PCS- Primary Care Services – FHU/ TCP- Outpatient Reference for TB/SE- Specialized Services. (*) Excluding statistically irrelevant response categories (n<5).
RESEARCH ARTICLES
Individual determinants and utilization of health services for tuberculosis diagnostic
Débora Raquel Soares Guedes TrigueiroI; Jordana de Almeida NogueiraII; Aline Aparecida MonroeIII; Lenilde Duarte de Sá IV; Ulisses Umbelino dos AnjosV; Tereza Cristina Scatena VillaVI
I
Nurse, Ph.D. candidate at the Graduate Nursing Program. Health Sciences Center (Centro de Ciências da Saúde). Federal University of Paraiba (Universidade
Federal da Paraíba), João Pessoa, Paraíba, Brazil. E-mail: deborasgt@hotmail.com
II
Ph.D. Professor at the Clinic Nursing Department. Graduate Nursing Program. Health Sciences Center (Centro de Ciências da Saúde). Federal University of
Paraiba (Universidade Federal da Paraíba), João Pessoa, Paraíba, Brazil. E-mail: jalnogueira31@gmail.com
III
Ph.D. Professor at the Mother-Child Nursing and Public Health Department. Nursing School at Ribeirão Preto. University of São Paulo (Universidade de São
Paulo). Ribeirão Preto, São Paulo, Brazil. E-mail: alinemonroe@yahoo.com.br
IV
Ph.D. Professor at the Nursing and Public Health and Psychiatry Department. Graduate Nursing Program. Health Sciences Center (Centro de Ciências da Saúde).
Federal University of Paraiba (Universidade Federal da Paraíba), João Pessoa, Paraíba, Brazil. E-mail: sa.lenilde@gmail.com
V
Ph.D. Professor at the Statistics Department. Graduate Program in Decision-Making Models in Health. Center for Exact Sciences. Federal University of
Paraiba (Universidade Federal da Paraíba), João Pessoa, Paraíba, Brazil. E-mail: ulissesanjos@gmail.com
VI
Full Professor at the Mother-Child Nursing and Public Health Department. Nursing School at Ribeirão Preto. University of São Paulo (Universidade de São
Paulo). Ribeirão Preto, São Paulo, Brazil. Coordinator of Operational Research for the Brazilian Tuberculosis Research Network. E-mail: tite@eerp.usp.br
VII
This research is part of the Multi-Center Project entitled Delay in Tuberculosis Diagnosis: Analysis of Causes in Different Regions in Brazil
approved and sponsored by the National Council for Scientific and Technological Development (CNPq).
ABSTRACT
It is a cross-sectional study which aimed to analyze the influence of the individual determinants in the utilization of health services for the access to tuberculosis diagnostic. 101 patients in treatment in João Pessoa-PB were interviewed, from July to October 2009.Three indicators were raised – predisposition, availability and necessity. These indicators were evaluated by means of bivariate analysis and association chi-square test. It was found that 46.5% of patients accessed the Primary Care Services (PCS), 36.6% opted by Specialized Services and 16.8% looked for the ambulatory of the Tuberculosis Control Program. In both sexes, the demand for PCS was predominant, as well as between individuals until 40 years old and above 60, brown and black people, and with low levels of income and education. The individual determinant associated to the demand for the PCS units is related to the attributes of people from the lower socioeconomic classes, reflecting in the inequalities of health access.
Keywords: Tuberculosis; diagnosis; utilization; individuality.
INTRODUCTION
The outline sketched by the sanitary reform in Brazil has brought about organizational technical-assistance changes upon the health scene, which have directly affected the use of health services. Under strong incentive by the Department of Health, the Family Health Strategy (FHS) emerges as priority for enhancing Primary Care Services (PCS), a gateway to the local health services system. Those services were found to be priority in the FHS to get to know the individuals within its operational limits; to identify health problems and risk situations found in the community; to formulate an agenda for actions to cope with determinants of the health-disease process; to plan on and to carry out inter sector awareness and training actions related to the health problems listed within its operational limits; and to provide total care to families under its responsibility1.
In face of the wide range of possibilities to assure the entire population better access to health, country-wide expansion of FHS was expected, reaching in June, 2010, 95% of the Brazilian municipalities, with more than 32 thousand teams, and 55% of the population under coverage. Still in the past years, the strategy pace has shown a global increase of 3% per year, expanding into large cities and state capitals in the country2.
As opposed to FHS rapid growth in small towns, implementation of FHS in large urban centers has been slow, on account of high demographic concentration, high exclusion levels in health services, aggravating factors profile in metropolis, inarticulate and poorly distributed care network, in a complex array of other interrelated factors 3.
In spite of the impasses, PCS unities are expected either to become the gateway to receive users in a condition compatible with tuberculosis (TB) or to identify breathing symptoms frames in the community, showing decision capability to identify the disease in time as well as to provide necessary actions. It must be highlighted that the user's background on that level, in face of the decision capability acknowledged, interferes with the standards of use of the remaining health care spots.
Along with that, regardless of being acknowledged as priority, an ideal option for healthcare, the utilization of PCS cannot be taken for granted. The client's willful search for a specific type of service involving a series of determinants is part and parcel of the process of healthcare utilization. Thus, the research aimed at analyzing the effects of individual determinants upon standards of healthcare utilization as gateway to TB diagnosis in João Pessoa, PB, Brazil.
THEORETICAL FRAMEWORK
Utilization of healthcare results from the interaction of a series of factors. In addition to the availability of services, reasons why people seek health care derive from interaction of socioeconomic and psychological factors, as well as morbidity profiles. However, effects and relative relevance of each factor are conditioned by cultural background, health policies in force, and characteristics of health system4.
From that standpoint, it may be highlighted that both internal and external factors to health services can be characterized as conditioning factors to utilization. Consumption of healthcare is related both to the way offer is structured and to individuals' characteristics and behaviors in face of the disease, as to their attitude seeking assistance, obtaining access, and profiting from the care received. Additionally, subjects' preferences and options prove decisive concerning standards of service utilization, since "not all needs become demands and not all demands are met" 5:689.
Among the wide range of considerations which must be taken into account for better understanding of that phenomenon, this research has set up as a guiding priority the identification of influences of individual determinants upon the standard of service utilization in TB diagnosis care. The starting assumption is that the search for healthcare (potential access) is determined by predisposition, availability, and need6. The predisposition component includes the characteristics that correspond to the individuals being prone to seek health service. They precede emergence of disease, are intrinsically subject-related, and include factors such as sex, race/color, religion/belief, and schooling, among others6.
The availability component is related to means or tools people have to utilize health services. These resources can be individual or family-specific, as income and social security, in addition to those community-specific qualities related to where the individual lives (urban region/rural region)6.
Need accounts for the determinant the closest to utilization of health services. It refers to the level of acknowledgement of health problems or of unsatisfactory health condition, comprising the most immediate reason for seeking care (spontaneous demands). The health need can be acknowledged within the individual sphere (behavior seeking) or can be prompted by the identification of problems not acknowledged as such by the individuals themselves (induced demand/ active search within the community)6,7 .
METHODOLOGY
Epidemiological, sectional research, on the basis of quantitative approach. João Pessoa, the state capital of Paraíba, Brazil, was elected the scenery for this investigation for integrating the group of 11 (eleven) priority municipalities of the federative unity showing healing and discontinuation rates not in keeping with the goals set up in the National Program of Tuberculosis Control.
The municipality of João Pessoa has 723,5158 inhabitants and organizes health care on a regional basis, with five Sanitary Districts with 180 family health units (USF), showing coverage rate at 84%. TB cases find two gateways in the municipality: USF and the specialized outpatient unit of the Hospital Complex Clementino Fraga (Complexo Hospitalar Clementino Fraga – CHCF), regarded as a state reference for diagnosis and treatment of the disease.
The research sphere included users undergoing treatment and residing in the municipality, excluding patients under 18 years of age and the jail population. Sample size estimated was calculated through Statistic program (with the Several means, ANOVA, 1-Way commands) and considered the following parameters: probability of type I error = 0.05; probability of type II error = 0.20; variation due to error = 0.2. One hundred informants were deemed necessary on the basis of that estimate. Selection of cases was made on a convenience basis, on account of the need to investigate all patients undergoing treatment.
Data were collected from July to October 2009 based on primary sources – interviews with patients. The questionnaire used was adapted and validated 10, and included evaluation indicators of TB control-related actions within primary care services. To meet research purposes, 13 variables concerning individual determinants to access were elected, as follows: Indicator 1 – Predisposition: sex, age, race/color, marital status, belief or religion, schooling; Indicator 2 – Availability: occupation, monthly income, and number of people depending on the income; Indicator 3 – Need: frequency he/she was exposed to awareness initiatives/campaigns/training before becoming ill, a family member with TB treatment background, evaluation of TB acknowledgement before becoming ill, symptom severity.
Data were entered and stored on a 2003 Excel spreadsheet and forwarded to the incoming data table of the 11.0 Statsoft Statistic Software. Variables studied were categorized or dichotomized according to their specificities, and were compared with the different health services: PCS; Tuberculosis Control Program (TCP) and specialized services (SE). PCS included the Family Health Units (FHU); Tuberculosis Control Program (TCP) – specialized outpatient reference for TB – and SE included general and privately-held hospitals, policlinics, and privately-held medical offices. Indicators raised were submitted to statistical treatment by means of bivariate analysis and the chi-square test of association ((c2).
In compliance with the guidelines provided for in the research protocol of the Resolution 196/96 of the National Health Council, this project was forwarded to the Committee for Ethics in Research of the Federal University of Paraiba (Universidade Federal da Paraíba - UFPB). It was approved on December 17, 2008, under protocol number 0589. The confidential character of the information on the questionnaires was ensured, and written consent was obtained from all interviewees.
RESULTS AND DISCUSSION
Indicator 1 - Predisposition
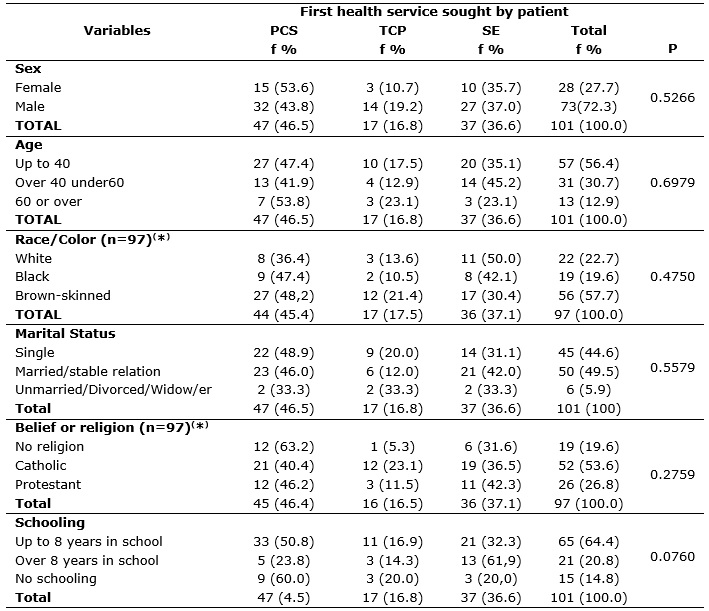
Among the total cases diagnosed (N=101), 47(46.5%) accessed PCS upon identifying signs and symptoms of the disease; 37(36.6%) opted for SE, and 17(16.8%) sought the TCP. Social demographic analysis showed 73 (72.3%) cases affecting males and 28 (27.3%) affecting females. Average age was 41.2 years (dp=14.92), 65 (64.4%) with 8 (eight) years of schooling, 50 (49.5%) were married or had a stable relation, 52 (53.6%) were Catholic, and 56 (57.7%) were brown-skinned, according to Table 1.
TABLE 1:
Association between variables related to the predisposition indicator, and the first health service sought by the tuberculosis (TB) patient. João Pessoa,
Paraíba, Brazil, 2009 (N=101).
PCS- Primary Care Services – FHU/ TCP- Outpatient Reference for TB/SE- Specialized Services. (*) Excluding statistically irrelevant response
categories (n<5).
The demand for PCS prevailed in both sexes, as well as among individuals up to 40 years of age (47.4%) and over 60 (53.8%), brown-skinned and black, with no schooling or with over 8 years of schooling. Individuals over 40 and under 60 (53.8%) sought SE more frequently, as well as white individuals with over 8 years of schooling , as shown on Table 1.
Thus, as with the remaining variables, marital status and belief/religion played no role on the differences found across the election of health services, with PCS reaching the highest rates. On the use of the test of association, at the 5% (α = 0.05) level of significance, proportion resemblance was evinced, but not the association between the variables which characterize the social demographic profile (sex, age, race, marital status, belief, schooling) and the type of service sought.
Indicador 2 - Availability
The following analysis resulted from the association between the variables that comprehend the availability indicator and the first health service sought by the patient upon showing signs and symptoms of the disease. Among the cases investigated, PCS were preferably accessed by the patients on unemployment (39.4%), retirement (58.8%), and by the economically vulnerable (52.9%), according to Table 2.
TABLE 2:
Association between variables related to the availability indicator, and the first health service sought by the tuberculosis (TB) patient. João Pessoa,
Paraíba, Brazil, 2009 (N=101).
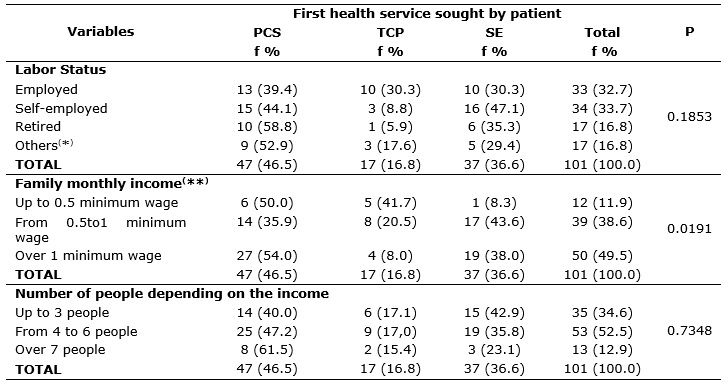
PCS- Primary Care Services – FHU/ TCP- Outpatient Reference for TB/SE- Specialized Services. (*) "Others" category corresponds to students,
those on a leave, or dollar (**) Minimum wages R$ 465.00.
Among the patients under the employed/self-employed category, 16 (47.1%) sought SE, which comprehend primarily chargeable assistance on personal visits to the doctor or at privately-held hospitals. Average family income of TB patients was R$ 465.00 (four hundred sixty-five reais). Fifty-one (50.5%) declared making a living with an amount inferior to one minimum wage unit, with an average of 4.4 people depending on that income. Patients with the lowest incomes and the largest families elected PCS as their first option.
The chi-square test of association showed that among the variables related to the availability indicator, only the monthly family income variable was statistically expressive (p=0. 0191).
Indicator 3 - Need
Upon conclusion of analyses, association was identified between the variables comprehending the need indicator and the first health service sought by patients upon showing signs and symptoms of disease. Results show that SE were preferably elected among patients with no access to awareness initiatives/campaigns/training. Conversely, PCS came at the top of the election list among patients showing previous awareness of the disease.
Still from the standpoint of TB awareness, living with a family member affected by the disease presupposes awareness of transmission. Among patients declaring previous contact with family members affected by the same disease, 47.2% sought PCS, 33.3% resorted to SE, and just 19.4% sought the TCP. Among those declaring having no family members with a TB treatment background, utilization of services showed similar figures: 46.7% for PCS, 40.0% for SE, and 13.3% for the TCP, as shown on Table 3. Such findings enhance the unsatisfactory result of patient's evaluation on TB awareness before infection of disease. It stands out, therefore, that almost the totality of subjects identifies as poor or average their general awareness of TB, and in both cases, PCS proved to be the gateway with the highest demand.
Highlighting the above, it becomes visible that in view of lack of notion about the problem as well as about its manifestation, it is the aggravating symptoms that determine healthcare demand. Among the cases analyzed, (N=101), 73 (72.7%) sought healthcare just when they could identify strong symptoms of the disease. However, it must be enhanced that regardless of symptom severity, PCS showed highest demand. The use of the test of association, at the 5% (α = 0.05) significance level, evinced proportion resemblance, as well as non-existence of association between variables related to the need indicator and the type of service sought.
TABLE 3:
Association between variables related to the need indicator, and the first health service sought by the tuberculosis (TB) patient. João Pessoa, Paraíba,
Brazil, 2009 (N=101).
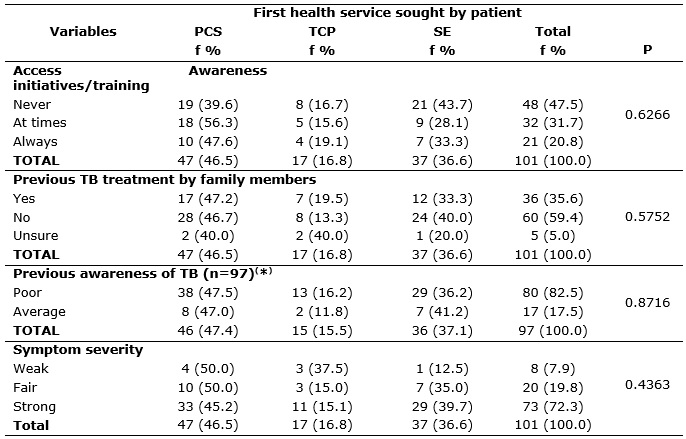
PCS Primary Care Services – FHU/ TCP- Outpatient Reference for TB/SE- Specialized Services. (*)Excluding statistically irrelevant response
categories (n<5).
Among the health services analyzed, it was found that PCS units had a leading position among users with TB. However, that percentage is not higher than 50% of the total number of TB patients investigated, a figure signaling to the services insufficiency as gateway. Such findings enhance research conducted country-wide in Brazil, on access to TB diagnosis and treatment. In Campina Grande, PB, Brazil, 51% of users do not seek the USF for disease diagnosis 11. In Ribeirão Preto, SP, Brazil, 34.5% of users with TB were received at emergency or hospital care, with PCS at an inexpressive 9.8% rate at identification of cases12.
As for access, research results publicized in Tamil Nadu, Southern India, show women with TB are more likely to use PCS than men. They have available time to access those services in their regular hours and are prone (have the opportunity) to visit the units on behalf of their children's health (childcare, inoculation or even prenatal care)13.
Brazilian studies show that women's presence at PCS is more outstanding than that of men.5,14. Men's behavior on that scene has been accounted for on two grounds: socialization (time spent at work, hanging out with friends, evening pleasures, etc) and the care process as alien to male practice. 15,16.
Despite those differences reported in the research presented, this research found no association between the female sex and PCS as the leading service sought, demand rates being proportional in both sexes.
On nationwide research to set up utilization standard of healthcare according to social demographic profile, age is regarded as a variable affecting behavior for medical assistance demand. It was found that among those not receiving healthcare by the SUS (Single Health System), rates of adults were proportionately higher than those of children and of the elderly17.
An additional study to identify profile changes in healthcare utilization, conducted in the São Paulo region, registered expressive difference on age distribution (p= 0.03), with higher rates of elderly users in the area the FHS was implemented than in the area not serviced by the strategy18.
In spite of the fact that most elderly people (53.8%) seek PCS, when it came to TB, there was no association between age group and the service sought, as gateway, according to results in this research.
In the health profile, race/color is an important social variable, for it allows for thinking racial disparities striking black and brown-skinned people, with skin color determining their status or social exclusion. However, few Brazilian studies incorporate existing disparities on the basis of skin color to health indicators. Moreover, the very health professionals neglect this determinant in the office interviews with patients. 19,20.
The research showed that 50% of white patients started their journey in the health system at the specialized services, which are predominantly constituted of chargeable assistance with unmediated disbursement. Nevertheless, no association between race/color and type of service sought was identified in this research, especially because poverty, as a condition, brings them all together.
As for marital status and religion, factors related to TB, lack of literature interweaving the several variables to health problems is outstanding. However, it must be enhanced that culturally shaped segregation and false beliefs about the TB patient must have a ban. Changes in the patients' social lives, which bring about additional effects upon their intimate relations, must be avoided. Attention to diagnosis and support to patients and their central social network must be reinforced, in view of the fact that most respondents in this research (49.5%) are married or have a stable relation.
The highest concentration of individuals with low schooling levels, identified in the results, rounds off the patients' social demographic profile. An additional concerning facet of the country's health scene comes out, that which is found in the literature that associates higher risks of TB infection to social strata with lowest schooling levels21-23. Data from the 2003 National Household Sample Survey – PNDA, show that among the SUS's (Single Health System) users, those with lower schooling levels, low income, and disclosure from private health plans prevail24. Existing logics rules that people with low schooling levels are usually economically disfavored on the social scene and use free-of-charge public services. This finding can be identified among those in this research, showing that higher rates of demand for PCS are presented by patients with no schooling or with up to 8 years of schooling, whereas patients with schooling levels over 8 years get into the health system through SE.
As for economic profile, writers signal that population facing the most adverse social economic conditions are more likely to be users of the SUS (Single Health System), system, whereas those users of the privately held health system belong in the higher strata of social demographic pyramid, with higher per capita family income. Writers add that the most serious difficulty to access is concentrated on the poorest contingent in the country, where, at the same time, individuals with higher social economic standards are more likely to use health services24. Other scholars confirm that understanding upon investigating variation in outpatient service used according to income, as follows: "higher income groups use chargeable services in privately-held doctors' offices and clinics, whereas those with lower income resort to state-run outpatient services and health centers 25:142.
Although the SUS (Single Health System) system has been instituted to target the whole of the population, regardless of economic status found in each social stratum, in reality, the wide social disparities help increase expectations about public policies that they should preferably provide assistance to the population strata with no additional health insurance or assistance from privately-run services24.
From this perspective, expectations were met in this research, that is, results show that most patients with lowest monthly incomes (equal or under one minimum wage) would be likely to seek public health services (PCS and TCP) and unlikely to seek SE), predominantly paid-upon-assistance services. Among variables related to the availability indicator, monthly family income was the only one showing statistically expressive association, with a type of health service demanded by TB patients (p= 0.0191). However, patients with monthly income between half and one minimum wage reached the expressive percentage of 43.6% in face of the demand for SE.
Although this research has found no association between the variables of users' awareness profile in face of service demanded, it stands out that 82.5% of patients investigated evaluated as poor their awareness of the disease. The demand for health care was found to be motivated by aggravating signs and symptoms of disease in 72.3% of cases.
CONCLUSION
This research has brought out into the investigation scene the relation between individual determinants for access and utilization of health services as gateway for patients infected with TB on a three-folded front, namely, predisposition, availability, and need.
It was found that both female and male patients made larger use of PCS as gateway to the healthcare network, as well as young adults, the elderly, as well as black and brown-skinned individuals. Prevailing demand for PCS also occurred among the single and the married or among those with a stable relation, in all religious segments, and among users with low schooling levels and lower income.
Self-evaluation by patients of their own awareness about the disease ranged unsatisfactorily, from average to poor, with symptom severity, in general, prompting the individual to seek care. Granting that ways of living and thinking play an important role on acknowledging the disease and coping with it, and that different actions for disease control must be elaborated on the basis of specific subjects and their scenes, health teams are expected to include in their daily actions those routines and processes of systematic search for health needs, in addition to the development of skills to identify the adequacy between supply and the specific context subject/teams meets.
Conclusions show, therefore that the theoretical models utilized confirmed the presence of predisposing factors favoring disparities in demand and supply in healthcare. Nevertheless, interpretation of variables selected neglects variability and dynamics of concrete social meanings. One of the limitations of the association studies proves to be the breaking down of the whole into inter-associated parts by linear cause-effect relations. Thus, they deal with a conditional positivity inherent to a discourse that becomes detached from variability, complexity, and dynamics of meanings in social practice in which such possibilities of falling ill are experienced. However, endeavoring to value subjective dimensions can generate expressive advances in the formulation of strategies to overcome TB. It allows for the understanding the whole of subjects through their specific behavior on demand for healthcare, as well as for the valuing of their stand and awareness to enable their visibility and co-responsibility in the process.
REFERENCES
1.Escorel SE, Giovanella L, Mendonça MHM, Senna MCM. O programa saúde da família e a construção de um novo modelo para atenção básica no Brasil. Rev Panam Salud Publica. 2007; 21: 164-76.
2.Ministério da Saúde (Br). Garantindo o acesso a toda população: saúde em todo o lugar. Departamento de Atenção Básica SAS. Brasília (DF): Ministério da Saúde. [citado em 09 jun 2011] Disponível em: http://portal.saude.gov.br/portal/arquivos/pdf/apres_13m_heider.pdf.
3.Sousa MF, Fernandes A, Araújo C, Fernandes MC. Gestão da atenção básica: redefinindo contextos e possibilidades. Divulgação em Saúde para Debate. 2000; 21:7-14.
4.Mendoza-Sassi R, Béria JU, Barros AJD. Outpatient health service utilization and associated factors: a population-based study. Rev Saúde Pública. 2003; 37:372-8.
5.Pinheiro RS, Viacava F, Travassos C, Brito AS. Gênero, morbidade, acesso e utilização de serviços de saúde no Brasil. Ciênc saúde coletiva. 2002; 7:687-707.
6.Aday LA, Andersen R. A framework for the study of access to medical care. Health Services Research. 1974; 208-20.
7.Branch L. Assessment of chronic care need and use. The Gerontologist. 2000; 40:390-6.
8.Instituto Brasileiro de Geografia e Estatística. Cidades [site de internet] [citado em 12 set 2012].
Disponível em: http://www.ibge.gov.br/cidadesat/topwindow.htm?1.
9.Hair JrJF, Anderson RE, Tatham RL, Black WC. Análise multivariada de dados. Porto Alegre (RS): Bookman; 2005.
10.Villa TCS, Ruffino Netto A. Questionário para avaliação de desempenho de serviços de atenção básica no controle da TB no Brasil. J Bras Pneumol. 2009; 35:610-2.
11.Figueiredo TMRM, Villa TCS, Scatena LM, Gonzales RIC, Ruffino-Netto A, Nogueira JA, et al. Desempenho da atenção básica no controle da tuberculose. Rev Saude Publica. 2009; 43: 825-31, 2009.
12. Arcêncio RA, Arakawa T, Oliveira MF de, Cardozo-Gonzales RI, Scatena LM, Ruffino Netto A, Villa TCS. Barreiras econômicas na acessibilidade ao tratamento da tuberculose em Ribeirão Preto - São Paulo. Rev esc enferm USP. 2011; 45:1121-7.
13.Balasubramanian R, Garg R, Santha T, Gopi PG, Subramani R, Chandrasekaran V, et al. Gender disparities in tuberculosis: report from a rural DOTS programme in south India. Gender disparities in tuberculosis: report from a rural DOTS programme in south India. Int J Tuberc Lung Dis. 2004; 8:323-32.
14.Figueiredo W. Assistência à saúde dos homens: um desafio para os serviços de atenção primária. Ciênc saúde coletiva. 2005; 10:105-9.
15.Courtenay WH. Constructions of masculinity and their influence on men's well-being: a theory of gender and health. Soc Sci Med. 2000; 50:1385-401.
16.Fonseca J LCL, Leão LS, Lima DC, Targino P, Crisóstomo A, Santos B. Homens e cuidado: uma outra família? In: Acosta AR, Vitale MA, organizadores. Família: redes, laços e políticas públicas. São Paulo: Pontifícia Universidade Católica de São Paulo; 2003. p. 79-91.
17.Ribeiro MCSA, Barata RB, Almeida MF, Silva ZP. Perfil sociodemográfico e padrão de utilização de serviços de saúde para usuários e não usuários do SUS – PNAD 2003. Ciênc saúde coletiva. 2006; 11:1011-22.
18.Goldbaum M, Gianini RJ, Novaes HMD, César CLG. Utilização de serviços de saúde em áreas cobertas pelo programa saúde da família (Qualis) no Município de São Paulo. Rev Saúde Pública. 2005; 39:90-9.
19.Batista LE. Mulheres e homens negros: saúde, doença e morte [tese de doutorado]. Araraquara (SP): Universidade Estadual Paulista; 2002.
20. Araújo CLF, Cruz LMF, Lopes MC, Fernandes ECS. O quesito cor/raça em formulários de saúde: a visão dos profissionais de saúde. Rev enferm UERJ. 2010; 18:241-6.
21.Bowkalowski C, Bertolozzi MR. Vulnerabilidades em pacientes com tuberculose no distrito sanitário de Santa Felicidade – Curitiba, PR. Cogitare Enferm. 2010; 15:92-9.
22.Vendramini SHF, Gazetta CEI, Chiaravalotti FN. Tuberculose em município de porte médio do sudeste do Brasil: indicadores de morbidade e mortalidade, de 1985 a 2003. J Bras Pneumol. 2005; 31: 237-43.
23.Ximenes RAA, Albuquerque MFPM, Souza WV, Montarroyos UR, Diniz GTN, Luna CF, et al. Is it better to be rich in a poor area or poor in a rich area? A multilevel analysis of a case–control study of social determinants of tuberculosis. Int J Epidemiol. 2009; 38:1285-96.
24.Ribeiro MCSA, Barata RB, Almeida MF, Silva ZP. Perfil sociodemográfico e padrão de utilização de serviços de saúde para usuários e não usuários do SUS – PNAD 2003. Ciênc saúde coletiva. 2006; 11:1011-22.
25.Travassos C, Viacava F, Fernandes C, Almeida CM. Desigualdades geográficas e sociais na utilização de serviços de saúde no Brasil. Ciênc saúde coletiva. 2000; 5:133-49.