eight were required to train the first step of empathy, understanding empathy. The experiences they had as a focus to develop the ability to; identify emotions and non-verbal signals in communication between people; hear and understand roughly, what is being communicated; listen and understand emphatically in situations where someone expresses need for aid without a conflict of interests and in situations where there is a conflict of interests. For the second stage of empathic empathy, expression was intended for six meetings in which the experiences focused on the ability to perform empathic behavior. Such as in, situations of verbal help without a conflict of interest situation in role-play, verbalplay empathic behavior with a patient who expresses the need for help without conflict of interest situation in role-playing perform verbal empathic behavior with a patient who expresses the need for help with conflict of interest in a role-playing situation.
The first meeting’s objective was: to facilitate the integration between the members of the group through an experience involving childcare, choice, positive affection; provide an overview on the multidimensional conceptualization of empathy and its importance for nursing. As well as define the contract of coexistence of the group where it was stressed the importance of the frequency, punctuality, participation by specifying what is expected of each member for the proper functioning of the group and explaining the ethical issues.
The other meetings followed the same format, i.e. each meeting was structured into six steps, as specified below:
At the end of each meeting, the participant received a text on the topic discussed. The last meeting was devoted to closing the group and evaluation of the Empathy Promotion Program and camaraderie of the group with the participation of the coordination and collaborators.
RESULTS
For comparison between groups were used, the parametric Student's t tests; for comparison between the subjects (intra-group analysis experimental and control) ANOVA; Bonferroni test for comparison of arithmetic averages after application of ANOVA; Kappa Test to assess the degree of concordance of scores of Behavioral Assessment Verbal Empathy, between judges. The minimum significance level adopted was 5%.
For the formation of the base line, it was found the equivalence between the two groups with regard to the degree of empathy and to empathize verbal behavior, i.e. all values of p>0.05. As For the Inventory of Empathy, we obtained the following result: perspective-taking p= 0.11; interpersonal flexibility p= 0.38; altruism, p= 0.44; affective sensibility, p= 0.58. The comparison between the two groups with the second measure used (EVBAI), through the total scores in six situations of role performance (S1, S2, S3, S4, S5 and S6), shows no statistical significance, p-value=0.85.
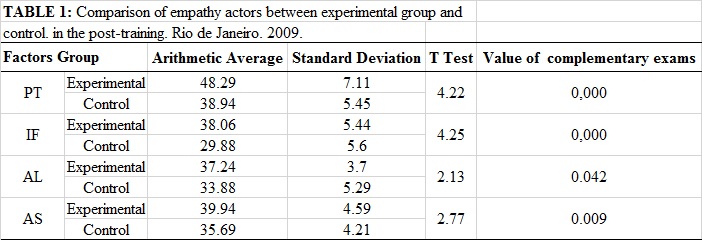
A hypothesis test was conducted on the programinfluence on the variable degree of empathy, the four factors that make up the inventory Empathy, shortly after completion of training. Allt-test values were significant, observing higher average valuesin the experimental group. This demonstrates, therefore, rejecting the null hypothesis and proving the hypothesis of this research, i.e., the EPP had an effect on the participants in all states as factors in Table 1.
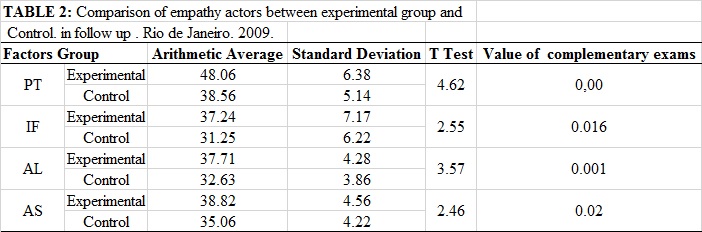
The hypothesis test of the influence of the program on the variable degree of empathy, the four factors that make up the inventory at 40 days follow-up, found that the difference between the experimental group and the control achieved statistical significance. All t values were significant with the average values higher in the Experimental Group (p<0.05). Therefore, up to the moment of assessment at follow-up, the differences remained, proving that there was no decrease in learning empathy offered by the program, according to Table 2.
We tested the influence of PPE on theverbal behaviorempathy of students as shown in Figure 1. It was observed that the difference between the experimental group and the control group regarding the empathetic verbal behavior change in all three phases of the research. While the experimental group experienced the influence of the PPE course, the control group showed only a slight improvement was not significant throughout the stages, more specifically in the follow-up probably due to the factor testing, as well as maturation and history in this type of experimental design26.
AquiFigura 1
DISCUSSION
In nursing studies that address care, it was observed that the empathy topic is always present. However, it has been constituted as a challenge from the point of view of practice, i.e., the materialization of empathic behavior the daily lives of health institutions. Most likely because it is generally considered, as a personal attribute. Therefore, the limited repertoire of skills cannot be seen and when shown, are not in the habit of systematically train professionals in the skills of human interaction.
The results of this study show the magnification of affective components, behavioral and cognitive empathy n the nursing graduates, which reinforces previous studies11,13,15,16,17,27-29, when confirm the increase of such skills, through training programs.The ability to pay attention and listen substantially the other, without judging, leaving aside for a moment the own beliefs, is the first step to true understanding. The skills to take the perspective of someone (cognitive) allow overcoming the egocentrism, guiding our behavior toward the expectations of the other, making it easier to help and care21. The perspective taking makes man more capable of looking at the world through the eyes of another, and experience similar feelings towards the other person. Contributions of neurosciences asserting that the perspective taking produces activation in specific parts of the prefrontal cortex involved in executive functions, mainly related to inhibitory control. In addition, the frontal lobes may serve to separate both perspectives, helping the individual to resist interference from own perspective to take the perspective of another20.
The ability to represent and report their own mental states (self-awareness) is what will allow the inferential knowledge of the mental state of others (consciousness of another)20. The awareness of their own feelings and the ability to consciously regulate the emotions is what will allow the individual disconnecting the answers empathetic qualities addressed to other than their own personal distress. Thus, empathy requires a minimum of distinction between the “I” and the other, being such a distinction demonstrated experimentally in recent studies, in both neuronal and behavioral levels21.23. If the nurse is not able to regulate their own emotions in contact with the patient, it becomes difficult activate a helping behavior, because experiencing the anguish the professional focuses on the experience in itself which makes it difficult to pay attention, listen and understand the reasons for the patient and this can cause consequences for nursing care.
Therefore, it is of fundamental importance to differentiate the affective component of empathy, characterized by feelings of concern, compassion, sympathy and interest by anguish of someone. Hence leading to behaviors of aid directed to another person, personal distress, which is identified by an emotional reaction aversive and so self-centered, triggered by the perception of distress to another person,which leads the individual to distance themselves physically or emotionally10,11,15. Some nursing professionals faced with the pain of the patient are identified with the same, what can they cause emotional suffering, while others are drifting away from the situation as a mechanism of perpetuation, but in both cases there is a likelihood of compromising the effectiveness of nursing care23,30-32. It is possible to think that one of the great challenges of nursing is to have the ability to have mercy, if awareness before the pain of the patient counting with cognitive resources that would allow the management affective and a practice of professional care, effectively.
In the role performance evaluation in situations to help with and without conflict of interest, it was evidenced that the students were able to verbalize empathically in six situations, pointing to an issue very significant in training: the empathic accuracy. Only through the empathic expression is that if you can say about the ability of someone having understood the thoughts and feelings of another15. Important to emphasize that the students have expanded their ability to verbalize empathically faced with situations of patients that involved feelings of hostility, anger, sadness, where there was conflict of interest. By the degree of difficulty of these situations, the students needed a larger effort to regulate the emotions that naturally are evoked in situations of this nature, as was seen in the responses given before the intervention23.32.
In fact, it is not easy to put yourself in the patient, because it runs the risk of being caught by their emotions and there are many such encounters in daily professional practice. It requiresmore accurate understanding of the empathic process to be able securely put yourself in another's place. Nurses must be able to discriminate what is theirs and what is the patient's, be sensitive and flexible enough to let your prospects aside temporarily to adopt and validate the patient's point of view. Validate and accept the other, is not the same as agreeing with the other and this understanding, sometimes, it is not clear, which interferes with the sympathetic attitude and the actions of the care23.
If a patient refuses to receive care, but requires the same, then the professional will be faced with an assistance situation involving conflict of interests. This will require an effort on the part of the professional to understand the reasons for the patient, without judge as right or wrong and verbalize this understanding in such a way that he feels understood, hence their anxiety level reduces and then, the professional will be opening paths channel, listening to the negotiation with the patient.
When the patient can express their deepest feelings and the nurse the returns so clarified, the result is a sense of being understood and ensured a sense of sharing the humanity with someone who has the ability to understand23.
The empathy seems to be a technology to help the nurse caring for the patient, but also to take care of themselves because the reduction of negative affection favors the closeness, the strengthening of ties, the construction of the therapeutic relationship, and the sense of fulfilled duty.Empathy is a two-way street, the patient to feel understood in his suffering, accepted and care, you can try to demonstrate a sense of comfort and well-being, which favors awakening from nurses this same experience because they both come in a thin line.
CONCLUSION
The results obtained in the evaluation of the Empathy Promotion Program are consistent with studies that underpin this research. It has been proved the hypothesis - the EPP had a positive effect on the dimensions cognitive, affective and behavioral of participants.
Empathy as an ability of social interaction can be learned formally if there is a careful systematization regarding the format of the training and assessment instruments is also important to have clarity on the conceptual ability and constituents that one wants to train. Whereas empathy is the social skills that help in the construction and maintenance of bonds and reducing conflicts, it is certainly desirable and necessary for nursing professionals, because it is one of the professions that most deals with human suffering - even though there is no cure, there is always the presence of care. The implementation of a program is suggested thatfor the promotion of empathy in training courses for nursing professionals and in training services and assessment of health institutions. Care is a human act and imposes itself as a value, and then the behavior empathy is a moral and ethical duty of nursing professionals.
REFERENCES
1. Macêdo SM, Sena MCS, Miranda KCL.Consulta de enfermagem ao paciente com HIV: perspectivas e desafios sob a ótica de enfermeiros. RevBrasEnferm. 2013; 66: 196-201.
2. Beck CLC, Lisbôa RL, Tavares JP, Silva RM, Prestes FC. Humanização da assistência de enfermagem: percepção de enfermeiros nos serviços de saúde de um município. Rev GaúchaEnferm. 2009; 30:54-61.
3. Sulzbacher M, Reck AV, StummEMF, Hildebrandt LM. O enfermeiro em unidade de tratamento intensivo vivenciando e enfrentando situações de morte e morrer. Scientia Medica. 2009; 19:11-6.
4. Oliveira AML, Guirardello EBE. Satisfação dos pacientes com os cuidados de enfermagem: comparação entre dois hospitais. Revescenferm USP. 2006; 40:71-77.
5. Carvalho MVB, Merighi MAB. O cuidar no processo de morrer na percepção de mulheres com câncer: uma atitude fenomenológica. Rev Latino-Am Enfermagem. 2005; 13:951-59.
6. Benincá CR, Fernandez M, Grumann C. Cuidado e morte do idoso no hospital: vivência da equipe de enfermagem. RevBras de Ciências do Envelhecimento Humano. 2005; 2:17-29.
7. Takaki MH, Sant’Ana DMG. A empatia como essência no cuidado prestado ao cliente pela equipe de enfermagem na unidade de terapia intensiva. CogitareEnferm. 2004; 9:78-83.
8. Wall FBM. A era da empatia: lições da natureza para uma sociedade mais gentil. São Paulo: Companhia das Letras; 2010.
9. Preston SD, Wall FBM. Empathy: its ultimateandproximate bases. Behavior and Brain Sciences. 2002; 25:1-72.
10. Davis MH. Measuring individual differences in empathy: evidence for a multidimensional approach. Journal of Personality and Social Psychology.1983; 44:113-26.
11. DelPrette A, Del Prette ZAP. Psicologia das relações interpessoais: vivências para o trabalho em grupo. São Paulo: Vozes; 2009.
12. Caballo VE. Manual de avaliação e treinamento das habilidades sociais. São Paulo: Santos; 2006.
13. Batson CD, Fultz J, Schoenrade PA. Las reacciones emocionales de los adultos ante el mal estarajeno. In: Eisenberg N, Strayer J, organizadores. La empatía y sudesarrollo. Bilbao (Es): Desclée de Brower; 1992. p.181-204.
14. Falcone EMO. A avaliação de um programa de treinamento da empatia com universitários [tese de doutorado]. São Paulo: Universidade de São Paulo; 1998.
15. Ickes W, Marangoni C, Garcia S. Studyingempathicaccuracy in a clinicallyrelevantcontext. In: Ickes W, organizer.Empathic accuracy. New York: The Guilford Press; 2009. p.282-310.
16. Yu J, Kirk M. Measurement of empathy in nursing research: systematic review. Journal of Advanced Nursing. 2008; 64:440-54.
17. Kruijver JPM, Kerkstra A,Francke AL, Bensing JM, Van de Wiel HBM. Evaluation of communication training programs in nursing care: a review of the literature. Patient Education and Counseling. 2000; 39:129-45.
18. Eisenberg N, Murphy BC, Shepard S. The development of empathic accuracy. In: Ickes W, editor. Empathic accuracy. New York: The Guilford Press; 2009. p.73-116.
19. Decety J, Jackson PL. The functional architecture of human empathy. BehavCognNeurosci Rev. 2004; 3:71-100.
20. Decety J, Lamm C. Empathy versus personal distress: Recent evidence from social neuroscience. In: Decety J, Ickes W organizers. The social neuroscience of empathy. Massachusetts (USA): A Bradford Book; 2009. p.199-213.
21. Falcone EMO. Empatia: a sabedoria do vínculo afetivo e das relações sociais. In: Anais do 2º Seminário Internacional de Habilidades Sociais; 2009 jun 3-5; Rio de Janeiro, Brasil. Rio de Janeiro: Universidade do Estado do Rio de Janeiro; 2009. p.5-14.
22. Falcone EMO, Ferreira MC, Luz RCM, Fernandes CS, Faria CA, D’Augustin JF, et al. Inventário de empatia (I.E.): desenvolvimento e validação de uma medida brasileira. Rev Aval Psicológica. 2008; 7:321-34.
23. Kestenberg CCF. Avaliação de um programa de desenvolvimento da empatia para graduandos de enfermagem [tese de doutorado]. Rio de Janeiro: Universidade do Estado do Rio de Janeiro; 2010.
24. Jacobson E.Relax: como vencer as tensões. Tradução de Heloysa de Lima Dantas. São Paulo: Cultrix; 1981.
25. Schultz J H. Auto-relaxaçãoconcentrativa, exposição clínico-prática. São Paulo: Mestre Jou; 1967.
26. Campbell, DT, Stanley JC. Delineamentos experimentais e quase-experimentais de pesquisa. São Paulo: EPU; 1979.
27. Reynolds W, Scott PA, Austin W. Nursing, empathy and perception of the moral. JournalofAdvancedNursing. 2000; 32: 235-42.
28. Garcia-Vera MP, Sanz J, Gil F. Entrenamientos em habilidades sociales. In: Gil F, Rubio JML organizadores.Habilidades sociales: teoria, investigacion e intervencion. Madrid (Es): Editorial Sintesis; 1998.
29. Nichols MP. The lost art of listening. New York: Guilford Press; 2009.
30. Santos EI, Gomes AMT, Oliveira DC, Santos CCE. Entre sofrimento e prazer: vulnerabilidade para enfermeiros nas relações interpessoais com pacientes com HIV/AIDS.
Revenferm UERJ. 2013; 21:9-15.
31. Pimentel MRAR, David HMSL. Formação crítica de enfermeiros: repercussões na Universidade do Estado do Rio de janeiro. Revenferm UERJ. 2013; 21: 247-53.
32. Kestenberg CCF, Falcone EMO. Empatia em enfermeiros: a importância da tomada de perspectiva na redução da angústia pessoal. In: Falcone EMO, Oliva AD, Figueiredo C, organizadores. Produções em terapia cognitivo-comportamental. São Paulo: Casa do Psicólogo; 2012.