RESEARCH ARTICLES
The quality of life of clients with tuberculosis in the context of primary
Sheila Nascimento Pereira de FariasI; Célia Regina da Silva MedeirosII; Maria Yvone Chaves MauroIII; Liane Gack GhelmanIV; Elaine Franco dos Santos AraujoV
IPhD. in Nursing. Faculty member. Universidade Federal do Rio de Janeiro, Anna Nery School of Nursing, Public Health Nursing Department. Rio de Janeiro,
RJ, Brazil. E-mail: sheilaguadagnini@yahoo.com.br
IIM.Sc. in Nursing. RN. Universidade Federal do Rio de Janeiro, Hospital Universitário Clementino Fraga Filho, Centro Cirúrgico. Rio de
Janeiro, RJ, Brazil. E-mail: celiamedeiros@globo.com
IIIPhD. in Nursing. Faculty member. Universidade Federal do Rio de Janeiro, Anna Nery School of Nursing, Public Health Nursing Department. Rio
de Janeiro, RJ, Brazil. E-mail: mycmauro@uol.com.br
IVPhD. in Nursing. Faculty member. Universidade Federal do Rio de Janeiro, Anna Nery School of Nursing, Public Health Nursing Department. Rio
de Janeiro, RJ, Brazil. E-mail: lgghelman@gmail.com
VPhD. in Collective Health. Faculty member. Universidade Federal do Rio de Janeiro, Anna Nery School of Nursing, Public Health Nursing Department. Rio de
Janeiro, RJ, Brazil. E-mail: elainefsaraujo@uol.com.br
ABSTRACT
This study aimed to investigate the quality of life of clients with tuberculosis (TB) treated at a Basic Health Unit (BHU) and discuss the relationship between TB and quality of life of clients. This is a study with a quantitative approach. The study setting was a primary care unit of the Municipal Health Secretariat of Rio de Janeiro. Was used in the survey, the WHOQOL-Bref World Health Organization. Participants were 102 clients with tuberculosis. Instrument data were processed using the software SPSS for Windows, version 17. Results: Clients reported a good quality of life, which is attributed to treatment adherence in SUS, receiving medication and counseling, with rapid clinical improvement. It was concluded that customers TB does not bring a negative view of their quality of life.
Keywords: Tuberculosis; quality of life; basic care; nursing.
INTRODUCTION
Tuberculosis (TB) is an important public health problem in Brazil, due to the expressive number of cases affecting the population each year. In Brazil, in 2008, 68,147 new tuberculosis were registered (incidence coefficient of 35.59 per 100,000 inhabitants), 56,172 of which were bacilliferous pulmonary forms (incidence coefficient of 29.33 per 100,000 inhabitants) and 9,712 extrapulmonary (incidence coefficient of 5.07 per 100,000 inhabitants). The largest absolute number of cases in Brazil is detected in the state of Amazonas, followed by the state of Rio de Janeiro. When considering the number of deaths due to tuberculosis, however, the latter presents a higher mortality rate. In addition, the relevant nature of the study is the bacillus' multiresistance to treatment1.
The search for quality of life has gained increasing importance, especially among health workers. The relation between quality of life and health goes beyond each individual's material conditions, as the human being's existential needs should be respected.
Interest in measuring the health-related quality of life has grown with the change in the morbidity and mortality profile, including a higher prevalence of chronic-degenerative conditions, a drop in mortality rates due to some diseases and, finally, an increased life expectancy. This means believing that living is not merely surviving, but living with quality.
Nowadays, it is considered relevant to get to know clients, in this case tuberculosis patients' quality of life, with a view to contributing to the prevention of illnesses, underlining the need for them to gain healthy life habits. As a profession that aims for education, nursing can greatly contribute in this area.
Quality of life emerged as an important health concept. Researchers, physicians, nurses, psychologists perceive quality of life as an important dimension of a population or individual's health. Nursing care is holistic and provides support focused on the human response and on the health condition. Quality of life and its measurement are important foci in the assessment of this response. Investing in quality of life means creating a mechanism for health promotion and disease prevention, particularly tuberculosis.
Thus, this study was aimed at: investigating the quality of life of clients with tuberculosis, followed during nursing consultations at a primary health care unit (PHCU), and discussing the relation between tuberculosis and these clients' quality of life.
LITERATURE REVIEW
The quality of life concept has been widely used recently and has even become part of common sense. As observed, the media disseminates the concept indiscriminately, favoring a generic or reductionist viewpoint, without any proper subjective deepening. This dimension, which is almost always ignored or receives limited attention, has aroused scientific interest and increasing awareness, receiving due consideration as part of an integrated and interdisciplinary approach, aiming for holistic solutions that are focused on the comprehensive wellbeing of human beings.
Quality of life tends to be assessed in research and its routine application is a fundamental instrument used in clinical practice. Quality of life assessment has improved communication between clients and health professionals, having the clients emphasize those domains that are more important to them during the evaluation process. Health-related quality of life can also be of help in decisions related to chronic conditions, distinguish factors that affect the preferred treatment, facilitate information, turning patients into direct participants in therapeutic decisions, and provide relevant data to the regulatory health authorities for the approval of new drugs, techniques and devices2.
In the health context, the quality of life concept is focused on health promotion. Health-related quality of life assesses individual difficulties to live with some condition and the influence of treatment or interventions in that decision. Health professionals can directly influence the health-related quality of life, assessing the disease, interfering in morbidities (relieving pain, ailments) and evaluating the interventions3-6.
In 1994, the World Health Organization Quality of Life Group (WHOQOL) defined quality of life (QoL) as "individuals' perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns"4:25. This definition implicitly states that the QoL concept is subjective, multidimensional and that it includes both positive and negative evaluation elements.
The general health status is assessed based on individuals' perception of their present health, comparing it with that of other people and with their own future health5.
In this context, one needs to understand that the quality of life of tuberculosis patients is a complex combination of disease, poverty, stigma, discrimination and lack of treatment with family life, work and social activities. Also, the disease affects not only the infected person, but also his/her family, community and country6.
To understand the essence of health care, not only the indicators of change in the frequency and problems related to tuberculosis, but also the indicators of wellbeing should be included. This disease affects the person's general health condition, causing a substantial but as of yet hardly characterized impact, which can reflect disease symptoms, treatment side effects and social concerns, such as isolation and job loss7.
A better understanding of TB patients' experiences can help to improve the therapeutic schemes, treatment adherence and people's wellbeing, promoting the success of the therapeutic process. A lack of awareness or knowledge about the disease can lead TB patients to mistaken attitudes, which can influence the information and, consequently, the adherence to an appropriate therapeutic scheme. Health education is fundamental to eliminate a negative attitude towards the disease8.
METHOD
The study was undertaken at a Primary Health Care Unit affiliated with the Rio de Janeiro Municipal Health Secretariat in Planning Area 2.2. The service's opening hours are from 7 to 17 h. It does not offer emergency care and has its own clinical analysis laboratory for laboratory tests like sputum smears and cultures.
The data were collected using an instrument developed by the World Health Organization Quality Of Life Group (WHOQOL-bref). The WHOQOL-bref questionnaire has been tested and validated in different cultures, under the coordination of the WHO group. Used to assess the quality of life of adult populations, the WHOQOL-Bref consists of 26 questions, 24 of which are distributed in four domains: physical, psychological, social relationships and environment9.
Participants were 102 clients who complied with the following inclusion criteria: tuberculosis patients enrolled in the Polyclinic's Tuberculosis Program, seen during the morning and/or afternoon shift and suffering from pulmonary, extrapulmonary or pulmonary/extrapulmonary tuberculosis; who had started treatment (with medication), independently of the treatment stage, and who signed the consent term before participating. The data were collected between February/2010 and April/2010, through the individual distribution of the WHOQOL-Bref questionnaire for completion. The researchers clarified any doubts.
The quantitative data were processed using descriptive statistics. The answers were grouped and ranked to develop a database, using the software Statistical Package for the Social Sciences (SPSS) version 17 for Windows, recommended by WHO.
The quality of life scores were analyzed in accordance with the WHO domains: physical, environmental, psychological and social relationships. The scores were calculated according to the syntax made available by WHO.
To collect the data, the project was submitted to the research ethics committees of the Municipal Health Secretariat and Anna Nery School of Nursing/Universidade Federal do Rio de Janeiro (EEAN/UFRJ), and received authorization under protocols 077/09 and 214/09.
The clients from the health service who complied with the inclusion criteria were consulted and those who agreed to participated signed two copies of the Free and Informed Consent Form, which stated: the research theme, the study objectives, guaranteed secrecy, freedom to refuse to participate or withdraw consent in any research phase, among others, as well as the free expression of ideas, opinions and assertions on the theme. The study did not entail any cost for the participants.
The collected data were organized and presented in two tables and one graph (figure) to comply with the proposed study objectives.
RESULTS AND DISCUSSION
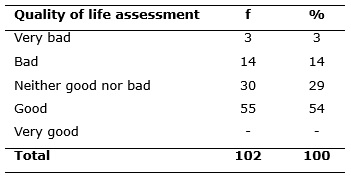
Out of the 102 questionnaires applied to the clients, 100% were completed and returned. The clients with tuberculosis assessed their quality of life as shown in Table 1.
TABLE 1:
Distribution of variables related to quality of life assessment of clients with tuberculosis. Primary Health Care Unit, Municipal Health Secretariat - RJ,
2010.
The large majority of the tuberculosis patients, 54%, considered their quality of life as good, while 29% assessed it as neither good nor bad and 3% as very bad.
The notion quality of life figures in a polysemic semantic field: on the one hand, it is related to the way of life, conditions and styles; on the other, it includes the ideas of sustainable development and human ecology. And, finally, it is related to the field of democracy, development and human and social rights. Concerning health, these notions combine in the collective constructed social result of standards of comfort and tolerance a certain society establishes for itself3.
The perceived quality of life varies among individuals and is dynamic. Individuals with different expectation, with a similar clinical condition, report on a diverse quality of life. Quality of life is an eminently human concept that has been related to the degree of satisfaction found in family, love, social and environmental life and in the existential esthetics itself. It presupposes the ability to develop a cultural synthesis of all elements a certain society considers as its standard of comfort and wellbeing4.
The clients' assessment of the quality of life domains is displayed in Table 2.
TABLE 2:
Assessment of quality of life domains by clients with tuberculosis. Primary Health Care Unit, Municipal Health Secretariat - RJ, 2010.
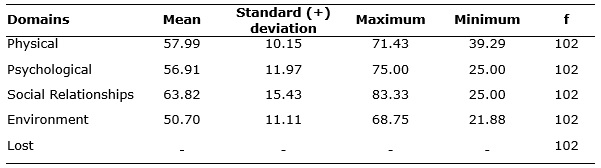
As observed, all 102 (100%) participants properly completed the questions related to the domains: physical, psychological, social relationships and environment. The mean scores in the different domains were similar, demonstrating homogeneity among these aspects in the analyzed individuals' life. The highest mean score in the domains was found in the social score, with 63.82 ±15.43. This was followed by the psychological and physical domains, with similar results of 56.91 ± 11.97 and 57.99 ±10.15, respectively. The environmental domain reached 50.70 ± 11.11. The highest maximum score was reached in the social domain, with 83.33. On the other hand, the lowest maximum score was found in the physical domain (71.43), while the environmental construct reached the lowest minimum score (21.88). Nevertheless, no significant differences were found among the means, with similar scores.
The large majority indicated a good quality of life, which means that, although they suffered from TB, for most clients, their quality of life was good, keeping in mind that quality of life is associated with different factors, including health, and that clients often do not consider simply being healthy as a synonym of quality of life. The term quality of life does not have a sole meaning. Health conditions, social functioning and quality of life have been used as synonyms.
As can be inferred, the quality of life theme is treated from a wide range of perspectives, whether in science, through different disciplines, or in common sense, whether from an objective or subjective viewpoint, whether through individual or collective approaches. In general, studies discuss situations related to individuals' daily quality of life after the experience of diseases, ailments or medical interventions. The role of health professionals is both to promote wellbeing and prevent illnesses, so that it is coherent for them to act in fields related to these principles.
Based on the data collected in the scale that assessed the social relationships domain, it is inferred that the clients could count on social support in accordance with their needs. Considering the facets of each domain, it was verified that the social domain is directly linked to social relationships, social support and sexual activity.
When analyzing the scores, it is verified that the tuberculosis patients presented a good quality of life. The lower score in the physical domain is justified by the fact that the population is ill, which can entail some physical limitations, and by the effects of the medication administered throughout the treatment.
Quality of life is a dynamic concept, which changes in the course of people's lives. Satisfaction with life and the feeling of wellbeing can often be a momentary feeling. The conquest of a high-quality life, however, is constructed and consolidated in a process that includes reflections on how quality of life is defined for oneself and the setting of targets, inspired by the desire to be happy. Quality of life is a broad, subjective and polysemic concept that has motivated different health studies, particularly focused on ill people. These illnesses, despite the technological advances that have extended patients' lives, have not always produced a qualitative impact. In chronic pulmonary diseases, multiple factors are interrelated and can influence people's perceived health and quality of life10.
Despite divergences as to its concept, a consensus exists that quality of life involves levels of physical, mental and social functioning and role performance, and also includes satisfaction with life skills, perceptions and social wellbeing and is directly related to age, gender and the trauma severity11.
A consensus exists that optimistic people face their problems better, are less stressed and, thus, get ill less. When they feel incapable of taking care of themselves, people's self-esteem and self-confidence is affected. Learning to cope with the disease by changing one's habits is an essential factor for one's autonomy12.
In view of the difficulties professionals face to broaden the health concept, which goes beyond the absence of diseases and strengthens the quality of life, one starting point may be the overcoming of the traditional care model for people with chronic conditions, which has been developed through the routine that ranges from the diagnosis, confirmed through tests, to the definition of a basic treatment and monitoring for evaluation, as well as any adjustments needed13-19. This crystallized model is being reverted through the valuation of the subjects' subjectivity and of the importance of people's self-assessment of their health and life, which is frequently better than that of the professional. This fact is explained by the adjustment to the new situation and the development of new attitudes and the adaptation of their lifestyle to the limitations deriving from the disease13.
Nowadays, as a result of effective treatment, society no longer sees tuberculosis patients as a collective danger, although prejudice is still found. Patients are already able to understand that, when they catch tuberculosis, they are not condemned to a social death, even though the disease sometimes causes limitations in their professional and family life; in most cases, these derive from their own physical condition when they are strongly affected by the disease. As a result of modern chemotherapy, this situation is temporary and does not necessarily need to influence the individual and the collective 14-19.
Being healthy means being able to act, despite the presence of pathological situations, being able to cope with challenges by overcoming adverse conditions. Thus, the notion of being healthy is associated with different aspects of life15.
Tuberculosis requires programs aimed at the improvement of quality of life. Its control is a great challenge that imposes the solution of problems with a view to compliance with therapeutic schemes. In addition, monitoring the problems these patients face can enhance treatment adherence, increasing the number of successful therapeutic cases. Therefore, in their analysis, health managers need to include not only indicators of changes in the disease's frequency and ailments, but also indicators of wellbeing, as that is the only way to understand the essence of the health care delivered7,16-19.
Nevertheless, although TB is curable, a significant impact on the patients' quality of life remains. Although the clients indicated a good quality of life, it should be acknowledged that TB changes people's lives, mainly regarding the treatment and medication, which is also the case when people are affected by a wide range of diseases.
It should be highlighted that the patients' lives do not need to be transformed from a personal and social perspective because of the disease, as this can be avoided through appropriate treatment.
CONCLUSION
As a disease that still entails prejudice, clients could have a negative view of their quality of life, which was not identified.
As observed in the theory, quality of life is a comprehensive and subjective concept, involving several aspects of life, including the health dimension. When one discusses the relation between quality of life and TB, the individual's universe is revealed. The majority took into account different aspects, the way of life, the daily reality of treatment and others, defining their quality of life as good. This is also due to treatment adherence and to the rapid improvement in the symptoms.
It is expected that this study will contribute not only to TB control, but also that it will arouse researchers and health professionals inquiries about care delivery to health service users in general.
REFERENCES
1.Ministério da Saúde (Br). Manual Técnico para o controle da tuberculose: cadernos de atenção básica. Brasília (DF): Ministério da Saúde; 2010.
2.Luderitz B, Werner J. Quality of life in patients with atrial fibrillation. Arch Intern Med. 2000; 160: 1749-57.
3.Minayo, MCS, Hartz ZMA, Buss PM. Qualidade de vida: um debate necessário. Ciênc Saúde Coletiva. 2000; 5: 17-8.
4.Fleck MPA. A avaliação de qualidade de vida: guia para profissionais de saúde. Porto Alegre (RS): Artmed; 2008: 25.
5.Frazão CMFQ, Ramos VP, Lira ALBC. Qualidade de vida em pacientes submetidos a hemodiálise. Rev enferm UERJ. 2011; 19: 577-82
6.Phaladze NA, Human S, Dlamini SB, Hulela EB, Hadebe IM, Sukati NA et al. Quality of life and the concept of living well with HIV/AIDS in sub-Saharan Africa. J Nurs Scholar. 2005; 37: 120-6.
7.Dhuria M, Sharma N, Ingle GK. Impact of tuberculosis on the quality of life. Indian J. Community Med. 2008; 33: 58-9.
8.Eram U, Khan IA, Tamanna Z, Khan Z, Khaliq N, Abidi AJ. Patient perception of illness and initial reaction. Indian J Community Med. 2006; 31: 198.
9. Fleck MPA, Louzada S, Xavier M ET AL. Aplicação da versão em português do instrumento abreviado de avaliação de qualidade de vida WHOQOL-BREF. Rev Saude Publica. 2000; 34: 178-83.
10.Dourado VZ. Influência de características gerais na qualidade de vida de pacientes com doença pulmonar obstrutiva crônica. J Bras Pneumol. 2004; 30: 207-14.
11.Hu XB, Feng Z, Fan YC, Xiong ZY, Huang QW. Health-related quality-of-life after traumatic brain injury: A 2-year follow-up study in Wuhan, China. Brain Inj. 2012; 26:183-7.
12.Panzini RG, Rocha NS, Bandeira DR, Fleck MPA. Qualidade de vida e espiritualidade. Rev Psiq Clin. 2007; 34: 105-15.
13.Ramos N, Crepalde ATA. Qualidade de vida em doenças pulmonares crônicas: aspectos conceituais e metodológicos. J Bras Pneumol. 2000; 26: 207-13.
14.Rodrigues ILA, Souza MJ. Representações sociais de clientes sobre a tuberculose: desvendar para melhor cuidar. Esc Anna Nery. 2005; 9: 90-7.
15.Paiva L, Rossi LA, Costa MCS, Dantas RAS. Qualidade de vida na perspectiva de vítimas de
traumas múltiplos e seus familiares. Rev enferm UERJ. 2012; 20: 507-12.
16.Alves RS, KM J Souza, Oliveira AAV, Palha PF, Nogueira JA, Sá LD. Abandono do tratamento da tuberculose e integralidade da atenção na estratégia saúde da família. Texto contexto - enferm. 2012; 21: 650-7.
17.Alcântara CCS; Kritski AL; Ferreira VG; Façanha MC; Pontes RS; Mota RS; Leitão TMJS. Fatores associados à tuberculose pulmonar em pacientes que procuraram serviços de saúde de referência para tuberculose. J. bras. pneumol. 2012; 38: 622-9.
18.Oliveira-Campos M; Rodrigues-Neto JF; Silveira MF; Neves DMR; Vilhena JM; Oliveira JF; Magalhães JC; Drumond D. Impacto dos fatores de risco para doenças crônicas não transmissíveis na qualidade de vida. Ciênc & Saúde Coletiva. 2013; 18: 873-82.
19.Barrêto AJR; Sá LD; Nogueira JA; Palha PF; Pinheiro PGOD; Farias NMP; Rodrigues DCS; Villa TCS. Organização dos serviços de saúde e a gestão do cuidado à tuberculose. Ciênc & Saúde Coletiva. 2012; 17: 1875-84.