RESEARCH ARTICLES
Socio demographic and occupational characterization of readjusted and rehabilitated nursing staff
Pâmella CacciariI; Maria do Carmo Lourenço HaddadII; Marli Terezinha Oliveira VannuchiIII; Roseana Almeida MarengoIV
INurse, Mastering in Nursing, State University of Londrina, Paraná, Brazil, Scholarship holder from the Higher Education Personnel Coordination of Improvement, Researcher in the Research Center Group for Study and Research in Nursing Management Services. Email: pamella_cacciari@hotmail.com.
IIPhD, Professor in the Nursing Course at the State University of Londrina, Paraná, Brazil, Researcher in the Research Center Group for Study and Research in Nursing Management Services. Email: carmohaddad@gmail.com
IIIPhD, Professor in the Nursing Course at the State University of Londrina, Paraná, Brazil, Researcher Leader in the Research Center Group for Study and Research in Nursing Management Services. Email: vannuchi@sercomtel.com.br
IVNurse, Specialist in Occupational Nursing, Regional University Hospital of Northern Paraná, Londrina, Paraná, Brazil. Email: vilamarengo@uel.br
ABSTRACT: This study aims to characterize the socio demographic and occupational profile of rehabilitated and readjusted nursing staff in a Public University Hospital in northern Paraná, Brazil. A cross-sectional study carried out with 30 subjects. The data were produced by a characterization of population questionnaire. The results showed that the average age was 50.3 years old, 93.3% were female, 50.0% Caucasian, 40.0% were married, 90.0% worked in the institution for over 16 years. It was found that 90.0% of the reasons for readjustment and rehabilitation are related to limitations as a result of a physical disorder, and even so, 30.0% worked overtime. 20.0% were crowded in the Inpatient and Care Division. It is concluded that it is essential for health institutions to redeem the promotion of workers' health, because it was found that many of the injuries are predictable and preventable.
Keywords: Nursing, worker´s health, human resources in healthcare, employment rehabilitation
INTRODUCTION
Work has a fundamental role in the lives of people; it contributes to the formation of their identity, the construction of subjectivity, allowing that they participate in the effectiveness of social life, considered as an essential element for health1. In this regard, its realization, whatever it be, must occur in an integral way, participatory and flexible, in a dynamic process, not only aiming to standardize and sort actions, whereas it must consider the individual as a holistic being2.
The transformations occurring in recent decades in the working world have intensively influenced the health of individuals and the collective of workers. The increasing incorporation of microelectronics, informatics, telematics and the robotics added to a new and complex set of organizational innovations and profoundly changed the productive structure of advanced capitalist countries, and at distinct levels, the countries of late capitalist development, as is the case of Brazil, causing profound changes in organization, profound changes in work conditions and relations. Work intensification is characteristic in current phase of capitalism and has led to the excessive consumption of physical and spiritual energies of workers3.
In healthcare institutions, the human resources are the largest contributors to the care process with emphasis on the nursing team, which participates, in a continuous and uninterrupted flow of care, the planning and optimization being necessary of this population in health services.
Work relations as evidenced by the great competitiveness, by high levels of demand and productivity are factors that consequently promote changes in the disease process of all humanity4.
The adversities in the organization and in the social relations of work, i.e., in the way that the work process occurs, can unbalance the relationship between health and disease, manifested in the level of worker satisfaction, causing physical and mental illnesses in nursing professionals5.
During the Course of Residence on Nursing Services Management in a Public University Hospital, after developing practical activities in Service Specialized in Safety Engineering and in Occupational Medicine, several readjusted/readjusted workers were found. This policy at the institution is normalized by the Resolution of the Board of Directors no. 71/200 that defines functional rehabilitation as:
[...] the limitation of the employee to with pathology, health problem or diagnostic clarification, preventing them from exercising definitively and completely the activities for which he was appointed, and does not characterize a reason for retirement or leave for healthcare treatment6:2-3.
In this circumstance occurs the change position due to the worker's permanent disability to perform their function. Another situation that happens is the functional readjustment also normalized by the resolution, which has as its definition:
It is understood with readjustment functional limitation of the worker to work on pathology, health problem or diagnostic clarification, preventing them from exercising partially, for a limited time or permanently, the activities for which it was appointed, and that does not characterize a cause for retirement or leave for healthcare treatment6:2-3.
This procedure allows the reduction of the permanent activities roll inherent to the position held, due to definitive health restrictions presented by the worker, provided, that they maintain the basic function ot hteir position.
It is relevant to study the profile of workers readjusted and rehabilitated from a public institution in the state of Parana, so that the managers can define strategies that will contribute to the establishment of a proper human resources policy, in order to leverage its use and implement health promotion actions for this group.
This research is of paramount importance due to the low volume of publications on this topic, in addition to subsidizing the creation of an institutional policy for rehabilitated and readjusted workers, reemphasizing the promotion of worker health, emphasizing the idea that many of the injuries are predictable and therefore preventable.
The aim of this study was to characterize the sociodemographic profile and occupational exposure of nursing workers who have gone the process of professional readaptation or readjustment in a public university hospital.
LITERATURE REVIEW
Employee health has caused major concern for health institutions due to wearing of the worker, a result of long and double working hours, low wages, problems with interpersonal relationships, lack of human resources, unhealthy environment, activities and stressful situations interfere with the health of workers as well as reflecting in the completion of their work. This context affects the physical and mental health of the worker, being necessary to readjust this professional in their duties for which can perform as their professional activities.
Workers that exhibit morphological, psychological and/or physiological changes caused by illness or accident of the work may evolve with limitations that lead to temporary or permanent restrictions, which has the objective of preserving the worker from occupational risks or because of the inability to perform the activities for which they were appointed7.
Public institutions offer for workers to job security, so that the individual approved in a public contest has full-time status after completing the probationary period, only losing their jobs if found guilty in an administrative or union proceeding. Because of this stability, the workers have matured in the institutions, which can generate large managerial problems, because the worker presents a physical and psychological distress that could lead you to do not expend more its routine activities in the institution, being then one of reasons to readapt this professional in another function.
In 1990, it was published by Federal law no. 8,112, which in its Article 24, establishes that the rehabilitation "is the investiture of the worker in charge of assignments and responsibilities consistent with the limitation that has suffered in his physical or mental capacities, verified in a medical inspection"6,8.
It is found that the health and work process and the interventions in the area of worker's health aiming at changes in work processes and in how they are organized by the organization of work, in addition to seek better working conditions to promote health, prevent injuries and recover the health of the worker collective9.
METHODOLOGY:
A descriptive cross-sectional study, conducted in a public university hospital, located in the northern region the State of Paraná. A large institution provides care exclusively to the Unified Healthcare System, in various medical and surgical specialties, and operates in human resource training, continuing education, research and technological development.
The potential of the study population was composed of rehabilitated and readjusted workers crowded on the Nursing Board of that hospital. The nursing staff of the institution in this study is composed of nurses, technicians and nursing aids, operational and technical administrative assistants.
According to the data of the Service Specializing in Safety Engineering and in Occupational Medicine (SESMIT) of the institution, in February 2011, 71 workers were registered as rehabilitated and or readjusted officially by Occupational Medicine, in a quota of 915 Nursing Board members. However, of the 71 reviewers, 16 that were on the list, they were not in this condition, totaling 55 of the study population, in the data collection. This number may be underestimated, since it can identify professionals in this situation off the record, ie, by informal agreement between supervisor and employee.
The inclusion criterion was to belong to the nursing staff and formally be rehabilitated /readjusted. All workers of the nursing staff employees in this condition was invited, considering only those workers who were in active exercise of their functions during the data collection period. Employees on medical leave for more than 30 days, special leave and adoption leave were excluded.
Of the 55 readjusted and rehabilitated workers that comprised the initial population of this study, six had already retired, two were in the process of pre-retirement exercising a special leave, one refused to participate in the study, 15 were on medical leave during the data collection period and one had died. Thus, the final study population brought together 30 workers crowded in the various departments of the institution.
Data collection was conducted in the period from November 2010 to March 2011, using a questionnaire for sociodemographic and occupational characterization. The data were tabulated by the program Microsoft Excel 2007.
The research project was approved by the Ethics in Research Committee registered with the National Information System on Ethics in Research, protocol No. 198/10, CAAE No. 0160.0.268.268 -10. All the interviewees received and signed the Free and Informed Consent.
RESULTS
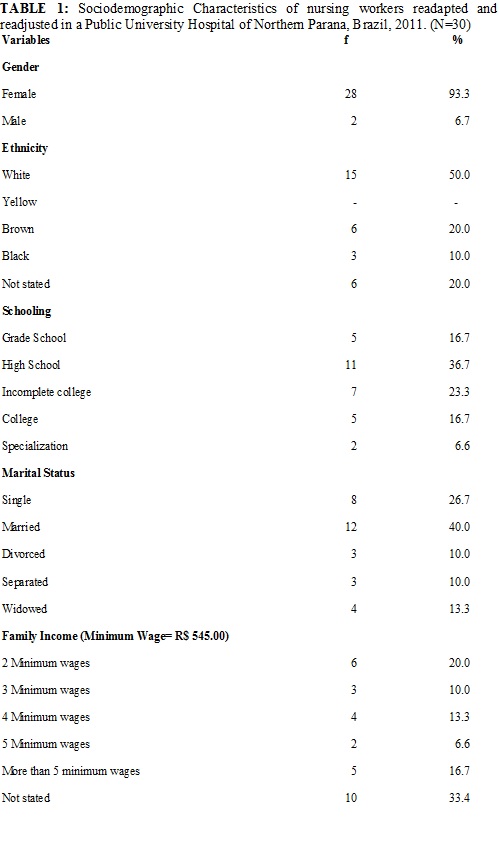
The age range has presented extremes of 40 to 65 years, with an average age of 50.3 years and median of 51 years. In relation to gender, 28 (93.3%) readjusted and rehabilitated are female, 15 (50.0%) Caucasian, 12 (40.0%) were married, all with more than 7 years of college education, and had an income greater than two minimum wages, as shown in Table 1.
Regarding the professional category, 14 (46.6%) are operational assistants and 12 (40%) nursing aids. The percentage of seating 6 (20.0%) is crowded in the Care Division, and Inpatient care followed by 5 (16.7%) in the Surgical Ward.
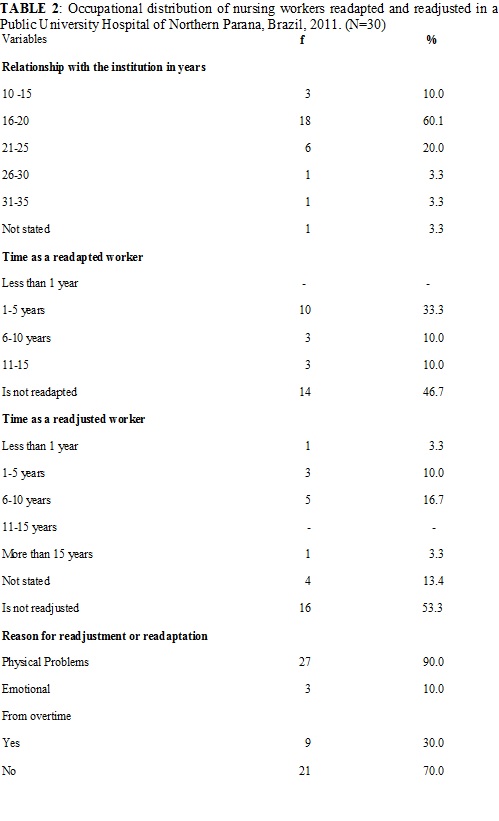
The occupational characteristics, where we can observe that 27 (90.0%) of the readjusted and readjusted working in the institution for more than 16 years, 16 (53.3%) are readjusted and 10 (33.3%) readjusted 4 (13.4%) did not respond. It was found that the reason for the readjustment and readaptation was by physical problems, 27 (90.0%), even with restrictions 9 (30.0%) of these workers took extra time, as shown in Table 2.
DISCUSSION
Assuming the results analyzed, has an average age of 50.3 years. According to the World Health Organization from 45 years of age, the worker presents decline in their functional capacity in reason of the decrease in muscle mass and resistance strength, as well as an increase in adipose tissue, characterizing the aging worker10.
The prevalence was female 28 (93.3%), being characteristic of the nursing profession. The care practices were always associated with the female gender. Revisiting the history, we see that with regard to social place of women, there is a myth defined by concepts that refer women to a condition of innate inferiority attributed to the approximation of their nature. Such representations have in its principles direct relation with the natural ability of biological reproduction and with the responsibilities to care for home and family11. Such affinity characteristics with the care process were criteria for inclusion of women in nursing by restricting the participation of men.
As for education, it was observed that the proportion of rehabilitated and readjusted individuals has over 11 years of education, predominance of the average level of education among professional nursing staff was found. The higher education also prevails among nursing professionals. These data reflect the requirement for the professional practice. It is highlighting that the support service is also being developed by professionals who, in addition to the practice, invest in theoretical knowledge. These results are very much in line with the other sectors in various localities, both the national and global levels, disposing that only the practice is sufficient to develop a valued and recognized professional activity. Simple as it is to do, this does not exempt the scientific knowledge and interpersonal relations12.
The cause of readjustment / rehabilitation is physical in 27 (90.0%), demonstrating that the conditions that led to the rehabilitation process were musculoskeletal system and connective tissue, which was also found in a survey conducted in a Hospital in the Interior of Sao Paulo state13. In a study conducted in Mobile Emergency Care Service - SAMU/Recife, PE with the nursing team 80% of workers had musculoskeletal symptoms14.
The nursing staff if exposed to the various positions such as the biological, chemical, psychological, as in this category examined. It was found that the mechanical and physiological postions, exemplified by the manipulation of excessive weight, working standing up, inappropriate and uncomfortable positions; night work and shift rotations; variety of activities; intensity of the work pace; in addition to their own work organization, are aspects possibly related to the occurrence of these injuries contributing to the genesis of musculoskeletal disorder4.15.
The readjustment / readaptation strategy has been developed to suit their workers in the work process despite their limitations. According to the study, the rehabilitated/readjusted population represents 6% of the Nursing Board staff, causing impact on management of the nursing staff, as well as requires technical competence of leadership in the organization of the work process to not further burden the team. The nurse manager of the team must identify the early emergence of diseases related to work and act in the resolution or escalation of the problem13.
In the daily routine of nursing, work overload and the little time for rest are situations that compromise the mental health of the worker, causing personal problems in interpersonal relations and in the performance of their professional activities16. The nursing professionals represent the largest and most complex work force of a hospital institution, both by its numeric quota as the heterogeneity of its composition (nursing aids and technicians, nurses), being present 24 hours with patients and in this manner presenting greater vulnerability to errors, recoveries and to stress16.
Workers' health is a priority today established for health services, as reflected in cases of sick leave, and also in situations where would be necessary in functional readaptation13.
Health promotion is guided to awaken a critical sense of man and the expansion of their knowledge, seeking to integrate it to the exercise of citizenship, thus knowledge is indispensable in the fight for the right to health and for better conditions of life17.
The actions of the worker's health include assistance to the aggravations, the surveillance of environments and working conditions, the situation of workers' health and the environmental situation. Included are also the production, collection, organization, analysis and dissemination of health information, the production of knowledge and educational activities, all designed under the control of the organized society. The cycle of comprehensive health care workers include, health promotion procedures defined and implemented within the health system and beyond, by sectors labor, social welfare, environment and government sectors responsible for economic and social development policies18.
One can see the obvious lack of training of both health professionals and the human resource professionals regarding the care, guidance and monitoring of clinical, social and labor rights of the rehabilitated professional, demonstrating the limited vision of wholeness of the human being proposed the Unified Health System in Brazil13.
CONCLUSION
The results obtained allowed us to outline the sociodemographic, readjusted, and rehabilitated occupational workers at a University Hospital of Northern Paraná. The majority was female, Caucasian, married, with more than seven years of study and had an income greater than two minimum wages. The reason that led to the readjustment and readaptation is related to limitations by physical disorder, and the majority of the workers in the operational assistant category.
This study showed the importance of the preparation of managers for the health of the staff under their supervision, emphasizing prevention, promoting worker health, and improving the quality of life of these professionals.
The limitation of this study highlights the downgrade of data relating to readjusted and rehabilitated workers. For the reason that the institution does not have dependable relation data; workers who find themselves on the list had already returned to their original functions; some were retired, hindering the data collection and demonstrating the importance of monitoring these workers and rethink actions developed for this population.
It is noteworthy that characterizing the demographic profile of these professionals guides the implementation of actions to promote health in this group, reflecting the quality of work life, the quality of care and empowerment of human resources.
It is essential that healthcare institutions employ strategies to promote health worker, because many of the diseases are preventable, sensitizing managers to the development of educational activities aimed at improving the quality of life of workers.
REFERENCES
1. Custódio IL, Moreira TMM, Lima FET, Freitas MC, Lima MMR, Silva AL. Saúde do trabalhador: caracterização das dissertações e teses nacionais de enfermagem, 2003-2007. Rev enferm UERJ. [Internet] 2010 [citado em 02 abr 2013].18:604-9. Available at: http://www.facenf.uerj.br/v18n4/v18n4a17.pdf
2. Trevisan JM, Robazzi MLCC, Garanhani ML. Sentimentos de prazer entre enfermeiros de unidades de terapia intensiva. Cienc Enferm. [Internet] 2009 [citado em 02 abr 2013]. 15:45-53. Available at: http://www.scielo.cl/pdf/cienf/v15n3/art_06.pdf
3. Elias MA, Navarro VL. A relação entre o trabalho, a saúde e as condições de vida: negatividade e positividade no trabalho das profissionais de enfermagem de um hospital escola. Rev Latino-Am Enferm. [Internet] 2006 [citado em 05 fev 2013]. 14:517-25. Available at: http://www.scielo.br/pdf/rlae/v14n4/v14n4a08.pdf
4. Leite PC, Silva A, Merighi MAB. A mulher trabalhadora de enfermagem e os distúrbios osteomusculares relacionados ao trabalho. Rev esc enferm USP. 2007; 41:287-91.
5. Manetti ML, Marziale MHP, Robazzi MLCC. Revisando os fatores psicossociais do trabalho de enfermagem. Rev RENE. 2008; 9:111-9.
6. Universidade Estadual de Londrina. Resolução CA n 71/2000 de 10 agosto de 2000. Determina novas normas para o programa de readaptação funcional. Londrina: UEL; 2000. p 2-3.
7. Ribeiro NF. Distúrbios musculoesqueléticos em membros inferiores em trabalhadoras de enfermagem. Rev Baiana de Saúde Publica [Internet] 2011 [citado em 11 fev 2013].35:128-42. Available at: http://inseer.ibict.br/rbsp/index.php/rbsp/article/viewFile/8/8
8. Presidência da República (Br). Lei n° 8.112, de 11 de dezembro de 1990. Dispõe sobre o regime jurídico dos servidores públicos civis da união, das autarquias e das fundações públicas federais. Diário Oficial da União, Brasília (DF), 11 dez 1990. Seção VII, p. 7.
9. Souza NVDO, Pires AS, Gonçalves FGA, Cunha LS, Shoji S, Ribeiro LV, et al. Riscos ocupacionais relacionados ao trabalho de enfermagem em uma unidade ambulatorial especializada. Rev enferm UERJ. [Internet] 2012 [citado em 10 mar 2013]. 20:609-14. Available at: http://www.facenf.uerj.br/v20nesp1/v20e1a10.pdf
10. Organización Mundial de la Salud (OMS). Él envejecimiento y la capacidad de trabajo: informe de un grupo de estudio de la OMS. Genebra (SWI): OMS; 1993.
11. Coelho EAC. Gênero, saúde e enfermagem. Rev Bras Enferm. [Internet] 2005 [citado em abr 2013]. 58:345-8. Available at: http://www.scielo.br/pdf/reben/v58n3/a18v58n3.pdf.
12. Costenaro AC, Stecca JP. Motivação profissional: um indicador de qualidade de vida. Rev Eletrônica Contab. [Internet]. 2004 [citado em 12 fev 2013].1:241-64. Available at: http://cascavel.ufsm.br/revistas/ojs-2.2.2/index.php/contabilidade/article/view/226
13. Batista JM, Juliani CMCM, Ayres JA. O processo de readaptação funcional e suas implicações no gerenciamento em enfermagem. Rev Latino-Am Enfermagem. 2010; 18:87-93.
14. Santos Júnior BJ, Silveira CLS, Araújo EC. Work conditions and ergonomic factors of health risks to the nursing team of the mobile emergency care/SAMU in Recife city. Rev Enferm UFPE. [Internet] 2010 [citado em 12 mar 2013]. 4: 246-54. Available at: http://www.ufpe.br/revistaenfermagem/index.php/revista/article/viewFile/746/500.
15. Zapparoli AS, Marziale MHP. Risco ocupacional em unidades de suporte avançado de vida em emergências. Rev Bras Enferm. [Internet] 2006 [citado em 15 jan 2013]. 59:41-6. Available at: http://www.scielo.br/pdf/reben/v59n1/a08v59n1.pdf
16. Silva LG, Yamada KN. Estresse ocupacional em trabalhadores de uma unidade de internação de um hospital-escola. Ciênc Cuid Saúde. 2008; 7:98-105.
17. Souza AR, Moraes LMP, Barros MGT, Vieira NFC, Braga VAB. Estresse e ações de saúde: contexto da promoção da saúde mental no trabalho. Rev RENE. 2007;8:26-34.
18. Dias EC, Hoefel MG. O desafio de implementar as ações de saúde do trabalhador no SUS: a estratégia da RENAST. Ciênc saúde coletiva. [Internet] 2005 [citado em 15 jan 2013].10:817-27. Available at: http://www.scielo.br/pdf/csc/v10n4/a07v10n4.pdf