ORIGINAL RESEARCH
Sociodemographic and epidemiological characteristic of patients in an adult intensive care unit
Odisséia Fátima PerãoI; Maria Bettina Camargo Bub II; Giseli Cristina ZandonadiIII; Magda Aparecida MartinsIV
I
Nurse. Doctoral student in Nursing. Federal University of Santa Catarina.
Florianópolis, Santa Catarina, Brazil. E-mail: odisseiaperao@gmail.com
II
Nurse. Ph.D. in Nursing. Professor at the Federal University of Santa
Catarina. Florianópolis, Santa Catarina, Brazil. E-mail: bettinabub@gmail.com
III
Nurse. Specialist in Occupational Health Nursing by Fisiomar.
Florianópolis, Santa Catarina, Brazil. E-mail: zandoseli@hotmail.com
IV
Nurse. Specialist in Occupational Health Nursing. Federal University of
Santa Catarina. Florianópolis, Santa Catarina, Brazil. E-mail: magdajem@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2017.7736
ABSTRACT
Objective: to analyze the sociodemographic and epidemiological characteristics of patients hospitalized in an adult intensive care unit (ICU) of a hospital in the Southern Region of Brazil. Method: quantitative, retrospective, descriptive study. Data were collected directly from the medical charts of 190 hospitalized patients from July to November 2012, presented in tables. Approved by the Ethics Committee of the Federal University of Santa Catarina, with the Opinion: 155,004. Results: predominant male population, aged between 50 and 59 years. The majority (93.1%) came from the Itajaí / SC micro region and the surgical center (40.3%) prevailed. Diseases of the circulatory system were the main causes and hospitalization (26.3%) and death (27.1%). The mode of stay in the ICU was from 0 to 3 days and admissions and admissions predominated in the evening period. Conclusion: the results obtained are relevant for the planning and execution of actions in intensive care units.
Keywords: Intensive care unit; descriptive epidemiology; nursing; adult patients.
INTRODUCTION
Sociodemographic and epidemiological data describe the characteristics of a population. Epidemiology is the science that studies the health-disease process in human collectivities, analyzing the distribution and the determining factors of diseases, harms to health and events associated with collective health, and suggests specific disease prevention, control or eradication measures, providing indicators to support planning, managing and evaluation of health actions1.
Epidemiological analysis in intensive care units (ICUs) must take some factors into account. One of them is related to the diagnosis of the population, that is, knowing the characteristics of the public to be assisted. This knowledge allows healthcare professionals to plan the care, regardless of the cause of admission, and make decisions to improve the quality of the assistance2.
Once the information about the population is available, a process of reflection and discussion on these data is established using the experience of the professionals involved – managers, technicians, healthcare professionals and community – to detect existing problems3. Awareness of the features of patients admitted to an ICU provides a basis that favors the diagnosis and planning of health care.
A study carried out in an adult ICU in a teaching hospital in Rio Grande do Sul with 144 patients revealed that most were elderly people, with an average age of 64.8 years4. This investigation corroborates the change in the profile of ICU adult patients that has been observed in Brazil in the past few years, attributed to a demographic and epidemiological transition. From a practical perspective, knowing these data can consolidate care strategies already in progress or help changing them according to the reality depicted in the survey.
The present study aimed at analyzing the sociodemographic and epidemiological characteristics of patients in an ICU in a hospital in the South region of Brazil.
LITERATURE REVIEW
Public health considers epidemiology a fundamental instrument in the process of identifying and mapping emerging diseases. Despite its importance, significant delays may occur in epidemiological findings and the resulting applications in the population5. This science addresses the health-illness process by studying determining factors and forms of occurrence of diseases in human populations6.
Analysis of demographic, epidemiological and organizational information from hospital care offers a basis to plan assistance and consequently improves its quality7.
With the improvement of basic sanitation in Brazil in the past decades, the death profile has changed. There was a reduction in the number of deaths caused by infectious and transmissible diseases and an increase in the number of deaths prompted by chronic diseases or associated with external factors, such as traffic accidents or violence8.
A study conducted in an ICU of a public hospital in the countryside of São Paulo showed that 64.9% of the patients were male, 20.1% were aged 40 to 49 years old, 62.9% stayed in the ICU for one to ten days and had respiratory and circulatory issues9.
Another investigation carried out in an adult ICU in a teaching hospital in Rio Grande do Sul with 144 patients reported that most were elderly people, with an average age of 64.8 years4.
A study performed in an ICU in the state of Paraíba showed that the deaths registered during the data collection were predominantly of female patients – 25 versus 2310. Knowledge of sociodemographic features is useful not just to managers that wish to improve services. It can also help advance the care to patients and relatives during hospital stay and post-discharge, define contents to prepare health education materials, train employees and develop prevention projects11.
In addition, it is necessary that professionals that work in ICUs have specific technological skills and knowledge to execute techniques and handle equipment in these units12.
These aspects expose the need to plan the care in ICUs according to the specificities of the public assisted.
METHODOLOGY
The present study was quantitative, retrospective and descriptive and its sample consisted of patients from an adult ICU in a hospital in the coast of the South region of Brazil.
The investigation was approved by the Human Research Ethics Committee of the Federal University of Santa Catarina in a report labeled 155004.
The studied population had 190 patients admitted to the ICU from July to November 2012.
The data referring to sociodemographic and epidemiological features – gender, age, marital status, city of origin, profession, origin, admission and discharge shift, type of discharge, length of hospital stay, deaths by group of diagnosis and cause of admission according to the International Statistical Classification of Diseases and Related Health Problems, 10 th revision (ICD - 10) – were collected from the patients' medical records.
Absolute and relative frequencies were calculated and organized in tables. Subsequently, statistical analyses were performed.
RESULTS AND DISCUSSION
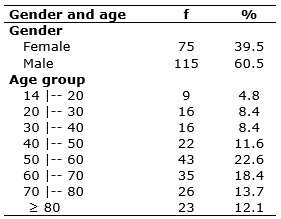
Among the 190 admissions registered during data collection, 60.5% were male patients. The predominant age group in the sample was 50 to 59 years old, with a share of 22.6%, as shown in Table 1. The predominance of men in the sample corroborated the reality observed in other ICUs. The data found are similar to the ones reported by other Brazilian studies, which also point to a prevalence of male population13, 14. This result may be explained by the increase in the number of accidents in the past years and in the rate of episodes of violence.
TABLE 1:
Demographic distribution according to gender and age of the patients
admitted to ICU 1 at HMMKB from July to November 2012. Itajaí, SC, Brazil.
(N = 190)
As for the city of origin, 177 patients or 93.1% of the sample were from the microregion of Itajaí, state of Santa Catarina. The studied ICU meets a great demand of patients from the city and region and the number of beds is insufficient; it belongs to a large institution that receives medium- and high-complexity patients through the Unified Health System (SUS), health insurance and private services. The lack of an appropriate number of ICU beds is a national problem. According to the Federal Medicine Council, most Brazilian cities do not have ICU beds either in public or private organizations15.
In the studied sample, 40.3% of the patients were sent by the surgical center, 27.7% by the emergency room, 28.3% by other units and only 3.6% were transferred from another institution. Other studies revealed similar rates; for instance, a survey carried out in two public and two private hospitals in São Paulo showed that 52.84% and 19.33% of the ICU patients originated in their own surgical centers, respectively16. A comparable result, 52.5%, was found in a hospital in Santa Catarina 7. In the institution where the study took place, patients undergo major surgeries that require intensive care, especially in the first 24 hours after the procedure. In this phase, patients present hemodynamic instability and need a rigorous monitoring of vital signs, bleeding control, removal of drains and ventilatory support, that is, continuous care that demands trained professionals.
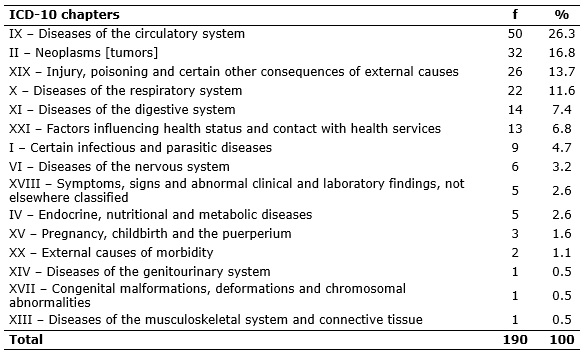
The most frequent cause of admission was circulatory issues (26.3%), followed by neoplasms (16.8%). The list also included injuries, poisoning and other consequences of external factors (13.7%) and diseases of the respiratory (11.6%) and digestive (7.4%) systems, as depicted in Table 2.
TABLE 2:
Distribution of causes of admission, grouped by ICD – 10 chapter, of
patients admitted to ICU 1 at HMMKB. Itajaí, SC, Brazil, 2012.
Several studies confirm these data. This increase in cardiovascular issues has also been observed in the elderly population, which requires more hospital interventions for being more vulnerable to cardiovascular complications17. This characteristic was evidenced in studies with patients from Sutis, in Paraíba and Pernambuco, in which most admitted patients had cardiovascular diseases18, 19. A different result was found in a retrospective study carried out in two Sutis in a hospital in the city of São Paulo, which reported a predominance of respiratory problems20. Injuries, poisoning and other consequences of external factors, among which traumas must be included, were the main cause of admission to ICUs in Maringá, state of Paraná21.
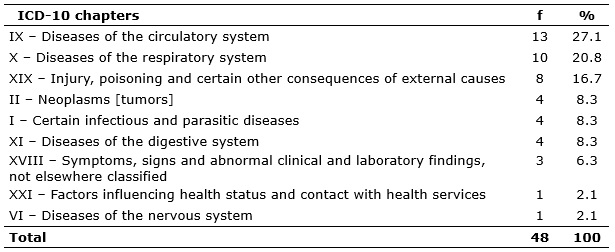
The highest frequency of deaths was related to circulatory diseases (27.1%), followed by respiratory problems (20.8%) and neoplasms (16.7%). The three first issues were responsible for most deaths (64.6%), as displayed in Table 3.
TABLE 3:
Distribution of causes of death, grouped by ICD – 10 chapter, of patients
admitted to ICU 1 at HMMKB from July to November 2012. Itajaí, SC, Brazil,
2012.
In the investigated ICU, 25.1% of the patients died and 71.2% were discharged and forwarded to other care units in the institution. These results resemble those reported in a study performed in an ICU in Florianópolis, state of Santa Catarina, which revealed death and discharge rates of 20.4% and 79.3%, respectively7. In another investigation developed in Paraíba, the findings were slightly different: 47.8% of the patients died, 50% were discharged from the ICU and 2.1% were transferred to another hospital18. In the past few years, chronic degenerative and cardiovascular diseases have become more common and lead the rates of morbidity and mortality in the present days. The present study reinforces this tendency: most deaths were provoked by circulatory and respiratory diseases. In a survey that described patients from an ICU in Rio Grande do Sul, most deaths were caused by kidney failure, respiratory issues, cardiovascular and surgical complications 22. Diversely, 51.2% of the deaths registered in the ICU of a public teaching hospital of the state of São Paulo were caused by septic shock23.
As for the length of stay, almost half the patients (47.6%) remained in the ICU for 3 days at most and 18.6% stayed from 4 to 7 days, totaling 66.2% of the sample. The mode of the length of stay was 0 to 3 days. The minimum and maximum stay lasted about 24 hours and 52 hours, respectively. A few factors influence length of stay in an ICU, such as the nature of the underlying disease and the therapeutic demands resulting from complications. Literature considers short a stay that lasts 4 days at most, and medium one that reaches 10.5 days4. Knowing the length of hospital stay is one of the relevant factors to plan care.
Nearly half the patients (46.3%) were admitted in the night shift; a similar percentage (39.5%) was found for the afternoon shift and only 14.2% were admitted during the morning shift.
This pattern was not reproduced in the discharge: 38.4% of the patients left the ICU during the afternoon (1 p.m. – 7 p.m.), 31.7% during the morning (7 a.m. – 1 p.m.) and only 12% during the night (7 p.m. – 7 a.m.). Patient turnover rates were higher during the afternoon and night.
The morning shift concentrated more deaths (31.3%), considering that it is shorter than the night shift (6 hours versus 12 hours).
Other relevant information, which is rarely found in literature, is related to the admission and discharge rates by nursing shift. These data can help design the planning of care. In the present study, most patients were admitted and discharged in the afternoon shift, a result similar to the one described in an investigation performed in an ICU in a city of the coast of Santa Catarina7.
CONCLUSION
The present study analyzed the sociodemographic and epidemiological characteristics of patients admitted to an adult ICU of a hospital in the South region of Brazil. Knowing these features precedes a proper care, together with the physical and technological resources in a health institution. These findings are relevant to plan and execute care actions in ICUs.
The results showed that the population of the ICU in question was predominantly male and belonged to the age group of 50 to 59 years. Most patients were from the microregion of Itajaí, Santa Catarina, and were sent to the ICU by the surgical center. Diseases of the circulatory system were the main cause of admission and death. The admission mode was 0 to 3 days. Most admissions took place in the night shift, whereas discharges were more common during the afternoon.
It is important to stress that the reduced time interval to collect data was a limitation of this study. Climate variations throughout the year impacted the results significantly, given that the population of the region increases during summer. The limited research field prevents the generalization of the results.
The authors suggest the development of similar investigations to increase the data about the characterization of the public assisted in ICUs. This type of research can be used as a basis for the design of evaluation and planning instruments in nursing care.
REFERENCES
1. Rouquayrol MZ, Silva MGC. Epidemiologia e saúde. 7ª ed. Rio de Janeiro: MedBook, 2013.
2. Lanetzki CS, Oliveira CAC, Bass LM, Abramovisi S, Troster EJ. The epidemiological profile of pediatric intensive care center at Hospital Israelita Albert Einstein. Einstein [Scielo – Scientific Eletronic Library Online]. 2012 [cited 2 Apr 2016]. 10 (1):16-21. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1679-45082012000100005&lng=pt .
3. Lacerda JT, Botelho LJ, Colussi CF. Planejamento na atenção básica . Florianópolis: Ed. UFSC, 2012. [cited 16 Jan 2016]. Available from: http://www.unasus.ufsc.br.
4. Favarin SS, Camponogara S. Perfil dos pacientes internados na unidade de terapia intensiva adulta de um hospital universitário. Rev Enferm UFSM [Internet]. 2012 [cited 10 Feb 2016]; (2):320-9. Available from: http://cascavel.ufsm.br/revistas/ojs-2.2.2/index.php/reufsm/article/view/5178/3913 .
5. Bonita R. Epidemiologia básica. 2ª ed. São Paulo: Editora Santos; 2010.
6. Matoso LML, Castro CHA. Indissociabilidade clínica e epidemiológica da pneumonia. Catussaba. [Repositório científico UNP]. 2013 [cited 4 Apr 2016] 2:11-23. Available from: https://repositorio.unp.br/index.php/catussaba/article/viewFile/223/284 .
7. Rodriguez AH, Bub MBC, Perão OF, Zandonadi G, Rodriguez MJH.
Epidemiological characteristics and causes of deaths in hospitalized
patients under intensive care. Rev Bras Enferm. [Scielo – Scientific
Eletronic Library Online]. 2016 [cited 3 Apr 2017] ; 69(2): 229-34.
Available from:
http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-71672016000200229&lng=en
.
http://dx.doi.org/10.1590/0034-7167.2016690204i
.
8. Azevedo R. As principais causas de mortes no Brasil (e como evitá-las). Exame. 2015 [cited 2 Apr 2016]. Available from: http://exame.abril.com.br/brasil/as-principais-causas-de-mortes-no-brasil-e-como-evita-las/ .
9. Melo ACL, Menegueti MG, Laus AM. Profile of patient in intensive care: considerations for the nursing team. [Journal of Nursing UFPE on line]. 2014 [cited 5 Apr 2016]; 8(7): 3142-8. Available from: file:///C:/Users/Usuario/Downloads/4912-61710-1-PB.pdf
10. França CDM, Albuquerque PR, Santos ACBC. Perfil epidemiológico da unidade de terapia intensiva de um hospital universitário. InterScientia [Periódicos Unipe]. 2013 [cited 5 Apr 2016]; 1(2): 72-82. Available from: file:///C:/Users/Acer%20M5/Downloads/203-210-1-PB.pdf .
11. Camuci MB, Marins JT, Cardeli AAM, Robazzi MLCC. Epidemiological characterization of adult patients hospitalized in a burns intensive care unit. Cogitare enferm [Internet]. 2014 [cited 28 Mar 2016]; 19(1): 78-83. Available from: http://revistas.ufpr.br/cogitare/article/viewFile/35961/22415 .
12. Passos SSS, Silva JO, Santana VS, Nascimento VM, Pereira A, Santos LM. User embracement in care for families at an intensive care unit. Rev enferm UERJ [http://www.e-publicacoes.uerj.br]. 2015 [cited 30 Apr 2016]; 23(3). Available from: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/6259/18303 .
13. Silva ML, Caminha RT, Oliveira SH, Diniz ER, Oliveira JL, Neves VS. Úlcera por pressão em unidade de terapia intensiva: análise da incidência e lesões instaladas. Rev Rene. [Scielo – Scientific Eletronic Library Online] 2013 [cited 30 Mar 2016]; 5(14): 938-44. Available from: http://www.revistarene.ufc.br/revista/index.php/revista/article/viewFile/1341/pdf_1 .
14. Oliveira EL, Westphal GA, Mastroeni MF. Demographic and clinical characteristics of patients undergoing coronary artery bypass graft surgery and their relation to mortality. Rev Bras Cir Cardiovascular. [Scielo – Scientific Eletronic Library Online]. 2012 [cited 3 Apr 2016]; 27: 52-60. Available from: http://www.scielo.br/pdf/rbccv/v27n1/en_v27n1a09.pdf .
15. Souza A. Número de leitos em internação diminui, mas cresce os de UTI, diz CFM. 2016. [cited 5 Apr 2016]. Available from: http://oglobo.globo.com/brasil/numero-de-leitos-de-internacao-diminui-mas-cresce-os-de-uti-diz-cfm-19320428 .
16. Nogueira LS, Sousa RMC, Padilha KG, Koike KM. Clinical characteristics and severity of the patients admitted to the public and private ICUS. Texto contexto - enferm. [Scielo – Scientific Eletronic Library Online]. 2012 [cited 9 Apr 2016]; 21(1): 59-67. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-07072012000100007&lng=en. http://dx.doi.org/10.1590/S0104-07072012000100007 .
17. Silva ST, Ribeiro RCHM. Principais causas de internação por doenças cardiovasculares dos idosos na UCOR. Arq Cien Saúde [http://repositorio-racs.famerp.br/racs_ol/online.html]. 2012 [cited 2 Apr 2016]; 19(3) 65-70. Available from: http://repositorio-racs.famerp.br/racs_ol/vol-19-3/ID-470-19-jul-set-2012.pdf .
18. Bezerra GKA. Unidade de terapia intensiva – perfil das admissões: Hospital Regional de Guarabira, Paraíba, Brasil. Rev Bras CiSaúde. [http://periodicos.ufpb.br/ojs2/index.php/rbcs]. 2012 [cited 3 Apr 2016]; 16(4): 491-96. Available from: file:///C:/Users/Acer%20M5/Downloads/11900-26943-1-PB%20(1).pdf .
19. Hissa PNG, Hissa MRN, Araújo PSR. Análise comparativa entre dois escores na previsão de mortalidade em unidade terapia intensiva. Rev Bras Clin Med [http://bases.bireme.br]. 2013 [cited 1 Apr 2016]; 11(1): 21-6. Available from: http://files.bvs.br/upload/S/1679-1010/2013/v11n1/a3383.pdf .
20. Santos AM, Souza GRB, Oliveira AML. Sepse em adultos na unidade de terapia intensiva: características clínicas. Arq Med Hosp Fac Cienc Med Santa Casa São Paulo. 2016 [cited 5 Apr 2017]; 61:3-7. Available from: http://www.fcmsantacasasp.edu.br/images/Arquivos_medicos/2016/01-AO90.pdf .
21. Silva MPP, Carvalho NZ, Pires JO, Paula PH, Gomes GLO, Costa CKF, et al. Causas evitáveis de internamento em unidade de terapia intensiva. Iniciação científica cesumar [periódicos.unicesumar.edu.br]. 2013 [cited 6 Apr 2016]; 15(2): 147-55. Available from: http://periodicos.unicesumar.edu.br/index.php/iccesumar/article/viewFile/3189/2287 .
22. Denti IA, Pesavento JA, De Biasi LS, Manfredini CS. Prognóstico da severidade de doenças em pacientes internados em unidade de terapia intensiva. Perspectiva [www.uricer.edu.br]. 2015 [cited 30 Mar 2016]; 39 (145): 29-39. Available from: http://www.uricer.edu.br/site/pdfs/perspectiva/145_479.pdf .
23. Giacomini MG, Lopes MV, Gandolfi JV, Lobo SM. Septic shock: a major
cause of hospital death after intensive care unit discharge. Rev bras ter
intensiva [Scielo – Scientific Eletronic Library Online]. 2015 [cited 9 Apr
2016]; 27(1): 51-6. Available from:
http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103-507X2015000100051&lng=en
.
http://dx.doi.org/10.5935/0103-507X.20150009
.