Source: Patients' charts. Medical Records Service/Reference Hospital/Pernambuco.
RESEARCH ARTICLES
Clinical and epidemiological characteristics of motorcyclists with traumatic brain injuries treated at a referral hospital
Mariana Sousa Arruda BarrosI; Betise Mery Alencar S.M. FurtadoII; Cristine Vieira do BonfimIII
I
Nurse from the Faculdade de Enfermagem Nossa Senhora das Graças da Universidade de Pernambuco. Nurse of the Hospital da Ilha do Leite. Recife, Pernambuco,
Brazil. E-mail: mari.arruda03@gmail.com
II
PhD in Public Health. Associate Professor of Faculdade de Enfermagem da Universidade de Pernambuco (UPE), Professor of Postgraduate Program in Forensic
expertise of Universidade de Pernambuco, Recife, Pernambuco, Brazil. E-mail: betisemery@gmail.com
III
PhD in Public Health. Research Associate of Fundação Joaquim Nabuco. Professor of Program Postgraduate Integrated in Public Health of Universidade Federal
de Pernambuco. Recife, Pernambuco, Brazil. E-mail: cristine.bonfim@uol.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2015.8036
ABSTRACT
This descriptive study of clinical and epidemiological features of motorcyclists with traumatic brain injury (TBI) analyzed data from 564 medical records of motorcyclists treated at a public referral hospital in Pernambuco State from November to December 2012. Most of the motorcyclists were male (84.05%), single (86.87%), and aged 15-34 years (72.8%). The main impact type was falls (292; 51.6%) and most TBIs were mild (415; 73.60%). Death occurred in about 5% of cases, and 465(82.44%) were discharged from the clinic. It was concluded that this information can assist in organizing emergency care services and implementing accident prevention strategies.
Keywords: Traffic accidents; traumatic brain injury; motorcycles; emergency hospitals.
INTRODUCTION
Accidents involving motorcyclists have become an important public health issue, especially the fatal ones. The number of two-wheeled vehicles has been acknowledged to be growing throughout the world. In comparison to other vehicles, motorcycles are cheaper and, therefore, represent a significant share of the market. Both mobility and speed are compelling factors to use them for work or leisure.1
Motorcycles are considered one of the most dangerous modes of motorized transportation due to the small size of the vehicles, thus, motorcyclists represent a group more vulnerable to multiple traumas of greater severity due to direct impact exposure. 2,3 Indeed, the motorcycle does not have the same structure and protection devices a car does, which allows for greater exposure of its riders. 4 Unlike what happens in car accidents, in motorcycle accidents, the pilots often absorb all of the kinetic energy and compression resulting from the accident.2
Motorcyclists suffer from a risk of death by accident, per mile traveled, thirty times higher than drivers of other kinds of motorized vehicles. 5 A study which analyzed the factors increasing the risks of motorcyclists compared to the risks of car drivers identified the chances of a motorcyclist involved in an accident to suffering from fatal or severe injuries as eight times higher than those of a car driver.4
Traumas caused by motorcycle accidents are extensive, costly and expansive. In motorcycle accidents, injuries in the lower members are more common; however, head injuries are more frequent in fatal accidents. It is estimated that head injuries correspond to 50% of deaths caused by motorcycle accidents, and in 1/3 of the victims, the head is the only wounded organ.6 In Brazil, a research into the epidemiological aspects of deaths caused by motorcycle accidents has identified skull fracture as the most common injury despite the mandatory use of helmets.1
Taking into consideration the growing number of victims involved in motorcycle accidents and the severity of injuries, especially traumatic brain injuries, as causes of morbidity and death, the goal of this study was to describe the clinical and epidemiological characteristics of motorcyclists with traumatic brain injuries who have been attended at a reference hospital. That information may aid in implementing measures for prevention and care.
LITERATURE REVIEW
Traffic accidents and the resultant deaths constitute a serious world health issue. There were 1.24 million deaths on roads around the world in the year of 2010, with over 50 million people wounded; we may add to that, an increase of 15% in the number of registered motorized vehicles to that scenario. Most of those deaths lie between the groups of most vulnerable users (pedestrians, cyclists and motorcyclists). Currently, motorcyclists represent 23% of the number of deaths in traffic accidents around the world.7
In the last decades, Brazil has slowly taken position among the world champions of traffic accidents.8 The death rate for land transport accidents (LTA) between 2000 and 2010 varied from 18 to 22.5 deaths per 100 thousand inhabitants, representing an increase of 22.54%.9 In addition to the social relevance of those accidents, the economic impact on the country has to be considered. LTAs represented 15% of the number of hospitalizations for external causes in public hospitals in the period ranging from 2002 to 2011.10 According to Datasus (the Brazilian state department of computer records for the public health system), medium- or long-term medical hospitalizations caused by traffic accidents alone represent an expense of R$187 million, not counting medical care for victims who are not hospitalized.11
The high traffic-related morbidity and death rates in Brazil have been associated with the model chosen for the transportation system, which prioritizes roads and usage of private vehicles without providing an adequate infrastructure, combined with a lack of inspection and the precariousness of public transport.9 The increase in the number of vehicles in urban centers, the scarcity of regulatory and educational measures, and the high speed and diversity of the types of vehicles should also be considered.12,13
Currently, the most frequent kind of LTAs involve motorcycles.7 There has been a rapid growth in the usage of two-wheeled motorized vehicles in several countries, which has been followed by an increase of injuries and deaths among users.14 Head and neck injuries constitute the main causes of severe injuries, disability and death among motorcycle users.12-15 In European countries, skull fractures contribute to approximately 75% of deaths among motorcycle users; in some low- and medium-income countries, head injuries are estimated to be the cause of up to 88% of such deaths. 7
Motorcycle riders represent the greatest risk of death among all traffic victims in Brazil, with 5.7 deaths per 100,000 inhabitants.9 A research developed by IPEA (the Institute of Applied Economic Research) estimates that a patient who has been the victim of a motorcycle accident costs, on average, R$152 thousand to the public purse with hospital bills alone; the social cost, in turn, is R$952 thousand on average, which includes pre-hospitalization care, hospitalization, license, early retirement, among others.16
In the State of Pernambuco, the death ratio for motorcyclists went up from 0.4/100 in 1996 to 5.7/100 thousand inhabitants in 2009.16 DETRAN-PE (the Traffic Department of the State of Pernambuco) has observed an increase in the motorcycle fleet: starting with 144,804 in the year 2000, that number reached 639,406 ten years later.16 This increase predisposes towards motorcycle accidents, which, when they do not result in death, often disables the riders. Compensation for personal damages caused by land automotive vehicles paid by (DPVAT) – a mandatory insurance for permanent disability to victims of accidents involving such vehicles – increased 274% in the case of motorcycles between the years 2000 and 2010. 17
Studies conducted locally highlighted motorcycles among LTAs.18,19 In the city of Olinda (PE), aiming to characterize the epidemiological profile of traffic victims, it has been identified that, among the types of vehicles involved in the accidents, 57.4% of them were motorcycles. 18 At Hospital Regional do Agreste de Pernambuco (HRA), located in the city of Caruaru, where it was sought to identify the prevalence of traumatic brain injuries (TBI) and related factors in victims, it has been observed that 20% of the cases were caused by motorcycle accidents.19
Considering the relevance of accidents with motorcyclists in the context of LTAs and that traumatic brain injuries are the most frequent causes of death among injured motorcyclists, the description of clinical and epidemiological characteristics of motorcyclists attended at the main reference hospital belonging to the public health service of the State of Pernambuco who suffered from traumatic brain injuries will provide information that may guide preventive and auxiliary measures.
METHODOLOGY
Research was descriptive, retrospective and documental, and was conducted at Hospital da Restauração (HR), located in Recife, Pernambuco, selected for being the state's biggest public healthcare unit, and also for being the biggest and most complex trauma and emergency care service in the Northern and Northeastern regions of Brazil. It is a reference in high-complexity care, such as cases of victims of traffic accidents in the specialties of orthopedic surgery, general surgery, peripheral vascular surgery, neurosurgery, neurology and oral and maxillofacial surgery.
Data was gathered based on reports issued by the hospital's computerized attendance system (SOUL MV/2010) listing all attendances involving motorcycle accidents as the reason for admission, enabling search queries of all patients' charts. All patients treated in the hospital during the period of November through December 2012 for motorcycle accidents, having TBI as an initial diagnosis, were included. Out of a total of 620 charts, 33 were excluded for not having an initial diagnosis of TBI, and 23 for not being found, resulted into samples of 564 charts.
The data was collected from the charts in the hospital's medical records service (SAME) from January to March, 2013. To do so, a specific form was used, where socio-demographic (gender, age, marital status and place of origin), accident-related (day of the week, shift of the occurrence and type of impact), and attendance - and trauma-related variables (mode of transportation to reach the hospital, radiograph, CT scans, MRI scans, other traumas, specialty, TBI's severity and recovery rate) were studied. To analyze the severity of the victims' states, the Glasgow Coma Scale (GCS), the clinical indicator most commonly-used to quantify a TBI's severity, was employed. The following scores were used to classify the trauma's severity: Heavy – 3 to 8; Moderate – 9 to 12; Light – 13 to 15. Due to a lack of information provided by the patients, the following variables could not be analyzed: level of education (99.82% did not inform it), occupation (95.57%), driver's license (100%), victim's position in the motorcycle (87.59%), and helmet usage (82.80%).
The gathered data was codified and processed in the program EpiInfo version 7, after which a descriptive statistical analysis of the variables (distribution of frequencies and measurement of central tendency) was performed.
This research project was evaluated and approved by the Committee of Ethics in Research of Complexo Hospitalar do Hospital Universitário Oswaldo Cruz/Pronto Socorro Cardiológico de Pernambuco – HUOC/PROCAPE (CAEE no. 04425112.8.0000.5192).
RESULTS AND DISCUSSION
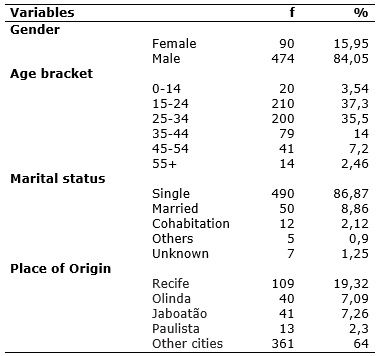
The information from 564 patients' charts was collected, most of them belonging to males – 474 (84.05%), age ranging from 15 to 34 years old – 410 (72.8%), averaging from 28 to 92 years old, varying between three and 88 years old, singles – 490 (86.87%), originating from various cities in the State of Pernambuco, according to Table 1.
TABLE 1:
Sociodemographic characteristics of victims with traumatic brain injury caused by motorcycle accidents attended at the reference hospital. Pernambuco,
2012. (N=564)
Source: Patients' charts. Medical Records Service/Reference Hospital/Pernambuco.
A prevalence of young adult males was observed in motorcycle accidents. It is worth pointing out that several national and international studies that have analyzed the profile of motorcycle accidents also identified a prevalence of young men.3,20-22 It should be pinpointed that the prevalence of young adults significantly impacts the economy, due to the fact these accidents attack individuals of working age.23
This profile is probably a consequence of the social and cultural behavior of young people, who expose themselves more to risky situations when driving vehicles: inexperience, high speed, impulsiveness, employment of riskier maneuvers in search of thrills, alcohol consumption.23 Indeed, the combination of age, low experience, risky behavior and unsafe attitudes are factors which contribute to accidents taking place.24 A study conducted in Italy has shown that the more experienced a driver is, the less dangerous the risky situations are.24
The day of the week with the highest number of attendances was Sunday – 135 (23.93%), mainly during the evening – 234 (41.50%), as seen in Table 2.
TABLE 2:
Characteristics of motorcycling accidents recorded during care at the reference hospital. Pernambuco, 2012. (N=564)
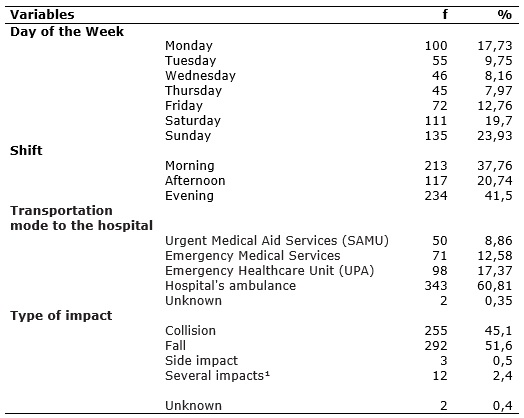
¹Several impacts = More than one impact, for instance: collision x head-on, side x collision, among others.
Source: Patients' charts. Medical Records Service/Reference Hospital/Pernambuco.
The characteristics of the accident related to the day of the week in which they took place point to an increase of the number of victims starting on Friday, reaching a higher number on Sunday. A research which analyzed the profile of multiple traumas in motorcyclists treated by the Urgent Medical Aid Services (SAMU) attributes the higher frequency of accidents during weekends to the high number of festive events, alcohol consumption, violation of speed limits, risky maneuvers and a decrease in traffic policing.23 Another study revealed that motorcyclists are three times more likely to get involved in accidents between Thursday and Sunday due to alcohol consumption than between Monday and Wednesday, when said consumption decreases. 25
In this research, over 40% of attendances happened after nightfall. Such a fact may be explained by various factors, which are: nighttime fatigue, an increase in the flow of vehicles, varying visibility limited by the headlights' range, a lack of signaling when overtaking, decreased traffic policing, violation of traffic lights, speeding and alcohol or drug consumption.23,25,26 There are human, environmental and mechanical factors which contribute to the risk of traffic accidents, since exhaustion and work overload also lead to human error.27
The hospital studied underwent changes in the manner of attendance to spontaneous demand, which no longer has access to medical services, since admission is gtanted by means of referral from the State's Office of Hospital Beds Regulation. Victims from other cities close to Recife, referred by healthcare units by means of hospital beds' regulation, appear in first place, with 361 (64%) attendances; the hospital's ambulance was the most employed mode of transportation - 343 (60.81%).
Based on place of origin, the study brought to light important differences in the satisfied demand when compared to the results of a research on attendance by the same hospital in 2004, showing that over 90% of attendances came from Recife,28 which differs from the current study, in which only 109 (19.32%) came from the capital.
Emergency healthcare units (UPA) sent approximately 98 (17.4%) of the patients, a result which displays the change in the emergency assistance network in Recife with the implementation of those units, starting in 2009, by the Ministry of Health in cooperation with the State; said units being defined as healthcare facilities of intermediate complexity between basic health / family health units and the hospital network, composing an organized network of urgent care notice.28,29
The type of impact most commonly observed was the motorcycle fall – 292 (51.6%), followed by collision – 255 (45.1%), as seen in Table 2. A research which evaluated facial traumas caused my motorcycling accidents also pointed out that falling off the motorcycle as the most frequent type of accident. 26 Other studies have indicated the collision between motorcycles and automobiles and between motorcycles as the primary mechanisms for accidents.1,30-32 A study which evaluated the risk of injuries in motorcyclists revealed that those involved in collisions presented 11.19 times higher chances of suffering injuries than those which hit pedestrians, animals or cyclists.21
A research which analyzed fatal motorcycle accidents concluded that collisions involving motorcyclists frequently result in death.1 One of the primary factors in vehicle collisions consists of high speed by the vehicle at the moment of the accident. There are three distinct moments involved in those accidents which have been identified: when the vehicle collides with another vehicle or object; when the riders collide with their own vehicle or some obstacle; and when the victim's internal organs collide with each other, or with the organism's walls, due to deceleration, leading to a rupture of organs. Thus, the probability of injuries and death is high, considering the three simultaneous opportunities for trauma to occur.21
Considering the correlated traumas, it can be seen that 263 (57.18%) of motorcyclists presented facial trauma, as described in Table 3. In motorcycle accidents, lower member traumas are more frequent,31 however, head and neck injuries are more severe,15 and traumatic brain injuries are the leading causes of death.20 A research that studied facial trauma and the risk of intracranial injuries in motorcyclists identified the presence of facial fractures which increase the risk of a traumatic brain injury.33
TABLE 3:
Clinical characteristics of victims with traumatic brain injuries caused by motorcycling accidents. Reference hospital, Pernambuco, 2012. (N=564)
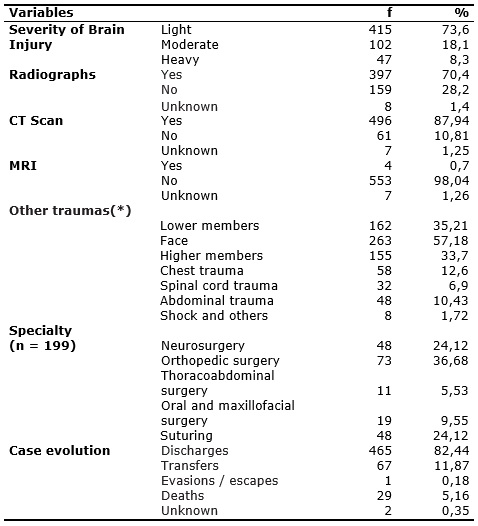
(*) Other traumas are valued as n= 460, more than one option could have been marked in this variable.
Injuries caused by traffic accidents with motorcycles have been leaving many fully active young people unfit for work and study, besides death and disability.34 It must be emphasized that the areas of the body usually hit are: head, face, and upper and lower members in traffic accidents, the most relevant ones which often determine if the individual is fit for activities or not. The analysis of patients who were victims of motorcycle accidents treated at a center of reeducation and rehabilitation has identified traumatic brain injuries as the prevailing neurological injury. Those injuries are associated with a vast number of disabilities, resulting into a delayed or even uncertain return to productivity.35
In this study, approximately 32 (6.9%) victims suffered a spinal injury, according to Table 3. A research in the clinical and epidemiological aspects of patients suffering from spinal cord traumas attended at an emergency hospital in the city of Petrolina (PE) has identified motorcycle accidents as the most frequent etiology of trauma. Spinal cord trauma causes physical disability and economic costs, standing out as a relevant health issue in Brazil. 36
Regarding the severity of the victims' states, based on the ECG value, 415 (73.60%) of the treated patients were noted to be classified as light TBI, as described in Table 3. Similarly, a study on the TBIs of victims of motorcycle accidents identified that approximately 415 (70%) cases as light TBI. 32
In the present study, only 47 (8.30%) patients were deemed as heavy severity, according to Table 3. TBIs of moderate and heavy severity are associated with neurological conditions and functional impairments.37 TBIs impact the population's health and quality of life. A research on the costs of traumatic brain injuries resulting from motorcycling accidents in Hanoi, Vietnam, revealed high costs which increased with the severity of the TBI. There is a significant burden on patients and their families due to direct high costs and the loss of income from the reduced workload.38
The literature denotes that usage of helmets reduces the occurrence of serious injuries, death rates and the need for hospitalization in motorcycle accidents.39 An analysis of the profile of victims of trauma caused by motorcycle accidents who were attended at a public emergency service showed 23.7% suffered traumatic brain injuries, displaying double the chances of developing injuries than those who wore helmets.20 In this study, no records on helmet usage was found in the patients' charts; for that reason, this variable was not studied.
A total of 397 (70.40%) and 496 (87.94%) radiographies and skull tomographies, respectively, were performed, according to Table 3. Computerized tomography (CT) is the imaging exam of choice to confirm a TBI diagnosis in the emergency room. By means of this exam, bruises may be quickly diagnosed, favoring, when so indicated, early surgical treatment.27,40 This study has ascertained that most victims underwent skull tomographies – 496 (87.94%), while only 4 (0.70%) underwent magnetic resonance, which is in accordance with what is expected, since it is not an exam for urgent detection of TBIs; such findings verify the results of another study.40
Analyzing the surgical specialties, it can be seen that 73 (36.68%) were related to orthopedics. It should be noted that 465 (82.44%) cases recovered enough to be discharged, and the register of 29 (5.16%) deaths, of the total amount, as observed in Table 3. The information related to surgical procedures are compatible with the traumas found; in other words, most performed orthopedic and neurosurgical procedures befitting the injuries detected in the head and the members.20
The rate of death ascertained was lower than the one described by other studies.32,37 It should be noted that 67 (11.87%) patients were transferred to other units, probably because of correlated traumas, since the studied hospital is a reference in the field of neurosurgery. Out of the 29 (5.16%) victims who died, most of them were young adult males whose accidents in their majority took place from Friday to Monday during the evening, with over 24 (85%) of the victims presenting an initial ECG of moderate or heavy severity, of which seven reported alcohol consumption. During attendance, 13 required a surgical procedure, and 23 more (80%) revealed other traumas in addition to a TBI.
As a limitation of the study, the quality of the records should be mentioned, since their omissions of some variables prevented the description of the profiles of motorcyclists who were victims of accidents from being improved.
CONCLUSION
In this study, it has been observed that the motorcyclist's profile is predominantly male, single, 15-34 years old and motorcycle falls as being the main type of impact. By means of the GCS, the prevalence of light trauma was also noticed. Most patients improved and were released from care, and death occurred to a small percentage of the cases. The study was proven relevant for describing the clinical and epidemiological characteristics of motorcyclists with traumatic brain juries, clarifying variables of this phenomenon. These data may contribute to an advance in health care and research, besides assisting with the organization of a network of emergency care and the implementation of accident prevention strategies.
REFERENCES
1.Carrasco CE, Godinho M, Barros MBA, Rizoli S, Fraga GP. Fatal motorcycle crashes: a serious public health problem in Brazil. World J Emerg Surg [PubMed-US National Library of Medicine]. 2012 [cited in 2015 Mar 12], 7(Suppl1):S5. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3424925/.
2.World Health Organization. World Report on Road Traffic Injury Prevention: Summary. Geneva: World Health Organization; 2004 [cited in 2015 Abr 20]. Available from: http://www.who.int/violence_injury_prevention/publications/road_traffic/world_report/summary_en_rev.pdf .
3.Golias ARC, Caetano R. Accidents between motorcycles: analysis of cases that occurred in the state of Paraná between July 2010 and June 2011. Ciênc saúde coletiva [Scielo-Scientific Eletronic Library Online]. 2013 [cited in 2015 Mar 12]; 18: 1235-46. Available from: http://www.scielo.br/pdf/csc/v18n5/08.pdf.
4.Keall MD, Newstead S. Analysis of factors that increase motorcycle rider risk compared to car driver risk. Accid Anal Prev [PubMed-US National Library of Medicine]. 2012 [cited in 2015 Mar 12]; 49:23-9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23036378.
5.National Highway Transportation Safety Administration. Traffic Safety Facts 2010 Data: Motorcycles (Report No. DOT HS 811 639). NHTSA, National Center for Statistics and Analysis, Washington, DC, [cited in 2015 Mar 20]. Available from: http://www-nrd.nhtsa.dot.gov/Pubs/811639.pdf.
6.MacLeod JBA, DiGiacomo JC, Tinkoff G, FACS, FCCM. Helmet Efficacy to Reduce Head Injury and Mortality in Motorcycle Crashes. J Trauma [internet]. 2010 [cited in 2015 Mar 20]; 69:1101-11. Available from: http://journals.lww.com/jtrauma/Fulltext/2010/11000/An_Evidence_Based_Review__Helmet_Efficacy_to.12.aspx .
7.World Health Organization. 10 facts on injuries and violence, [cited in 2015 Mai 13]. Available from: http://www.who.int/features: factfiles: injuries:en:index.htlm.
8.Ministério da Saúde (Br). Atividades Rodoviárias. Acidentes de transito [cited in 2015 Mai 7 Mai]. Available from: http://www.atividadesrodoviarias.pro.br/acidente.htm.
9.Morais Neto OL, Montenegro MMS, Monteiro RA, Siqueira Júnior JB, Silva MMA, Lima CM et al. Mortality due to Road Traffic Accidents in Brazil in the last decade: trends and risk clusters. Ciênc saúde coletiva [Scielo-Scientific Eletronic Library Online]. 2012; [cited in 2015 Mai 18]; 9: 2223-36. Available from: http://www.scielo.br/pdf/csc/v17n9/a02v17n9.pdf.
10.Mascarenhas MDM, Barros MBA. Evolution of public health system hospital admissions due to external causes – Brazil, 2002-2011. Epidemiol Serv Saúde [Scielo-Scientific Eletronic Library Online]. 2015 [cited in 2015 Jun 18]; 24: 19-29. Available from: http://www.scielo.br/pdf/ress/v24n1/2237-9622-ress-24-01-00019.pdf.
11.DATASUS. Informação em Saúde – mortalidade por causas externas [cited in 2015 Mai 15]. Disponível em: http://w3.datasus.gov.br.
12.Hyder AA, Peden M. Inequality and road-traffic injuries: call for action. Lancet [PubMed-US National Library of Medicine] 2003; 362(9401):2034-5. [cited in 2015 Fev 05]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/14697797.
13.Lima MLC, Cesse EAP, Abath MB, Júnior FJMO. Tendência de mortalidade por acidentes de motocicleta no estado de Pernambuco, no período de 1998 a 2009. Epidemiol Serv Saúde. [Scielo-Scientific Eletronic Library Online]. 2013; 22:395-402 [cited in 2015 Mai 12]. Available from: http://scielo.iec.pa.gov.br/pdf/ess/v22n3/v22n3a04.pdf.
14.Toroyan T. Helmets: a road safety manual for decision-makers and practitioners. World Health Organization, Geneva, 2006, [cited in 2015 Fev 05]. Available from: http://www.who.int/violence_injury_prevention/publications/road_traffic/helmet_manual.pdf .
15.Talving P, Teixeira PG, Barmparas G, Dubose J, Preston C, Inaba K et al. Motorcycle-related injuries: effect of age on type and severity of injuries and mortality. J Trauma [PubMed-US National Library of Medicine]. 2010 [cited in 2015 Mar 20]; 68:441-6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20154556.
16.Pernambuco. CEPAM, Comitê Estadual de Prevenção aos Acidentes de Moto. [cited in 2015 Mai 2]. Available from: http://www.cepam.pe.gov.br/apresentacao/.
17.DENATRAN, Departamento Nacional de Trânsito. Aumento da frota de motocicleta. [cited in 2015 Mar 21]. Available from: http://www.denatran.gov.br.
18.Cabral APS, Souza WV, Lima MLC. Mobile Emergency Care Service: A survey of local land transportation accidents. Rev bras epidemiol [Scielo-Scientific Eletronic Library Online]. 2011 [cited in 2015 Mar 22]; 14: 03-14. Available from: http://www.scielo.br/pdf/rbepid/v14n1/01.pdf.
19.Ramos EMS, Silva MKB, Siqueira GR, Vieira RAG, França WLC. Epidemiological aspects of brain and head injuries treated at the Hospital Regional do Agreste de Pernambuco from 2006 to 2007. RBPS [Internet]. 2010 [cited in 2015 Mar 22]; 23: 4-10. Available from: http://ojs.unifor.br/index.php/RBPS/article/view/1164/2286.
20.Santos AMR, Moura MEB, Nunes BMVT, Leal CFS, Teles JBM. Profile of motorcycle accident victims treated at a public hospital emergency department. Cad Saúde Pública [Scielo-Scientific Eletronic Library Online]. 2008 [cited in 2015 Jun 22]; 24:1927-38. Available from: http://www.scielo.br/pdf/csp/v24n8/21.pdf.
21.Oliveira NLB, Sousa RMC. Risk for injuries among motorcyclists involved in traffic incidents. Rev Esc Enferm USP [Scielo-Scientific Eletronic Library Online]. 2012 [cited in 2015 Jun 22]; 46: 1133-40. Available from: http://www.scielo.br/pdf/reeusp/v46n5/14.pdf.
22.Chandran, Lunnen JC, Pérez-Núñez, Híjar MM, Hidalgo-Solórzano, Hyder. The prevalence of motorcycle helmet use in three mexican cities. Inj Prev [Internet]. 2012 [cited in 2015 Mar 20]; 18 (Suppl 1):A1-A246. Available from: http://injuryprevention.bmj.com/content/18/Suppl_1/A233.2.
23.Rezende NDS, Alves AKS, Leão, GM, Araújo AA. Profile of multiple trauma occurrences in motorcycle drivers attended by the SAMU of Teresina-PI. Rev bras enferm [Scielo-Scientific Eletronic Library Online]. 2012 [cited in 2015 Jun 15]; 65: 936-41. Available from: http://www.scielo.br/pdf/reben/v65n6/a08v65n6.pdf.
24.Bjornskau T, Naevestad TO, Akhtar J. Traffic safety among motorcyclists in Norway: a study of subgroups and risk factors. Accid Anal Prev [PubMed-US National Library of Medicine], 2012 [cited in 2015 Jun 3]; 49: 50-7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23036382.
25.Vieira RCA, Hora EC, Oliveira DV, Vaez AC. An epidemiological survey on motorcycle accident victims assisted at a Reference Trauma Center of Sergipe. Rev Esc Enferm USP [Scielo-Scientific Eletronic Library Online] 2011 [cited in 2015 Jun 3]; 45:1359-63. Available from: http://www.scielo.br/pdf/reeusp/v45n6/v45n6a12.pdf.
26.Brasileiro BF, Vieira JM, Silveira CES. Evaluation of facial injuries from motorcycle accidents in Aracaju/SE. Rev cir traumatol buco-maxilo-fac. [Internet]. 2010 [cited in 2015 Jun 3]; 10: 97-104. Available from: http://www.revistacirurgiabmf.com/2010/v10n2/15.pdf.
27.Veronese AM, Oliveira DLLC. Traffic accidents from the motorcycle couriers' perspective: feedback for health promotion. Cad Saúde Pública [Scielo-Scientific Eletronic Library Online]. 2006 [cited in 2015 Jun 3]; 22: 2717-21. Available from: http://www.scielo.br/pdf/csp/v22n12/20.pdf.
28.Furtado BMASM, Junior JLCA, Cavalcanti P. O perfil da emergência do Hospital da Restauração: uma análise dos possíveis impactos após a municipalização dos serviços de saúde. Rev Bras Epidemiol [Scielo-Scientific Eletronic Library Online]. 2004 [cited in 2015 Jun 3]; 7: 279-89. Available from: http://www.scielosp.org/pdf/rbepid/v7n3/06.pdf.
29.Ministério da Saúde (Br). PORTARIA Nº 1.020, DE 13 DE MAIO DE 2009. [cited in 2015 Mai 22]. Available from: http://bvsms.saude.gov.br/bvs/saudelegis/gm/ 2009 /prt1020_13_05_2009.html.
30.Rodrigues NB, Gimenes CM, Lopes CM, Silva JMR. Deaths, injuries and pattern of motorcycle accident victims in the city of Sorocaba, São Paulo, Brazil. Rev Fac Ciênc Méd [Internet]. 2010 [cited in 2015 Jun 3]; 12: 21-5. Available from: http://revistas.pucsp.br/index.php/RFCMS/article/view/2931.
31.Debieux P, Chertman C, Mansur NSB, Dobashi E, Fernandes HJA. Musculoskeletal injuries in motorcycle accidents. Acta Ortop Bras [Scielo-Scientific Eletronic Library Online]. 2010 [cited in 2015 Jun 7]; 18:353-6. Available from: http://www.scielo.br/pdf/aob/v18n6/10.pdf.
32.Canova JC, Bueno MFR, Oliver CCD, Souza LA, Belati LA, Cesarino CB, Ribeiro RCHM. Cranioencephalic trauma of patients victims of motorcycle accidents. Arq Ciênc Saúde [Internet]. 2010 [cited in 2015 Jun 7]; 17:9-14. Available from: http://repositorio-racs.famerp.br/racs_ol/vol-17-1/v17-1.htm.
33.Kraus JF, Rice TM, Peek-Asa C, McArthur DL. Facial trauma and the risk of intracranial injury in motorcycle riders. Ann Emerg Med [Internet]. 2003 [cited in 2015 Jun 3]; 41:18-26. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12514678.
34.Siscão MP, Pereira C, Amall RLC, Foss MHDA, Marino LHC. Spinal Cord Injury: Characterization at a Public Hospital. Arq Ciênc Saúde [Internet]. 2007 [cited in 2015 Jun 7]; 14:145-7. Available from: http://repositorio-racs.famerp.br/racs_ol/vol-14-3/IIIDDD195.pdf.
35.Jácomo AAE, Garcia ACF. Analysis of motorcycle accidents at the Dr. Henrique Santillo Rehabilitation and Readaptation Center (CRER). Acta Fisiatr [Internet]. 2011 [cited in 2015 Jun 12]; 18: 124-9. Available from: http://www.actafisiatrica.org.br/detalhe_artigo.asp?id=60.
36.Creôncio SCE, Moura JC, Rangel BLR. Clinical and epidemiological aspects of spinal injured patients in Hospital de Urgencias e Traumas - Petrolina, Pernambuco. Jornal Bras Neurocirurg [Internet] 2012 [cited in 2015 Jun 12]; 23: 211-6. Available from: http://www.abnc.org.br/ed_art_down.php?id=1016.
37.Ruy EL, Rosa MI. Epidemiological profile of patients with traumatic brain injury. ACM [Internet]. 2011 [cited in 2015 Jun 12]; 40: 17-20. Available from: http://www.acm.org.br/revista/pdf/artigos/873.pdf.
38.Hoang HT, Pham TL, Vo TT, Nguyen PK, Doran CM, Hill PS. The costs of traumatic brain injury due to motorcycle accidents in Hanoi, Vietnam. Cost Eff Resour Alloc [PubMed-US National Library of Medicine]. 2008 [cited in 2015 Jun 3]; 6:17. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2538497/.
39.Liu BC, Ivers R, Norton R, Boufous S, Blows S, Lo SK. Helmets for preventing injury in motorcycle riders. Cochrane Database Syst Rev [PubMed-US National Library of Medicine]. 2008 [cited in 2015 Jun 16]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18254047.
40.Morgado FL, Rossi LA. Correlation between the Glasgow Coma Scale and computed tomography imaging findings in patients with traumatic brain injury. Radiol Bras. [Scielo-Scientific Eletronic Library Online]. 2011 [cited in 2015 Jun 12]; 44:35-41. Available from: http://www.scielo.br/pdf/rb/v44n1/10.pdf.