
RESEARCH ARTICLES
Nurses' organizational Tracking of alcohol use among drivers after implementation of Brazil's Drink-driving Law
Louise Anne Reis da PaixãoI; Angela Maria Mendes AbreuII; José Mauro Braz de LimaIII
I
M.Sc. in Nursing. Nurse, Family Health Strategy, City of Rio de Janeiro. E-mail: lousieppaixao@gmail.com
II
Ph.D. in Nursing. Adjunct Professor, Anna Nery School of Nursing, Universidade Federal do Rio de Janeiro. Public Health Nursing Department. E-mail: angelabreu@globo.com
III
Ph.D. in Medicine. Associate Professor, School of Medicine, Universidade Federal do Rio de Janeiro. E-mail: jmbl@globo.com
DOI: http://dx.doi.org/10.12957/reuerj.2015.8499
ABSTRACT
This cross-sectional study to identify patterns of drinking among motor vehicle drivers and to associate this with drink-driving behavior at a Traffic Department (DETRAN) station in Rio de Janeiro City. Data were collected in 2011 by applying the Alcohol use disorders identification test (AUDIT) questionnaire, with additional drink-driving-related variables, to the 390 study participants, and tabulated using Epi-Info 2000 software. Analysis revealed a significant frequency of drivers classified by AUDIT as problematical drinkers, who reported drinking and driving, even after enactment of Law 11.705/08. This underlines the need to extend education and inspection with regard to drink-driving.
Keywords: Accidents, traffic; accident prevention; alcohol-related disorders; public health nursing.
INTRODUCTION
Traffic accidents are a severe public health problem. Around the world, more than 1.2 million people are killed each year due to this problem, representing more than 2.1% of the global mortality1,2.
Today, traffic accidents are the main cause of deaths among children and young people3, representing more than 40% of deaths among people between 0 and 25 years of age2.
In view of that reality, it is estimated that, in 2020, traffic accidents might be the third main cause of death around the world and the number of deaths may reach about 2.4 million people4,5.
To minimize this morbidity and mortality in traffic, the United Nations Organization (UNO) established the period from 2011 till 2020 as the Decade of Action for Road Safety, aiming to better direct targets to contain the growth of traffic accidents, mainly in developing countries5.
In Brazil, these statistics are also a source of concern. According to the Report by the Ministry of Health, in 2010, 145,920 hospitalizations of traffic accidents were funded by the Unified Health System (SUS), indicating that, for every 100 thousand Brazilian, 76.5 were hospitalized due to traffic accidents. It is highlighted that the Southeast concentrated almost half of these hospitalizations (44.9%)6.
Different Brazilian7-9 and international1-3,10 studies appoint alcohol use as an important risk factor to provoke car accidents, as this consumption causes impaired judgment, reaction time and reduced visual acuity for the driver10.
Thus, the objectives in this study were: To identify the alcohol consumption patterns among motor vehicle drivers and associate this alcohol consumption pattern with these drivers' drinking and driving behavior after the implementation of the Dry Law in Brazil.
LITERATURE REVIEW
In 2008, the Brazilian government enacted Law 11,705 on 06/19/2008, which determines zero alcohol use to drive any motor vehicle. In addition, another measure the Brazilian government adopted was the National Pact for the Reduction of Traffic Accidents – Pact for Life, which officially triggered the International Decade of Actions for Traffic Safety (2011-2020), strengthening the country's commitment to reduce its car accident statistics6.
This supports the other Public Health Policies in Brazil, such as the National Traffic Policy11, the National Alcohol Policy12 and the National Agenda of Health Research Priorities13, which strengthen the need to promote effective actions to reduce the morbidity and mortality in traffic deriving from alcohol use/abuse.
METHOD
This is a cross-sectional and descriptive study, deriving from a Master's thesis defended at Anna Nery School of Nursing - Universidade Federal do Rio de Janeiro. The study was undertaken in 2011 at one of the offices of the Department of Traffic (DETRAN) in the city of Rio de Janeiro (RJ), in the sector called Service Center for Citizen's Driving Permit. The study population consisted of 434 individuals randomly selected to participate in the research. Nevertheless, 10.14% of the participants were lost, as 4% complied with the exclusion criteria and the remaining 6.1% did not fill out the questionnaire correctly, totaling a sample of 390 people.
In this research, male and female individuals were included who held a Brazilian driver's license in any type of category, whether for two or four-wheel motor vehicle, who attended DETRAN-RJ to renew or get a copy of their driver's license (CNH) and/or obtained an international CNH and/or added a category to their CNH at the time of the data collection. Subjects who were obtaining the permission to drive were excluded, as they were not motor vehicle drivers yet, as well as subjects who were regaining their driver's license, as their CNH had been apprehended or suspended due to a traffic violation.
To collect the data, the Alcohol use disorders identification test (AUDIT) was used, in combination with variables related to drinking and driving. The AUDIT is a tool to screen for alcohol use, developed by the World Health Organization, recognized and validated in different regions around the world, including Brazil. This instrument is a simple method to investigate alcohol use and can be applied in different services and in different cultural contexts, mainly in primary health care14.
The AUDIT contains ten questions on alcohol consumption in the past 12 months and its answers are scored between zero and four points. The interviewee's score can be divided according to the following alcohol consumption patterns, low-risk drinker (zone I-score between zero and seven points), hazardous drinker (zone II-score from eight to 15 points), harmful drinker (zone III-score from 16 to 19 points) and probable dependence (zone IV-score from 20 to 40 points)14.
Individuals who obtained scores corresponding to zones III and IV on the AUDIT received orientations on site about the harmful effects of alcohol, mainly regarding driving; and were also referred, if wanted, to the Study, Research and Rehabilitation Center for Alcohol and Addiction (CEPRAL), developed at the Teaching Hospital São Francisco de Assis (HESFA).
The researcher collected the data in September and October 2011, which were digitalized and electronically processed in Epi-info version 3.5.1. Uni and bivariate analyses were applied to the study population. Pearson's chi-square test was used to assess the association between the categorical variables. Statistical significance was set at 5%.
This study received approval from the Research Ethics Committee at Anna Nery School of Nursing under protocol 065/2011, on August 16th 2011.
RESULTS AND DISCUSSION
Regarding the use of alcoholic beverages, most of the interviewees, i.e. 242 (62.1%) informed using this substance, while 148 (37.9%) reported not consuming alcohol, according to Table 1.
TABLE 1
: Declared alcohol use among motor vehicle drivers at an Office of DETRAN-RJ. Rio de Janeiro, RJ, Brazil – 2011. (N=390)
Concerning the alcohol consumption pattern of the drivers who mentioned using this substance, according to the AUDIT, 178 (73.6%) were classified as low-risk drinkers, followed by 55 (22.5%) as hazardous drinkers, six (2.5%) as harmful drinkers and three (1.2%) as probable dependent drinkers, as shown in Table 2.
TABLE 2:
Description of alcohol consumption patterns among motor vehicle drivers who mentioned alcohol consumption at an Office of DETRAN-RJ, Rio de Janeiro, RJ,
Brazil – 2011 (N= 242)
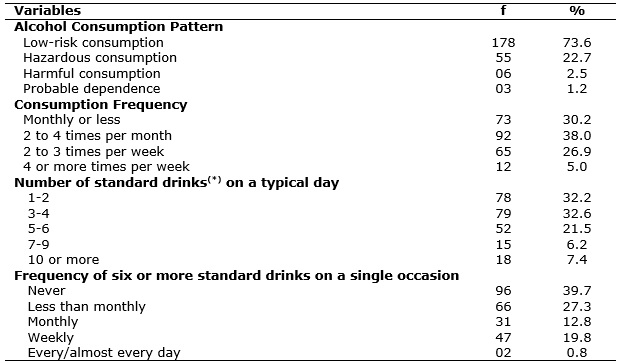
(
*) A standard drink is equivalent to 350ml of beer or 40ml of spirits or 150ml of wine.
Regarding the frequency of alcohol use, 65 (26.9%) mentioned drinking two to three times per week and 12 (5%) declared drinking four or more times per week. As for the number of standard drinks consumed on a typical day, 52 (21.5%) affirmed having five to six standard drinks, followed by 15 (6.2%) having seven to nine standard drinks and 18 (7.4%) ten ore more standard drinks. Concerning the frequency of six or more standard doses on a single occasion, 47 (19.8%) said doing this weekly, followed by two (0.8%) who informed drinking every or almost every day, according to Table 2.
Among the participants who drank and drove after the enactment of the Dry Law, 37 (50.7%) were classified under low-risk consumption and 36 (49.3%) under problematic alcohol consumption according to the AUDIT, that is, they were considered hazardous or harmful drinkers or probable dependents (p=0.00).
TABLE 3:
Association between drinking and driving after the Dry Law and the alcohol consumption pattern with the risk levels of the AUDIT, as referred by
motor vehicle drivers at an Office of DETRANRJ, Rio de Janeiro, RJ, Brazil – 2011 (N=231)
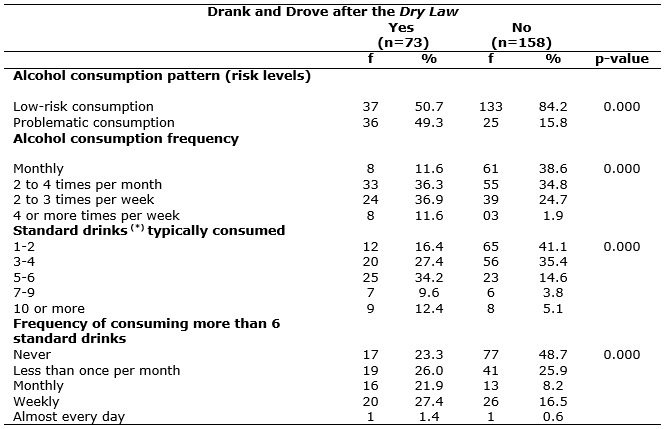
(
*) A standard drink is equivalent to 350ml of beer or 40ml of spirits or 150ml of wine.
As for the frequency of alcohol use, it was identified that, among the drivers who mentioned having drunk and driven after the Dry Law, eight (11.6%) mentioned drinking four or more times per week. Among the drivers who informed no drinking and driving after the Dry Law, this frequency dropped to three (1.9%). Concerning the standard drinks consumed on a typical day, among the drivers who mentioned drinking and driving after the Dry Law, seven (9.6%) declared having seven to nine standard drinks when compared to drivers who drank but did not drive after that law (p=0.00).
What the consumption of six standard drinks or more is concerned, it was observed that the participants who drank and drove tended to do this more frequently when compared to drivers who drank but did not drive after the Dry Law (p=0.00), as demonstrated in Table 3.
In this study, most of the population mentioned drinking, and a significant proportion of consumers with alcohol abuse was identified according to the AUDIT.
Alcohol is a culturally accepted drug, but experts draw attention to the fact that alcohol consumption is progressively increasing in Brazil. In the 1970's and 1990's, alcohol consumption grew by more than 70%15. Similarly, the II Household Survey on Psychotropic Drug Use in 2005 identified alcohol as the most used drug in the Brazilian population16.
Thus, the proportion of alcohol consumers in this study is similar to a study on the alcohol consumption pattern of the Brazilian population (52%) 17. When compared to other studies involving motor vehicle drivers, similar proportions were found15,18.
Nevertheless, no further Brazilian studies were found that estimated the prevalence of alcohol use among motor vehicle drivers, but an alcohol use pattern similar to the profile of the Brazilian population is supposed.
Also regarding the alcohol consumption pattern, this research found a significant part of drivers classified as harmful drinkers and probable dependents. Nevertheless, in comparison with other publications on the alcohol consumption pattern among drivers, the population in this study showed a lower frequency of harmful consumers7,18.
In general, the numbers of alcohol-dependent drivers, harmful drinkers or hazardous drinkers are preoccupying data, as the literature appoints that there are drivers circulating on the Brazilian highways who are classified as problematic alcohol drinkers, representing great chances of car accidents.
In that sense, a study at emergency services in Peru demonstrated a strong association between having a problematic alcohol consumption pattern (AUDIT >8), and having drunk within six hours before the trauma19.
It should be highlighted that, in this study, beyond a significant frequency of drivers with problematic alcohol use, a relevant proportion of individuals was also identified who declared drinking almost every day and who drive motor vehicles.
This underlines that health professionals should advise and sensitize the population better about the risks and harms of driving under the influence of alcohol, as described in the National Alcohol Policy12 and the National Agenda of Priorities in Health Research13.
In addition, these study findings evidenced a relevant proportion of drivers who declared binge drinking on a single occasion, in line with other epidemiological studies, although with other research subjects7,15,17,20. As mentioned, binge drinking is related to different harmful consequences for individuals predisposed to some diseases, such as alcoholic hepatitis for example.
Binge drinking is related to increased accident risk, dependence and the worsening of diseases17. In that sense, the accidents that stand out due to binge drinking on a typical day are – drowning, run overs and car accidents. In addition, it is highlighted that 28% of the Brazilians have already experienced binge drinking.
Experts emphasize that one measure to prevent binge drinking could be raising the price of these drinks21. Therefore, effective strategies should be devised for this alcohol consumption patterns to be less common among Brazilian drivers, either through educational or supervisory policies. Hence, health professionals, including nurses, need to promote effective actions to prevent binge drinking and its health problems.
In that context, health professionals are responsible for the public health policies on alcohol and traffic, concerning emergency care as well as health promotion, and overall in primary health care.
The decision to drink and drive is also related to the circle of friends. Drivers who submit to drinking and driving are influenced by their social context and by their friends. In one study that intended to investigate the variables associated with the decision to drink and drive, it was verified that drivers who will drive a short distance are more prone to drinking than drivers who intend to driver far. It was also evidenced that drivers who mentioned drinking weekly are more prone to drinking and driving. In addition, they highlighted that, if the drivers know that this act will culminate in detention, this will imply the decision not to drink and drive22, that is, if supervision is effective, it is believed that this situation will tend to decrease.
In that sense, a study developed at DETRAN-SP before the enactment of the Dry Law found a considerable number of future drivers who admitted being prone to drinking and driving and highlighted that the increased probability of being detained by the police and/or receiving legal penalties would imply the decision to drink or not and to drive23.
Nevertheless, other Brazilian studies after the Dry Law appoint that many drivers still decide to drink and drive, like in a study involving drivers who attended a bar in Porto Alegre in 2009, 51% drank and went out to drive15.
The State of Rio de Janeiro has been the Brazilian state that managed to reduce its morbidity and mortality rates in traffic the most. Within one year after the implementation of the Dry Law, the state cut down on its mortality in traffic by 32%24. It is highlighted that, since the first month after the enactment of this law, morbidity and mortality in traffic was already significantly reduced (12.9%)25.
The behavioral change among drivers in terms of alcohol use is a gradual process, which requires efforts from the public power through the encouragement of commercials on if you drink, don't drive, disclosure of information on the harm of alcohol before driving, supervision and punishment of drivers who break the law.
Unfortunately, however, not all Brazilian states have been able to reduce their morbidity and mortality in traffic. In the State of São Paulo, the Military Police disclosed that the number of drivers under the influence of alcohol caught during unexpected controls increased by 38% in comparison with 2010 18.
Similarly, the director of the Brazilian Association of Traffic Medicine highlights that the supervision of the Dry Law in Brazil remains precarious 18. Therefore, education and awareness-raising actions on safe traffic in society need to be expanded and strengthened even further, mainly with regard to alcohol and driving. In addition, the supervisory measures of Law 11.705/08 need to be observed permanently all over the country, following the example of the city of Rio de Janeiro through Operation Dry Law, implemented by the State Government.
If the managers do not adopt the Law on Zero Alcohol Use, broadening and promoting effective actions to supervise that law, its compliance will be further weakened and the morbidity and mortality statistics in traffic will tend to rise progressively.
When comparing the frequencies of drivers who declared drinking and driving in this study after the Dry Law (Law 11.705/08) with studies undertaken before 2008, reductions in this behavior are observed25,26.
Experts also recommend adopting the five steps to reduce the morbidity and mortality of traffic accidents: information, education, awareness raising, supervision, punishment27.
It is highlighted that Brazil takes part in the decade of road safety (2011-2020), in which the member countries have committed to reducing their morbidity and mortality rates in traffic. One of these initiatives is the Project Life in Traffic, launched in 2010, which intends to reduce injuries and deaths in traffic6.
CONCLUSION
Concerning the policies for the prevention of traffic deaths and injuries or social damage resulting from alcohol consumption, all sectors, mainly education and health, need to engage, whether private, public or philanthropic, as this behavioral change is a public and social responsibility.
In that sense, research on the association between alcohol and violence, such as traffic accidents, should continue to be undertaken and encouraged in order to be able to identify and discuss problems that can be overcome, such as traffic violence associated or not with alcohol use, mainly considering the International Decade of Action for Road Safety (2011-2020), strengthening the country's commitment to reduce its accident rates.
REFERENCES
1.World Health Organization. Global status report on road safety. Time for action. Geneva (Swi): WHO; 2009.
2.Organização Pan-americana de Saúde. Primera semana mundial de las naciones unidas sobre la seguridad vial. Tradução do original em inglês. Washington (D.C): OPAS; 2007.
3.Organização Mundial de Saúde. Primera conferencia ministerial mundial sobre seguridad vial: es hora de actuar Moscú, 19-20 de noviembre de 2009. Geneva (Swi): WHO; 2009.
4.Organization of the des Nations United. Global road safety crisis. Report of the secretary general. New York (UN): ONU; 2003.
5.Make Roads Safe [site da internet]. A decade of action for road safety 2011-2020. [cited in 2015 Oct 10]. Dísponível em: http://www.makeroadssafe.org.
6.Ministério da Saúde do (Br). Década de ação para a segurança no trânsito 2011-2020. [cited in 2015 Oct 10]. Disponível em: http://www.portal.saude.gov.br.
7.Domingos JBC, Pillon SC. O uso de álcool entre motoristas no interior de São Paulo. Rev enferm UERJ. 2007; 15: 393-9.
8.Abreu AMM, Lima JMB, Griep RH. Acidentes de trânsito e a frequência dos exames de alcoolemia com vítimas fatais na cidade do Rio de Janeiro. Esc Anna Nery. 2009; 13: 44-50.
9.Mariscal IMP, Silva EC. Accidentes de tránsito y el consumo de alcohol en una unidad de urgencia de La Paz, Bolivia. Rev Latino-Am Enfermagem. 2010;18: 613-9.
10.World Health Organization. Drinking and Driving: a road safety manual for decision makers and practitioners. Geneva (Swi): WHO; 2007.
11.Ministério das Cidades (Br). Departamento Nacional de Trânsito. Política nacional de transito. Brasília (DF): Gabinete Ministerial; 2004.
12.Governo Federal (Br). Decreto Nº 6.117 de 22 mai. de 2007. Aprova a política nacional sobre o álcool, dispõe sobre as medidas para redução do uso indevido de álcool e sua associação com a violência e criminalidade, e dá outras providências. [citado em 10 out 2015]. Disponível em: www.planalto.gov.br.
13.Ministério da Saúde (Br). Secretaria de ciência, tecnologia e insumos estratégicos. Agenda nacional de prioridades de pesquisa em saúde. Brasília (DF): Departamento de Ciência e Tecnologia: 2008.
14.Barbor TF, Biddle JCH, Saunders JB. AUDIT. Teste para identificação de problemas relacionados ao uso de álcool. Roteiro para uso em atenção primária. Faculdade de Medicina de Ribeirão Preto (SP): Universidade de São Paulo; 2003.
15.Pechansky F, Duarte PCAV, Boni RB (organizadores). Uso de bebidas alcoólicas e outras drogas nas rodovias brasileiras e outros estudos. Porto Alegre: Secretaria Nacional de Políticas sobre Drogas; 2010.
16.Secretaria Nacional de Políticas Antidrogas (Br). II Levantamento domiciliar sobre uso de drogas psicotrópicas no Brasil. Brasília (DF): SENAD; 2005.
17.Secretaria Nacional de Políticas Antidrogas (Br). I Levantamento nacional sobre os padrões de consumo de álcool na população brasileira. Brasília (DF): SENAD; 2007.
18.Leão AL. Mais da metade dos motoristas do país bebe, diz associação de medicina de tráfego [citado em 04 out 2015]. Disponível em: http://www.noticias.r7.com.
19.Fiestas F, Ponce J, Gallo C, Bustamante I, Ordóñez C, Mazzotti G. Factores predictores de uso problemático de alcohol en personas atendidas en una sala de emergencia. Rev Peru Med Exp Salud Publica. 2011; 28: 54-61.
20.Silveira CM, Silveira CC, Silva JG, Silveira LM, Andrade AG, Andrade LHSG. Epidemiologia do beber pesado episódico no Brasil: uma revisão sistemática de literatura. Rev Psiquiátrica clínica. 2008; 35: 31-8.
21.Annderson P, Chisholm D, Fuhr DC. Alcohol and global health. Effectiveness and cost-effectiveness of policies and programmes to reduce the harm caused by alcohol. Lancet . 2009; 373:2234-46.
22.Gustin JL, Simons JS. Perceptions of level of intoxication and risk related to drinking and driving. Addict Behav. 2008; 33: 605-15.
23.Pinsky I, Labouvie E, Laranjeira R. Disposição e alternativas ao dirigir alcoolizado entre jovens paulistas. Rev Bras Psiquiatr. 2004; 26: 234-41.
24.Lopes CA. Coordenação Geral da Operação Lei Seca. Operação Lei Seca. Nunca dirija após beber. Rio de Janeiro: DETRAN; 2010.
25.Abreu AMM, Jomar RT, Thomas RGF, Guimarães RM, Lima JMB, Figueiró RFS. Impacto da lei seca na mortalidade por acidentes de trânsito. Rev enferm UERJ. 2012; 20: 21-6.
26.Moura EC, Malta DC, Neto OLM, Penna GO, Temporão JG. Direção de veículos motorizados após o consumo abusivo de bebidas alcoólicas, Brasil, 2006 a 2009. Rev Saúde Pública. 2009; 43: 891-4.
27.Lima JMB, Abreu AMM. Fórum sobre a Lei Seca (Lei nº 11. 705 / 2008). Rio de Janeiro: Universidade Federal do Rio de Janeiro; 2012.