RESEARCH ARTICLES
Representations about the vulnerability of black and non-black women to the infection of HIV/AIDS
Dera Carina BastosI; Mirian Santos PaivaII; Evanilda Souza de Santana CarvalhoIII;
Gilmara Ribeiro Santos RodriguesIV
INurse, Master in Nursing. Professor of the Nursing Course at Faculdade Dom Pedro II. Salvador, Bahia, Brazil. E-mail: dera.bastos@hotmail.com.
IINurse, PhD in Nursing. Professor of the Nursing Course, Head of the Sexuality, Vulnerabilities and Genders Research Grup. Department of Community Health. Nursing School at Universidade Federal da Bahia. Salvador, Bahia, Brazil. E-mail: paivamirian@hotmail.com.
IIINurse, PhD in Nursing. Professor of the Nursing Course, Department of Health. Researcher at the Center for Interdisciplinary Studies on Health Inequalities at Universidade Estadual de Feira de Santana. Feira de Santana, Bahia, Brazil. E-mail: evasscarvalho@yahoo.com.br.
VNurse, PhD in Nursing. Member of the Sexuality, Vulnerabilities and Genders Research Grup. Research associate at the School of Nursing. Universidade Federal da Bahia. Salvador, Bahia, Brazil. Email: jubaenfa@hotmail.com.
ABSTRACT: The growth of Human Immunodeficiency Virus/Acquired Immunological Deficiency Syndrome (HIV/AIDS) is expressive among women and in heterosexual. This descriptive, quantitative and qualitative study aims to apprehend and analyze the Social Representations about the vulnerability of black and non-black women to the infection of HIV/AIDS. Interviews were performed with 124 women in an the ambulatory of Salvador-Bahia, from August to December, 2007. The data were collected through the test of free association of words, and submitted to the factorial analysis of correspondence in the Tri deux mots. The unmarried women perceive themselves to be vulnerable to HIV and AIDS by using the condom, while married women or in partnership sets consider preventing something necessary for all people, except for themselves, since they represent the AIDS as the disease of the other.
Keywords: Health vulnerability; sexually transmitted diseases; women's health; nursing
INTRODUCTION
At the beginning of the epidemic of acquired immunodeficiency syndrome (AIDS), health policies focused on specific populations of homosexuals and drug users, groups considered at risk for infection with Human Immunodeficiency Virus (HIV)1.
In the 90s, a large number of monogamous women, with stable relationships, judged far away from social norms and therefore sexually and socially within the expected standards, they were infected with the HIV virus, which contradicted the estimates of epidemiologists indicating just how vulnerable women sex workers and injecting drug users are1,2.
The belief in the trustworthiness of the other, the myth of romantic love and the lack of power in negotiating condom use to keep women at a disadvantage, considering that the use of it depends on the acceptance of the other. With this, the feminization of the epidemic has brought the debate on gender, power, sexuality and vulnerability of women married or in stable relashionships3.
The different patterns of vulnerability between men and women in social, cultural and religious reveal the importance of knowing the social representations shared by groups about HIV and AIDS, as these base and influence the behaviors adopted for prevention. Thus, this study was developed in order to grasp and analyze the social representations about the vulnerability of black and non-black women to HIV / AIDS.
LITERATURE REVIEW
In the early years of the epidemic, the prevailing notion was that of individual risk, which was replaced by the concept of risk groups and risk behaviors1. The use of these expressions marked the social and historical construction of AIDS, implying discrimination, stigma, prejudice and social exclusion of infected individuals. However, AIDS has spread to other segments of the population hitherto considered invulnerable. The concept of risk groups has been replaced by the vulnerability, which recognizes the influence of multiple factors, not just the individual in the spread of HIV1-4.
According to this paradigm, women are vulnerable to HIV because of biological susceptibility and reduced sexual autonomy, reinforced by the power and privilege of men. It is assumed that men are more likely to bring HIV to the partner and women wish to avoid HIV, but do not have the power to do so5.
The existing representations over AIDS are the result of the first information broadcasted presenting a serious, rapidly evolving, unknown and lethal illness to society, whose victims were male homosexuals. AIDS was seen as something new, threatening and distant than ever would be part of the daily lives of people who did not belong to this list, mainly because it is linked to what is socially considered as disqualified or immoral. Such roles are rejected by individuals themselves and believed to be on someone else6.
What people know and understand about AIDS comes from everyday conversations, advice, situations lived in their belonging groups and in contact with the media. These unspecialized forms of knowledge characterize a common sense and that knowledge about AIDS base behaviors adopted for its prevention7.
THEORETICAL-METHODOLOGICAL REFERENCES
This is a quantitative and descriptive study based on the theory of Social Representations. Social representations (SR) are produced daily in groups as a way to explain the reality, with the function of elaborating and justifying the behavior, and also to enable communication between individuals8.
After approval by the Ethics Committee of the Department of Health of Bahia by Opinion No. 141/2007, data were collected at the outpatient clinic of a public university in the city of Salvador, Bahia, between August and December 2007. Participated in the research 124 black and non black women randomly selected, seeking gynecological and family planning.
We applied the test of free association of words (TALP), which is a projective technique that consists of providing a verbal or visual stimuli to subjects and request them to speak, on a certain issue, a number of words or phrases that comes to memory by submitting themselves to such stimuli9.
Individually, in a private environment, women were asked to name five words to each of the six stimuli: 1 (AIDS), 2 (Sex) 3 (Sexuality), 4 (AIDS and black women), 5 (AIDS and non black women) and 6 (AIDS and yourself). We used as fixed (sociodemographic) variables: age, race, education and marital status. The data were processed using the software Tri-Deux-Mots version 2.2 Cibois 1995 and interpreted by correspondence factor analysis (CFA). The analysis in the program results in a map composed by two factorial axes F1 and F2, which show the words with the most significant set of approaches and modalities of opposition, to the time that offers a reading of semantic variations in the spatial organization of the field10.
RESULTS AND DISCUSSION
Of a total of 124 women participating in this study, 56 (45%) were in the range of 14 to 24 years, 44 (35.5%) reported being married or have a stable relationship, 75 (60%) were single and only 5 (4%) were divorced . Of the total, 109 (88%) declared themselves black and only 15 (12%) said they were not black. Regarding education, 43 (34.7%), 45 (36.2%) and 36 (29%) reported having attended elementary school, high school and college, respectively.
The AFC taken as a reference frequency was equal to or greater than eight, for invocations of a single inductive stimulus through the opposition game. The color variable was not significant on the total percentage of responses, possibly because the population was made up of, in most cases, 109 (88%) of people who considered themselves to be black, of which 50 (40%) had brown skin and 59 (48%) were black.
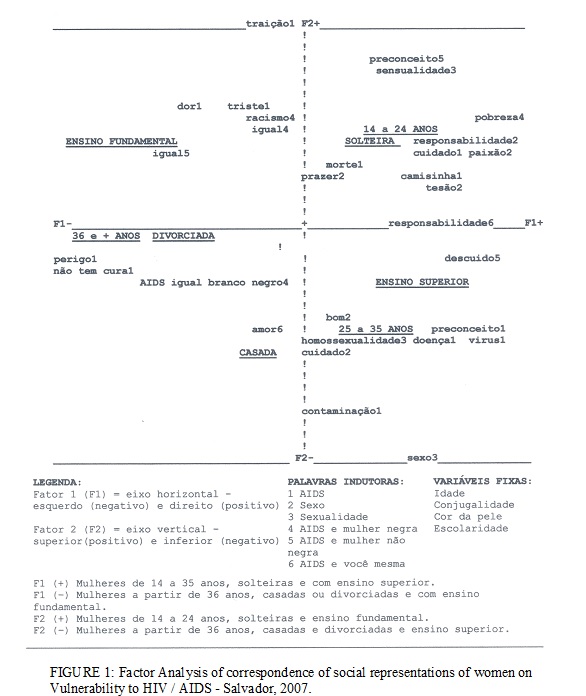
2243 words were raised, of which 909 were different. Factor 1 (F1), horizontal line, explained 33.4% of variance value to which it was added the percentages of 25% Factor 2 (F2), the vertical line in Figure 1, reaching 58.4% of the total variance of the responses, which denotes that both factors have significant explanatory power, and are statistical parameters that have internal consistency and reliability10.
The analysis was conducted from the reading of the mentioned words or distributed representations in the opposite way on the two axes or factors, followed by a number corresponding to the applied stimulus, seen in Figure 1.
On the right axis F1 (+), women 14-35 years of age, unmarried and having higher education, represent a stimulus 1 (AIDS) by the words condom and care. For these, AIDS is anchored in death, and we need to protect ourselves by using condoms, as shown in Figure 1.
Still in F1 (+) for sex (stimulus 2), these same women highlighted their representations by the words passion and lust, which denotes feelings of sexual attraction, romantic view differing from this in other studies of social representations about this subject11. For them, sex should still be done with responsibility, demonstrating that they are more alert to the perception of the risk of contamination.
Another study shows that women with casual sexual profile, most common among the young and not married, are showing greater adherence to prevention. In turn, women with a monogamist profile are the least protected against possible dangers of transmission of sexually transmitted infections (STIs)12.
In axis F1 (+), for women aged from 14-35 years old (unmarried) and having higher education, there was no significance for sexuality (stimulus 3), indicating the difficulty that older women have to expose their representations. These participants represented AIDS and black women (stimulus 4) by the word poverty. For them, the social condition of black women influences to a greater vulnerability to AIDS.
It is recognized that the illiteracy rate among black women is twice the number of that found among whites, and that low education increases women's vulnerability by interfering in economic conditions, the ability to grasp the messages, making the understanding of the disease. Thus, misinformation is a factor of distorted ideas about HIV transmission11.
Studies show that poor women tend to join a series of monogamous relationships to ensure their survival and their children’s, hoping to garantee financial support from the partner. Throughout life, these women may have children with different partners. Because they are concerned with survival issues, they have limited access to services and health information, and options to reduce the risks are not priorities for them13.
However, the same women mentioned above, in axis F1 (+), in relation to AIDS and non-black woman (stimulus 5) expressed the word carelessness. This word is the lack of care and highlights the infection as a result of the negligence of women with regard to preventive measures such as condom use.
Women aged from 14-35 years of age, unmarried, and having higher education, in factor 1 (+), when answering about AIDS and themselves (stimulus 6), evoked the word responsibility, claiming the same power and autonomy to take care of themselves and prevent HIV infection.
Nevertheless, the vulnerability to which women are subject does not depend exclusively on their will, but is enhanced by the asymmetry in the power of decision in affective-sexual relations, arising from gender issues, along with other inequalities such as poverty or discrimination ethnic grounds, creating the so called cumulative vulnerability14.
In F1 (-) on the left of Figure 1, there are 36 years old or older women (married or divorced), with elementary education. These women, in analogy to AIDS (1 stimulus) evoked the words pain, danger, there is no cure and sadness, representing AIDS as a disease which promotes dangerous and incurable pain and sadness. These women, whether they are married or divorced, did not discuss words with significance for sex (2 stimuli) and sexuality (3 stimuli), which can configure a zone of representations, which occurs when a representation has intense emotional change and therefore people avoid talking about it.
Even for the women presented previously, the vulnerability of black women and non-black women was represented as an equal. For them, all individuals, regardless of color, are susceptible to the HIV virus, revealing the ignorance on the part of women with less education about the social and economic aspects that distinguish the vulnerability of black and non black women.
On the vertical axis F2 (+), the top of Figure 1, single women aged 14-24 years with schooling have evoked the words betrayal, pain, sadness, death to AIDS (stimulus 1).
By evoking the word betrayal, young women attribute their vulnerability to AIDS to the behavior of their partner. The vulnerability of women is attributed to feelings of trust in the relationship, the partner and love. These are considered to be inversely proportional to the perception of vulnerability, because the sense of security can lead women to unsafe practices and consequently the possibility of contamination and illness3.
Death is considered one of the hegemonic representations of AIDS, despite advances with the introduction of antiretroviral therapy (ART), which has reduced the morbidity and mortality from opportunistic diseases, providing the HIV carrier a better quality of life. It is still in the popular imagination a stigma as a historical product of emotional representations of illness, but that still circulate in the scientific environment, the media and thought popular imagination3,5.6, and associating virus contamination to a death sentence.
Sex (stimulus 2), was represented as pleasure, approaching the personal satisfaction and away from the representations linked to reproduction, which once seemed only a right of man. Sexuality (stimulus 3) in this age group was represented by the word sensuality, which is linked to the social meanings attributed to women as objects of sexual stimulation, able to provoke the senses and desires.
Still in factor 2 (+), when referring to AIDS and black women (stimulus 4) participants evoke the words equality and racism. For them, both black and non black women are not equally vulnerable to the disease, but it stressed the prejudice of the disease as it is more evident in black women when evoked racism. When this same group is instigated by AIDS and non-black woman (stimulus 5) the word prejudice is evoked.
Prejudice comes to AIDS since the epidemic began, and constitutes the most serious problem faced by people living with AIDS. The disease has been a pretext for discrimination in various contexts. At work, people resign themselves to submit to treatment, others are fired due to prejudice or give up looking for a job because the admission tests exclude people who have the virus14. In the context of health, which discrimination is also evident, the nurse can act discouraging attitudes of prejudice against women with HIV/AIDS3.
There was no representation of single women aged 14-24 years and with school to express themselves and AIDS (stimulus 6). The lack of approximation contents of participants with the syndrome may be influenced by the idea of AIDS as a disease to be just on someone else.
At the bottom of Figure 1 (F2 -), women above 25 years of age and with higher education, married or divorced, representing AIDS through the words disease, viruses, bias and contamination. These anchor AIDS as a disease transmitted by a virus, and surrounded by prejudice. This group brings knowledge elements closer to medicine and leads us to infer that it is women who are approaching information of scientific knowledge.
Regarding sex (stimulus 2), women evoked the words good and care, showing that despite being a pleasurable experience, it must be surrounded by care and preventive practices.
Regarding sexuality (stimulus 3), the representation of these women was evoked by the word homosexuality, which denotes a lack of understanding about sexuality in its broadest sense and positions AIDS as a disease of homosexuals. This group of women did not invoke meaningful words for AIDS and black women (4 stimuli) and AIDS and non-black women (5 stimuli).
Women aged over 25 years old, when referring to themselves and AIDS (stimulus 6), evoked the word love, revealing a romantic view on the relationship. This becomes risky, because the concept of romantic love in the exercise of sexuality implies to be physically and emotionally available to the partner, often leading to resignation, suffering and inequality, which makes prevention measures more difficult, as it motivates women to underestimate the vulnerability sexually transmitted infections can be15,16.
Due to the asymmetry of power, discussing AIDS within relationships can translate into new conflicts in intimacy. This is because the negotiation for condom use, in the sense of disposing of prevention measures, is linked to the imaginary as proof of love, in which the fact of not surrendering to the other opposes trust15-17. There may be still the dread of approaching the issue in the relationship, because the requirement of condoms by women can be understood by the partner as a sign of infidelity, mistrust and or control, or of insubordination and may result in situations of violence or disruption of the relationship16-19.
These representations come from the group of married women in which it has become apparent the increase in vulnerability to HIV infection. The fact of experiencing stable relationships limits the reflection on the perception of risk. Beginning from the courtship, it increases the confidence in the partner, causing unsafe sexual practices to become frequent due to the emotional involvement of the couple3,16-18.
The confidence in the partner, being married or in a stable relationship, a situation that obscures the risk of contamination of women, do not feel at risk for not considering promiscuous and having a unique partner, in this case, the husband, which gives feeling of security19,20.
Married men who do extramarital sex make married women vulnerable to AIDS and other STIs, often leading to late diagnosis. It is worth noting that over 70% of transmissions worldwide are currently among heterosexuals, but the programs and policies, in large part, do not include the prevention needs of men who have sex with women5. Surveys show that heterosexual men do not usually make use of condoms to relate to women, or themselves at risk before knowing to have AIDS20.
The vulnerability of women in stable marital relationships to AIDS highlights the asymmetrical relations of gender that due to cultural, social, political and religious, in a coercive approach, increasingly exposes this woman of the syndrome. To achieve an effective change, this vulnerability therefore needs to be widely discussed not only in health programs but also in education3. Studies highlight that health professionals, particularly the nursing staff, can contribute to the empowerment of women as a strategy for reducing gender inequalities through educational activities capable of providing information about the factors that increase their vulnerability3,11.
CONCLUSION
This study allowed us to grasp and analyze the social representations about the vulnerability of black and non-black women to HIV / AIDS. Women without a regular partner feel more vulnerable to AIDS, using a condom in their casual relationships. On the other hand, married or having a steady partner, consider the AIDS prevention need something to everyone except for themselves, who feel secure in their marital relations, because of a feeling of love and trust in their partner.
We emphasize the need to explore the affective dimensions of the representations of AIDS among women who are in stable relationships, considering that the notions of love, surrender and trust remain as the foundation of an unprotected sexual act, contributing to the feminization of AIDS.
It is noteworthy that participants, regardless of their marital status, when asked to think about AIDS and themselves did not discuss significant content, which may be because of the feeling of invulnerability. This aspect deserves further investigations to further analyze the factors that lead and this distance, since most are self-declared black and represented the black woman as vulnerable.
Representations analyzed here may support actions during nursing care for women, in order to allow reflection on the situations that expose women to such vulnerable conditions, either within or outside of stable relationships. It also sees the need to extend care actions to men, partners of these women, inviting them to reflect on the problem, encouraging them to adopt safer sexual practices.
The fact that this study was performed in a single setting restricted public clinic located in Salvador, Bahia, presented itself as a limitation, considering that the sample could be extended to contexts of private services, and other municipalities that would enable to compare social representations of women from variables such as class, access to health care and geographic location.
REFERENCES
1. Calazans GJ, Saletti FHC, França JI, Ayres JRCM. O conceito de vulnerabilidade. In: Padoin SMM, Paula CC, Schaurich D, Fontoura VA, organizadoras. Experiências interdisciplinares em AIDS: interfaces de uma epidemia. Santa Maria (RS): Editora da UFSM; 2006. p. 43-62.
2. Taquette SR. Interseccionalidade de gênero, classe e raça e vulnerabilidade de adolescentes negras às DST/AIDS.Saude soc. 2010; 19(supl.2): 51-62.
3. Rodrigues LSA, Paiva MS, Oliveira JF, Nóbrega SM. Vulnerabilidade de mulheres em união heterossexual estável à infecção pelo HIV/AIDS: estudo de representações sociais. Rev esc enferm USP. 2012; 46: 349-55.
4. Nichiata LYI, Bertolozzi MR, Takahashi RF, Fracolli LA. The use of the vulnerability concept in the nursing area. Rev Latino-Am Enfermagem. 2008; 16: 923-8.
5. Higgin JA, Hoffman S, Dworkin SL. Rethinking gender, heterosexual man, and woman’s vulnerability to HIV/AIDS. Am J Public Health. 2010; 100: 435-45.
6. Maliska ICA, Padilha MICS, Silva DMGV.Práticas sexuais e o uso do preservativo entre mulheres com HIV/AIDS. Ciênc Cuid Saúde. 2007; 6: 471-8.
7. Gomes AMT, Silva EMP, Oliveira DC. Social representations of AIDS and their quotidian interfaces for people living with HIV. Rev Latino-Am Enfermagem [Scielo-Scientific Electronic Library Online]. 2011 [citado em 09 set 2012]. 19: 485-92. Available at: http://www.scielo.br/pdf/rlae/v19n3/06.pdf.
8. Vala J. Representações sociais e psicologia social do conhecimento quotidiano. In: Vala J, Monteiro MBM. Psicologia social. 7ª ed. Lisboa (Po): Fundação Calouste Gulbenkian; 2006. p. 457-502.
9. Oliveira A, Amâncio L. A Análise factorial de correspondências no estudo das representações sociais: as representações sociais do suicídio na adolescência. In: Moreira ASP. Perspectivas teórico-metodológicas em representações sociais. João Pessoa (PB): Editora Universitária UFPB; 2005. p.323-62.
10. Vieira KFL, Coutinho MPL. Representações sociais da depressão e do suicídio elaboradas por estudantes de psicologia. Psicol cienc prof. 2008; 28: 714-27.
11. Silva CM, Vargens OMC. A percepção de mulheres quanto à vulnerabilidade feminina para contrair DST/HIV. Rev Esc Enferm USP [Scielo-Scientific Electronic Library Online]. 2009.[citado em 09 set 2012]. 43(2): 401-6. Available at: http://www.scielo.br/pdf/reeusp/v43n2/a20v43n2.pdf.
12. Aboim S. Risco e prevenção do HIV/AIDS: uma perspectiva biográfica sobre os comportamentos sexuais em Portugal. Ciênc saúde coletiva. 2012; 17: 99-112.
13. Karim QA, Sibeko S, Baxter C. Preventing infection women: a global health imperative. Clin Infect Dis [on line]. 2010. [citado em 04 set 2012]. 50(Supl.3): 122-9. Available at: http://cid.oxfordjournals.org/content/50/Supplement_3/S122.full.pdf+html.
14. Herrera C, Campero L. The vulnerability and invisibility of women facing HIV/AIDS: constant and changing issues. Salud Publica Mex. 2002; 44:554-64.
15. Cechim PL Selli L. Mulheres com HIV/AIDS: fragmentos de sua face oculta. Rev Bras Enferm. 2007; 60: 145-9.[citado em: 04 set.2012].Available at: http://www.scielo.br/pdf/reben/v60n2/a03v60n2.pdf.
16. Santos CO, Iriart JAB. Significados e práticas associados ao risco de contrair HIV nos roteiros sexuais de mulheres de um bairro popular de Salvador, Bahia, Brasil. Cad Saúde Pública. 2007; 23: 2896-905
17. Galvão MTG, Gouveia AS, Carvalho CML, Costa Ê, Freitas JG, Lima ICV. Temáticas produzidas por portadores de HIV/AIDS em grupo de autoajuda. Rev enferm UERJ. 2011; 19:299-304.
18. Amorim MM, Andrade NA. Relações afetivo-sexuais e prevenção contra infecções sexualmente transmissíveis e AIDS entre mulheres do Município de Vitória - ES. Psicol Estud. 2006; 11: 331-39.
19. Dias FLA, Silva KL, Vieira NFC, Pinheiro PNC, Maia CC. Riscos e vulnerabilidades relacionados à sexualidade na adolescência. Rev enferm UERJ. 2010; 18:456-61.
20. Filipe EMV, Batistella E, Pine A, Santos NJS, Paiva V, Segurado A, et al. Sexual orientation, use of drugs and risk perception among HIV-positive men in São Paulo, Brasil. Int J STD AIDS. 2005; 16: 56-60.