REVIEW ARTICLES
Educational strategies for people with Hypertension and Diabetes mellitus
Maria Fernanda ManoelI; Sonia Silva MarconII; Vanessa Denardi Antoniassi BaldisseraIII
ISpecialist in Public and Family Health. Regular student of the Master´s degree in Nursing at the State University of Maringá. Nurse of the Reference Center in the of interdisciplinaty monitor to the Chronic hypertensive and Diabetic patient. Londrina, Paraná, Brazil. E-mail: mariafernanda.manoel@gmail.com.
IIDoctor in philosophy of nursing. Faculty of Graduate and postgraduate education in nursing at the State University of Maringá, work co-advisor. Maringá, Paraná, Brazil. E-mail: soniasilva.marcon@gmail.com.
IIIDoctor in Sciences. Associate Professor of the Nursing Department at the State University of Maringá. Work advisor. Maringá, Paraná, Brazil. E-mail: vanessadenardi@hotmail.com.
IVWork done in the subject Advanced Topics: care in the different life cycles of the master's degree in nursing at the State University of Maringá, in 2010.
ABSTRACT: The present study aimed at analyze the educational strategies used with people with arterial hypertension and Diabetes Mellitus conveyed in the literature of database of Scientific Electronic Library Online from 1990-2010. Through the bibliographic research with emphasis in document analysis, were analyzed 20 articles that presented educational activities to this population. The articles were classified according to the research method, the strategy/approach of teaching used and professional category of the authors. In relation to the education focus, it was observed that the emancipatory strategies were more frequent among the published studies. As for the professionals involved in the publications, the nurse is highlighted. It is concluded that the main strategies used in health education for patients with hypertension and Diabetes mellitus have been an emancipatory approach in confrontation with those predominantly normative and vertical businesses.
Keywords: Health education; hypertension; Diabetes Mellitus; nursing.
INTRODUCTION
The transformations produced by society over time significantly altered the profile of the morbidity and mortality of the Brazilian population, contributing to the progressive decrease of deaths from communicable diseases and increase of deaths from chronic non-communicable diseasesIV (NCD), which we can mention the Diabetes Mellitus (DM) and systematic arterial hypertension (SAH)1,2.
The NCD constitute a serious public health problem, both in rich and poor countries2. Currently, the NCD total 63% of all deaths in Brazil and are responsible for 75% of the cases of incapacity3. It is highlighted that SAH is related, in Brazil, with 35% of the total deaths caused by cardiovascular diseases4. As for the prevalence of DM in the world, there are over 346 million individuals, while in Brazil there are about five million people diagnosed with the disease5. The ratio is a person with the disease in every ten adults6. In Brazil, both the prevalence of SAH and the DM has increased in recent decades, in particular when associated with themselves7.
The overall increase in the prevalence of SAH and the DM represents important prejudice to quality of life and incurs high burden on health systems. Educational measures are pointed as important prevention strategies and monitoring aimed at improving the health and quality of life, as well as collaborates with the reduction of the complications and costs arising from assistance of these diseases8. Health education programs are highlighted as positive measures in the control of chronic conditions, including how preventative for complications9.
Health education combines multiple determinants of human behavior with various learning experiences and educational interventions presenting itself as a systematically planned activity. It facilitates, predisposes and reinforces behavioral measures adopted by a person, group or community to achieve an intentional effect on the own health10.
The actions with educational character constitute only a fraction of the technical activities aimed at health, specifically as regards the ability to organize the educational component in programs developed in different environments, in many different levels of performance10. These are, however, actions inherent to the process of care.
The strategies used to carry out health education are very importance, as they may stimulate the active participation of the individual, valuing the dialogue as shared knowledge construction11 or, conversely, may simply reinforce the healing character centered in diseases and in transmitting information.
When these strategies are published in the form of scientific studies can greatly, disseminate knowledge that will be translated into ownership by the practice, guiding the behavior of educational professionals.
Thus, the objective of this research was to analyze the educational strategies used by people with SAH and DM conveyed data base reports in the Scientific Electronic Library Online (SCIELO), during the period from 1990 to 2010.
METHODOLOGY
This is a search of bibliographical nature, exploratory, with emphasis in the proposal of document analysis, in which were analyzed available scientific articles in the Scientific Electronic Library Online (SCIELO) published between 1990 and July 2010, when the search occurred in the articles.
As inclusion criteria we defined that would be valid articles that present educational actions with people with SAH and DM, both of foreign productions, as national productions, since they were free access. As exclusion criteria were established: incomplete articles; articles already included in combination of other descriptors defined for searching for articles, namely: education, teaching, arterial hypertension and Diabetes mellitus combined with each other. The papers found were analyzed and the located in both descriptors were deleted automatically from one of them.
Combining education and Diabetes mellitus descriptors, 22 works were found and selected two that met the inclusion criteria. Using the descriptors arterial hypertension and teaching, were obtained 32 works and selected two that met the criteria. With education and arterial hypertension descriptors were found 43 articles, being selected six that met the criteria and, finally, by means of Education and Diabetes mellitus descriptors were found 50 articles, of which 10 were selected.
In this way, we use the total of 20 articles that complied with the objective of this research and the established inclusion/exclusion criteria.
To organize the analysis, it was used a frame with the authors and the key terms that instrumentalize analysis of the main concepts presented in articles. In the step of processing of the data, it was used the process of coding and inferences about the information contained in the publications, finding the topics covered through the analysis of its contents. The articles were analyzed as to the method of research, the educational strategy used and the authors' professional category.
RESULTS AND DISCUSSION
It was found that among the 20 (100%) articles analyzed, 15 (75%) were published between 2005 and 2010. The data revealed a significant increase of productions about educational strategies, in the first decade of 2000, stepped from the year 2005. This may be related to the increasing prevalence of these diseases in the world's population, as in the Brazilian population12, which allegedly may have boosted health professionals to rethink their educational strategies and, consequently, to extend the knowledge on the theme from the initiative of carrying out research in this area. Thus, this evidence may have collaborated with reflection of health professionals about the need to rethink their pedagogical alternatives, contributing constructively with their practice13.
We can also relate this increase of production with the changes that has taken place in the models of health care, especially as regards people with chronic diseases, whose focus has been the commitment to quality of life of this population, boosting to more effective strategies for approaches that include the integrality of attention with an emphasis on health promotion2 – which health education becomes an essential element.
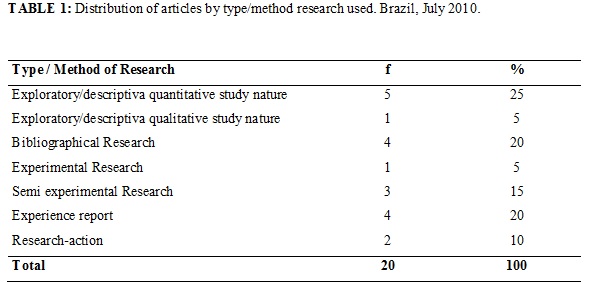
Highlighting the most research methods employed by these studies, it is pointed out firstly the exploratory/descriptive quantitative nature study – 5 (25%), followed also the case studies, the literature research – 4 (20%) and secondly, as shown in Table 1.
Exploratory-descriptive nature studies are often used when it is wanted to describe and/or explain a fact or phenomenon and tends to have a character focused on the disease14, whereas studies carried out by the action-research method or new emancipatory methodologies, are facing the dialogue and awareness of people15.
The emancipatory approach or social critic was instituted in the 60 by educator Paulo Freire. He proposed a new method of teaching that was not just literacy, but also critical awareness and development to the decision-making process. This educational reference caused radical changes in the management and educational practice and did break with the traditional form of education that was based on the transmission of knowledge. On critical-social approach, within educative actions in health, seeks to stimulate the participation of people actively in all stages of the educational process, from planning to evaluation16.
Behaviors that take into account the awareness, blaming people for their own learning, have been increasingly stimulated and used by health professionals. It is worth mentioning the study conducted by the State University of Minas Gerais, which had as its principle the educational practice-based in Freire´s philosophy. This study stimulated the participation of patients with a diagnosis of Diabetes Mellitus to participate in the development of an educational primer, based on questions and opinions of patients and also demonstrated that the participation of target groups in the preparation of educational material makes it more effective as regards the result of the strategy of health education, especially regarding the necessary content to each individual15.
In experimental and semi-experimental research is good to evaluate the practical educative testing results13-17. Therefore, not necessarily these methods allow to enhance the educational process regarding human approach, dialogical and pertinent participatory to emancipatory education, but rather about the goals that have been achieved.
The case studies, in turn, contributes to the dissemination of actions that are being put into practice12 and therefore allows to share innovative knowledge of everyday professional, bringing theory and practice, the knowing and the doing.
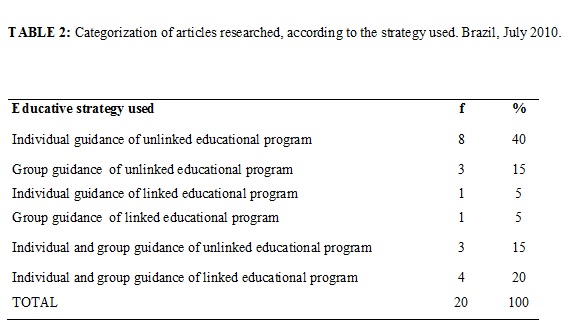
In relation to the types of strategies that have been used for the approach of people with SAH and DM, it was possible to observe the existence of two more significant: the individual guidance and orientation on group, associated with each other or not, and linked to educational programs or not. The one-to-one mentoring and educational program unlinked was prevalent in the texts examined, as shown in table 2.
Looking for arguments that guide to the type of educational strategy more effective in monitoring of people with SAH and DM, were found differences of information.
A study of review of literature on self-care of people with DM type I identified that both the individual and the monitoring group present equivalence in the improvement of metabolic control18. In fact, the frequent contact with the health team has been appointed as the factor that produces sense of confidence, however, needs to be viewed with extreme caution because it may cause the false perception that replaces the non-pharmacological treatment5, implying educational action in this matter.
An experimental research held in patients with DM type II, it was identified that the two strategies have been effective, but people who participated in the education in group showed better results of glycemic control than those who performed only the individual monitoring17.
The studies mentioned indicate that the diagnosis of the disease can collaborate also with the choice of educational method, because the natural evolution of the disease, its symptoms and its demands of coping will be different and will guide the educational pathway. In this connection, a study conducted through the integration of operating groups and individual consultations showed significant reduction of blood pressure and serum glucose level in people with SAH and DM19.
To better discuss the educational focus of the works reviewed, it was opted for organizing articles into two antagonistic and contrasting categories. On one side the normative approach, focusing on the disease; on another side the emancipatory perspective, based on the participative dialogue20. Thus, it was found that 7 (35%) articles used the normative approach and 13 (65%), the emancipatory.
It is possible to observe that the productions on the educational strategies, here analyzed, signaling for changes in the educational approach, once the emancipatory perspective was used by the majority of the studies. Thus, there is an emerging character of overrun of the curative model where healthcare was heavily centered in attendance conduct complaint and pervaded by multiple requirements, something quite common in the normative approach. Therefore, the published works turned mostly to the preemptive model, based on participatory dialogue, on interdisciplinary, in criticism and not alienate health/disease process, consistent with the emancipatory perspective.
The following should be noted, however, that such a result is confronted by other authors where the healing vision still predominates among health professionals and healthcare continues strongly anchored in curative attendance20. It is explained this disagreement because the data of the present study have been originated from research published, while the aforementioned study20 is based on the empirically verified educational actions, signaling to the abyss that still prevails among the theory – the result of scientific research, and the practice-fruit of daily professional.
In the emancipatory perspective, the health education programs have developed differentiated strategies through a diverse and qualified team. This is the case, for example, project Diabetes Weekend who owned team prepared to act with people affected by type 1 DM, through a summer camp held during a weekend. Count on a multidisciplinary team, made up of doctors from different specialties, nutritionist, psychologist and physicist educator and nurse, which used dynamics and collective games, to build knowledge of self-care so enjoyable craving also stimulating the quality of life of these people21.
On the other hand, it was possible to observe programs that count with the participation of a single professional, most of the time the nurse, who was in charge of conduct guidelines14. It is worth that the integrality of attention directed toward people with chronic diseases is one of the principles of the current Brazilian health system2, which the assistance of a single professional, only in educational activities, will be insufficient to ensure impact on complex needs of this population demand. signals, to the urgency of a practice integralized of person centered care, where the contexts are valued, the familiar scenarios, cultural processes, the inter subjectivity and the power relations, given the peculiarities of the subjects involved22, for which the team work contributes significantly.
The problems involving the educative actions becomes more evident when in practice assumed the passivity of the population and if it adopts archaic educational posture of transmitting information about the disease, about the proper diet and about the necessary treatment, unlinked from reality, possibilities of learning, emotional, social and economic conditions of each customer, remaining doubts if indeed, learning happened.
Also the design of each professional on education and health must be considered, because it influences the choice of teaching strategies and interferes directly in the results. In this way, the health educator, in search of a contextualized educational practice, must be attentive to the concerns, the issues of emergency subject who live with the disease, respecting their beliefs, their feelings and their culture in order to direct educational activities effective and individualized16.
The articles published were analyzed, according to the Professional category of the authors. It was found that most of the articles have authorship of nurses, either in isolation or associated with other professionals, according to table 3.
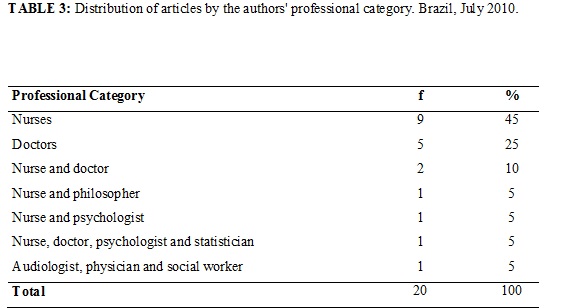
These data corroborate other work20 and translate the involvement of nurses with the subject in question. The fact of the nursing practice a large role in the context of HAS and DM, through actions ranging from participation in early detection programs until the development of strategies to ensure adherence to treatment, has led to further efforts to the publication of studies, focusing on the education and guidance of the person as an integral part of nursing care23.
It is likely that the formation of this professional has contributed to their insertion in educational actions together with engaged people with SAH and DM. Also their participation in activities of this nature occurred for their insertion in serving this population in health monitoring programs20. Thus, the very practice of nursing in primary health care, which includes the completion of the home visit, as an instrument for the care, covers health education in its dynamics24. In addition, the educational action needs to be conceived as a pedagogical dimension of the practice of nursing.
We cannot forget, however, that education and health are interface themes of interdisciplinary is present15. For this reason, there are other professional inclusion in educational practice by clarifying that, from the perspective of health promotion, there is need for multidisciplinary and interdisciplinary.
Accordingly, it is appropriate that education and health issues continue to be the target of research also by other professionals, enabling new configurations of the educational strategies.
FINALS CONSIDERATIONS
It was noted, in this research, that the strategies of health education for people with SAH and DM have been increasing focus on investigations, disclosure of emancipatory experiences in confrontation with those whose focus has been predominantly normative and vertical. It was possible to observe the use of one or more educational activities, individual and group approach, individual guidance and unlinked educational paradigm shift in articles analyzed.
Health education is indispensable for people affected by chronic diseases, with a view to self-care, change of habits and improving the quality of life. The participatory approach and criticism was applied by the majority of the studies reviewed, having been successful in the results.
It is worth remembering that, the method of teaching used directly interferes in the effectiveness of learning; Therefore, the approach used should focus on the problems experienced by clients, promoting their autonomy, in appropriate educational material, in the pleasant place and on time for the educational action, enabling the reflection of those involved about their experiences, living conditions, health and disease. In addition, the persons intended to educational action should be involved in planning, action, learning needs assessment and in the organization of the material, so that the process of learning to be contextualized, participatory and Dialogic.
It is highlighted the authorship of nurses in most of the analyzed publications, highlighting that it is engaged in the production of Professional category knowledge and educational practice geared towards people with SAH and DM. In fact, nursing, in its praxis, values the educational activity in health, but it is necessary to enlarge the multidisciplinary and interdisciplinary teamwork.
REFERENCES
1. Paiva DC, Berssusa AAS, Escuder MM. Avaliação da assistência ao paciente com diabetes e/ou hipertensão pelo Programa Saúde da Família do Município de Francisco Morato, São Paulo, Brasil. Cad Saude Pública. 2006; 22:377-85.
2. Ministério da Saúde (Br). Diretrizes e recomendações para o cuidado integral de doenças crônicas não transmissíveis. Série Pactos Pela Saúde. Brasília (DF): Editora MS; 2008: 1-72.
3. Moura EC, Mauta DC, de Morais Neto OL, Monteiro CA. Prevalence and social distribution of risk factors for chronic noncommunicable diseases in Brazil. Pan Am J Public Health. 2009; 26:17-22.
4.Cavalari E,Nogueira MS, Fava SMCL, Cesarino CB,Martin JFV. Adesão ao tratamento: estudo entre portadores de hipertensão arterial em seguimento ambulatorial. Rev enferm UERJ. 2012; 20:67-72.
5. Miyar-Otero L, Arrelias CCA, Lima YCI, Pena FPS, Santos MA, Teixeira CRS et al. Seguimento de pacientes com Diabetes mellitus em serviço de atenção básica: parâmetros clínicos e laboratoriais. Rev enferm UERJ. 2010; 18:423-8.
6. American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes care. 2012; 35 (supl.):11-63.
7. Freitas LRS, Garcia LP. Evolução da prevalência do diabetes e deste associado à hipertensão arterial no Brasil: análise da Pesquisa Nacional por Amostra de Domicílios, 1998, 2003 e 2008. Epidemiol Serv Saúde [periódico na Internet]. 2012; [citado em 09 mar 2013]. 21(1): 07-19. Available at: http://scielo.iec.pa.gov.br/scielo.php?script=sci_arttext&pid=S1679-49742012000100002&lng=es.
8. Pereira FRL, Torres HC, Candido NA, Alexandre LR. Promovendo o autocuidado da educação em diabetes na educação individual e em grupo. Cienc cuid saude. 2009; 8: 594-9.
9. Frigo LF, Silva RM, Mattos KM, Boeira GS, Manfio F, Piaia E et al. Ação educativa interdisciplinar para pacientes com diabetes na atenção básica: uma revisão bibliográfica. Rev Epidemiol Control Infect. 2012; 2(4):141-3.
10. Candeias NMF. Conceitos de educação e promoção em saúde: mudanças individuais e mudanças organizacionais. Rev Saude Publica. 1997; 31: 209-13.
11. Acioli S, David HMSL, Faria MGA. Educação em saúde e a enfermagem em saúde coletiva: reflexões sobre a prática. Rev enferm UERJ. 2012; 20:533-6.
12. Rodrigues ACS, Vieira GLC, Torres HC. A proposta da educação permanente em saúde na atualização da equipe de saúde em diabetes mellitus. Rev esc enferm USP. 2009; 44: 531-7.
13. Zanoni PH, Parisi MCR, Admoni AN, Queiroz MS, Nery M. Curso de imersão em diabetes como técnica educativa para profissionais médicos. Arq Bras Endocrinol Metab. 2009; 53: 355-9.
14. Manzini FC, Simonetti JP. Nursing consultation applied to hypertensive clients: aplocation of Orem’s self-care theory. Rev Latino-Am Enfermagem. 2009; 17: 113-9.
15. Torres HC, Candido NA, Alexandre LR,Pereira FRL. O processo de elaboração de cartilhas para orientação do autocuidado no programa educativo em diabetes. Rev Bras Enferm. 2009; 62: 312-6.
16. Tavares DMS, Rodrigues, RAP. Educação conscientizadora do idoso diabético: uma proposta de intervenção do enfermeiro. Rev esc enferm USP. 2002; 36:88-96.
17. Torres HC, Franco LJ, Stradioto MA, Hortale VA, Schall VT. Avaliação estratégica de educação em grupo e individual no programa educativo em diabetes. Rev Saude Publica. 2009; 43: 291-8.
18. Leite SAO, Zanim ML, Granzoto PCD, Heupa S, Lamounier, RN. Pontos Básicos de um programa de educação ao paciente com Diabetes mellitus tipo 1. Arq Bras Endocrinol Metab. 2008; 52: 233-42
19. Silva RT, Feldemam C, Lima MHA, Nobre MRC, Domingues RZL. Controle do diabetes mellitus e hipertensão arterial com grupos de intervenção educacional e terapêutico em seguimento ambulatorial de uma Unidade Básica de Saúde. Saude soc. 2006; 45: 180-9.
20. Toledo MM, Rodrigues SC, Chiesa AM. Educação em saúde no enfrentamento da hipertensão arterial: uma nova ótica para um velho problema. Texto contexto enferm. 2007; 16:233-8.
21. Maia FFR, Araújo LR. Projeto “Diabetes Weekend”- proposta de educação em diabetes mellitus tipo I. Arq Bras Endocrinol Metab. 2002; 46:566-73.
22. Mandú ENT. Intersubjetividade na qualificação do cuidado em saúde. Rev Latino-Am Enfermagem. 2004; 12: 665-75.
23. Chaves ES, Lucio IML, Araujo TL, Damsceno MMC. Eficácia de programas de educação para adultos portadores de Hipertensão Arterial. Rev Bras Enferm. 2006; 59:543-7.24. Kebian LVA, Acioli S. Visita domiciliar: espaço de práticas de cuidado do enfermeiro e do agente comunitário de saúde. Rev enferm UERJ. 2011; 19:403-9.