RESEARCH ARTICLES
Promoting self-care of obese patients with coronariopathy: application of pender’s diagram
Iraci dos SantosI; Carla dos Santos SoaresII; Lina Márcia Miguéis BerardinelliIII
IPhD. in Nursing, Professor of the Department ofFundamentals in NursingProfessor in the Nursing Graduate Program, School of Nursing at the State University of Rio de Janeiro, Email: iraci.s @terra.com.br
IIMaster's in Nursing. Assistant Professor at the Faculty of Nursing of the University Center Serra dos Órgãos. Email: carlinhasoares@yahoo.com.br.
IIIPhD. in Nursing, Assistant Professor of the Medical-Surgical Nursing Department, Professor in the Nursing Graduate Program, School of Nursing at the State University of Rio de Janeiro, Email: l.m.b@uol.com.br
IVTaken from the Master's Dissertation of: Soares CS, Socioeconomic Conditions and obesity: the challenges for nursing in the promotion of self-care in contemporary society . Approved by the Graduate Program in Nursing at the State University of Rio de Janeiro, 2010.
ABSTRACT: This work aimedto identify self-care needs of clients with obesity and coronary artery disease applying Pender’s Health Promotion Model. Descriptive method, case-series type, which was implemented in a meeting with 30 clients assisted in nursing consultations at the outpatient cardiology unit, in a university hospital in Rio de Janeiro, Brazil, from 2009 to 2010. In the results needs were identified related to the conduct and personal factors; impairing and facilitating situational influences and nursing interventions for self-care.It was concluded that the client was encouraged by interactions and health education, which led them to reflection, awareness, interference on their lifestyle and autonomy for self-care. This is a challenge to overcome from a prevention model, which is solely responsible for the adherence or being the therapy conducted by the professional.
Keywords: Nursing; health promotion; self-care; nursing theory.
INTRODUCTION
Concern about the lifestyle is a constant in society due to individual decisions that affect health and on which it is possible to exercise a degree of control. Because the decisions and inappropriate habits towards health create risks arising from the individual themself. When these risks result in illness or death, it can be asserted that the life style contributed or caused the illness or dysfunction1.
Reverting unhealthy life styles becomes an imperative to public policies and health practices, through investment in interventions and actions oriented to behavioral factors such as non-pharmacological treatment of obesity and coronary artery disease (CAD).Health practices and public policies aimed towards educational proposals in order to orchestrate changes in life style to adopt healthy habits.
The success of the healthstrategies also involves the overcoming of important barriers, among them2: disinformation, resistance to change, social exclusion, the conflicts of interest and the distance between the knowledge. The nurse as a healthcareprovider becomes an intervener through guidance for the control of obesity of the client with CAD, since it proposes to integrated care, i.e. care associated with educating.
Over time, it has been considered that no profession cares more than nursing, because care is related to this profession, in the interactive secure and integrative care modes. Being that it is a human science, in addition to coming from the health field; the professionals build their actions with the people from their experiences, acquired by their experiences3.
Nola J. Pender, during the 1980s, introduced the Model of Health Promotion (MHP), whereas theoretical bases on the cognitive processes, the valorization of expectations of human motivation, personal attitudes and social norms, such as triggering the behavioral decisions4. From these bases, it was considered that the promotion of health (PH) depends on determinants of cognitive and perceptual aspects, which will subsidize meanings for making PH decisions as well as the behaviors.
The MHP is essentially a conceptual nursing model, to be used to implement and evaluate health promotion actions, allowing assessing of the behavior that leads to the promotion of self-care, by the study of the interaction of three main points: characteristics and individual experiences, feelings and knowledge about the behavior that they want to achieve and desirable behavioral health promotion4-7.
This model emerges in an attempt to identify factors that influence healthy behaviors and decisions on the life style adopted by people5,6. The lifestyle health promoter is an instrument that allows the recovery of the health of individuals, having utility for nursing care, both in support and in guidance for self-care of clients4-7.
Care associated with education transcends its basic precepts, because through the educating, there is training to intervene constructively /reflexive, singular/plural, dynamic /flexible, in a complex cultural and historical human relation between the subjects8.
Here situations are addressed arising from obesity, especially its occurrence in client with CAD. This is characterized primarily by an imbalance between the demand and supply of oxygen to the heart muscle caused by a decrease in the light of the coronary vessel, due to a complex process of thrombus formation. The clinical manifestations of CAD interfere with the autonomy of the individual, who is unable to exercise basic care towards human life, such as gaseous exchanges, nutrition, elimination, hygiene, or even administer aspects of important social impact, such as work and/or family8.
Obesity, considered as a public health problem and a worldwide epidemic, is caused by the imbalance between the intake and caloric expenditure. It demands a review of the client's life style involving dietary change, introduction of physical activities compatible with a healthy living, thus avoiding the increased intake of caloric foods. The increasingly sedentary nature of various occupations of adults, adolescents and children activities are the main contributing factors to this problem, which is at the root of chronic diseases such as hypertension, diabetes and renal disease8,9.
Focusing on the complications of obesity; complexity of the events which cause it; and people with heart disease, it emphasizes education as a transformation instrument under two main aspects of health promotion. Those which seek changes in the behavior of individuals, and thoserelated to their lifestyle, locating them within the family, and cultural environment of the community in which they are10,11.
Whereas the success of health strategies involves overcoming barriers, in order to balance the body dimensions of the human being asks is; what are the self-care needs of the client with CAD? Facing these observations the daily dynamics of health care, had as an objective:to identify needs for self-care among clients with obesity and coronary artery disease, applying the Pender's Health Promotion Model.
THEORETICAL-METHODOLOGICAL FRAMEWORK
The process of restructuring health practices reflects the concept and applicability of self-care (SC) in educational practices, there is no view of the proposed transition in the way of thinking in health organizations. Thus, the nursing care is perceived as an integral part of the survival process in human life. Because this is the essence of the profession, both in its objectivity, during the development of technologies and procedures, such as in subjectivities expressed in sensitivity, creativity and intuition12.
Education provides reflexive movement to the individuals, resulting in autonomy, therefore allowing themselves to be and realizing they are responsible for themselves, carrying out the SC, aiming at their well-being. Therefore, the PH is different, transforming them into collective activity that involves prevention, education, and participation of different segments of society13.
It is an expanded strategic perspective, where the incentive to autonomy for SC is not just an reductionist ideatowards adherence and accountability of the subject, from educational practices conducted by the involved health professional. Education enables individuals to resort to understood knowledge, raising levels of health, without harming the meaning of their own life13,14.
The development of strategies based on the promotion of a healthy lifestyle requires coordinated effort between the healthcare providers in various educational, governmental and industrial instances14. Thus, it is understood that health education and health promotion go hand in hand, being the awareness of the first step to self-care14.
The diagram proposed in the Theory of Nola Pender was applied as a conceptual schematic model6,15, which represents a multivariate paradigm, allowing explain and predict the component of PH and the style of living to investigate how individuals make decisions about the care of themselves, in the context of nursing. It’s reasoning in nursing theories, human development, experimental psychology and education have led to the use of a holistic perspective and psychosocial nursing whose theory offers a new vision on the pillars of the MHP.
The lifestyle health promoter is an instrument that allows the valorization of people's health; it is useful to nursing care, both in support and in education of clients. It mainly identifies the cognitive and perceptual factors as the main direct determinants of behaviors PH. This model revised in 2002, shows the identification of facilitator concepts of demonstrable hypothesis generation, aiming to diagnose nursing care needs6,16,17.
Method
Descriptive Study, time series of cases15, operationalized from February 2009 to July 2010, during the care of clients in nursing consultation (NC), in the cardiology outpatient clinic of the State University of Rio de Janeiro. Clients withoutinvasive therapeutic behaviorswere addressed as being an inclusion criteria for the sample selection, being enrolled in a CAD outpatient clinic; participant of the nursing consultation (NC); age between 50 and 70 years; both genders; signed the Free and Informed Consent form (ICF); capable of understanding the preserved; without difficulties to participate in the study (cognitive deficit, problems related to speech and locomotor problems).
The research was approved by the Protocol no. 223328, of the Ethics Committee of the State University of Rio de Janeiro. All subjects signed the informed consent form, after knowing the purpose, advantages and disadvantages of the research and agreed with the disclosure of their information, since their anonymity was respected.
Thesample selection considered the 7-day operation at the chosen NC, noting that 120 clients were scheduled for attendance; and, of these, 46 individuals were less than 50 or more than 70 years of age and were excluded from the study. There were, 74 individuals who met the inclusion criteria. Of this total, four subjects missed their scheduled appointment and 40 clients did not wait for the NC, whose duration was between 45 and 90 minutes of individual care. Therefore, the study sample was composed of 30 subjects.
A form composed by demographic characteristics was used: age, educational level, occupational status, family income, number of dependents, housing conditions; and behavioral factors: quality of diet; regular practice of physical exercise; risk factors for obesity: family history, anthropometric parameters: body mass index (BMI) and waist circumference (WC).
For the NC, a previously validated clinical record was used16 to develop the nursing process (NP), in the same institutional context of the field of research. The developed steps were research, nursing diagnosis, planning and formulation of nursing interventions for the healthcare needs of the consulted client´s self-care.
Since the perception of the clients regarding their needs for self-care,Pender's MHP diagram has been applied6, relating them if the following aspects: characteristics and individual experiences (previous behavior and personal factors); knowledge about the behavior - factors cognitive and affective influences (interpersonal and situational: intrusive and facilitators) and result of the ducts (institutional and professional and guidelines for the SC). The data were organized in the program Excel and submitted to simple descriptive statistics15. In the correlation of data,the following values and meanings: were considered, above 0.70 positive or negative points to a strong correlation; 0.30 to 0.70 indicate positive or negative moderate correlation, below 30 expressed weak correlation.
Corresponds to a limitation of this research the partial use of the nursing consultation, and the partial implementation of the MHP. It is reported that it was impossible to check the results of the nursing interventions proposed for consulted, clients considering the expected time for completion of the Master's Thesis.
RESULTS
Regarding the personal biological factors it was observed that, of the 30 (100%) study subjects, 24 (80%) are elderly, distributed equally in both genders; 19 (63.3%) were overweight or obese according to the BMI; and 26 (86.6%) have abdominal obesity, according to CA,.Regarding the sociocultural factors, predominantly Caucasian ethnicity Self-declared- 26 (83.3%), only 11 (36.6%) individuals cited labor activity, due to retirement, 23 (76.6%) only had elementary schooling, 20 (66.7%) have a family income of up to 2 minimum wages and in 16 (53.3%) families, up to four people depend on this income. All of them said they reside in their own homes, masonry, composed of four or five rooms, with running water and regular garbage collection.
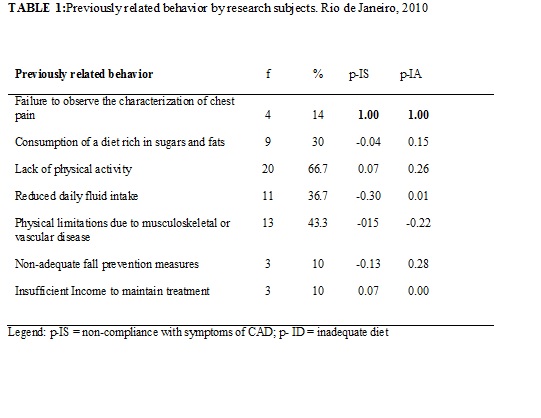
In relation to the behavior of the subjects prior to the development of actions aimed at the promotion of healthcare, it was observed that the majority- 20 (66.7%) did not practice physical activity, while 9 (30%) consumed an inadequate diet before obesity and the CAD. It is Noteworthy, also, that 4 (14%) clients are unaware of the characterization of chest pain as a symptom of heart disease. Associating this failure symptom of inadequate nutrition, we obtained 1.00, corresponding to the strong correlation. As For the reduced daily water intake, the correlation was moderate and the remaining items have reached low correlation, according to Table 1.
As for the cognitive and affective factors regarding the interpersonal and situational influences impeding the promotion of health/self-care, affirms that the emotional state of 1 (3.3%) client by loss (death) potential of a significant person, and the relations of conflict in family life, such as a difficulty to develop self-care actions informed by 5 (16.7%) people. Low education levels and poor knowledge on obesity, CAD and other diseases were found, also, in the majority of 25 (83.3%) subjects. See Table 2.
It is inferred that, such findings may result in inadequate health choices as well as the insufficient family income has contributed to the lower forward in promoting behaviors health promoters, fact perceived by a majority of 20 (66.7%) subjects. Relating the range of good level of self-perception to the consumption of diets rich in sugars and fats, a correlation of 0.92 was obtained. This index means that the high self-perception is inversely proportional to the energy consumption of the inadequate diet. The remaining items have reached low correlation, according to Table 2.
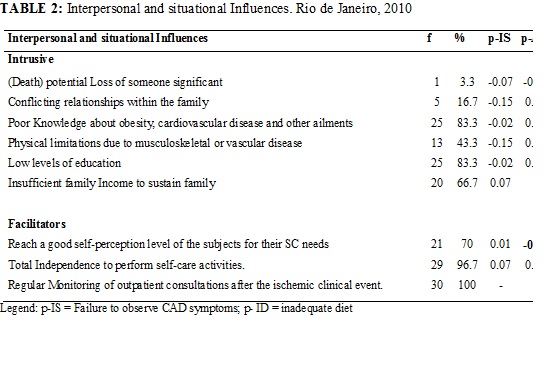
These impediments, are described as facilitating situational influences: the good level of self-perception in the majority of 21 (70%) subjects, despite the low schooling hinder the understanding of their needs of SC during the nursing consultation; the partial independence to carry out activities of SC, identified in almost all-29 (96.7%) clients. It surpasses the regular attendance at outpatient visits by all of the research subjects, as shown in Table 2.
Regarding factors related to income, insufficient wage income to maintain drug treatment, and education, it was observed, that they possess a high degree of correlation -0.92.
Before the identification of the needs for self-care, perceived and revealed by research subjects, during the NC, the following nursing interventions were highlightedincenting behaviors for the promotion of health of clients: maintenance of climate of trust and openness between professional /client /family; discourse/dialog favoritism and incentive on the emotional origin issues, related to self-esteem, self-motivation or personal competence; clarification on obesity, CAD and their injuries; guidance on relaxation techniques (stretching, complementary therapies); sensitive listening to complaints and comments from clients.
DISCUSSION
Applying the Health PromotionModel4-7,15,17, characterized in the Pender's diagram, personal factors of biological origin were highlighted which subsidized nursing interventions for self-care of the client with obesity and coronary artery disease. The finding of the uncontrolled obesity on the increase in abdominal circumference allows for the warning that it mainly leads to cardiovascular morbidity and mortality due to important metabolic changes caused by excess abdominal weight10.18. Therefore, through the information and encouraging awareness of the individual, invoking their own prior experience, it is expected to achieve changes in behavior and adoption of a healthy lifestyle4-6.
Recalling the MHP diagram, warning that the personal social factors correspond, among others, the socioeconomic status in which people are inserted4-6,15,17. It should be stressed that the research subjects with obesity criterion, according to the anthropometric standards, reside in their own home, built in masonry, composed of four or five rooms, with regular garbage collection and piped water. Meanwhile, have more than two people dependent on their low family income. This fact can trigger anxiety and stress.
On this subject, researchers together with community groups13,17 propose that the nurse will play the educator role as something directly political, precisely by facilitating the autonomy of groups that have a social disadvantage13,19, such as those with low education income insufficient to sustain the family. In this case, the choice of the best options on the lifestyle depends on the perceptual and cognitive abilities of the subjects, the main direct determinants of behaviors PH4-6, putting them as co-responsible for their health condition4.
This proposition refers also to educational practices for self-care awareness that mobilize people and taking healthy measures. The same occurs in the psychological health ambit, the condition of perceived health and the concept of health understood by clients, allowing them to define PH proposals4-6,8,20,21.
Self-perception of the lack of physical activity is highlighted among surveyed clients who are elderly, obese and still have CAD. They have physical limitations resulting from musculoskeletal or vascular diseases, as well as their daily water intake is reduced and consume a diet rich in sugars and fats. These results suggest that the development and intervention of medical technology have reached a small stratum population and showed a superficial and exclusionary form of aging. Therefore, disinformation, resistance to change and social exclusion are important barriers2,13 to be overcome for obtaining the PH based on SCactions4,5.
However, in addition to biological factors are the interpersonal influences, mainly those related to the emotional and spiritual dimensions experienced in family and social environments, because these are some factors that may hinder the SC exercise. The negative affection influence the personal ability to organize and execute a health-promoting behavior (perceived self-efficacy), as well as the properties of the stimulus behavior itself. The increase of feelings toward the self-efficacy and generate greater positive affection4-6.
The model for valuing human motivation based on rational behaviors, cognitive aspects in behavior decision correspond to the central construction of the MHP developed by Pender4,15. Still, without this information, it will be impossible to adopt behaviors that potentially foster health throughout life.
The good level range of subject's perception on their SC needs, independence to carry out these activities and attending regular outpatient consultations are considered facilitating situational influences for behavior promoters of health.
It is necessary that the nurses listens carefully to the client's complaints and comments or their perceptions and understanding of situations, whereas the socio-economic reality perceived constitutes a dimension that goes beyond the personal options. This reality consists fundamentally, in leaving the person aware of the public proportion and dependence on public policies with investments in health, education, compensation, and quality in work, type of housing, among others.
CONCLUSION
In their role of the nurse educator develops actions directed to the promotion and strengthening of responsible behaviors for the adoption of healthy lifestyles together with the client and communities. These actions allow the critical review of experiences of past losses, propitiating the acceptance of feelings (understanding or perceived health status, redefinition of health). It becomes essential to know the family history and monitor psychobiological responses, looking for those that demand stress.
Therefore, they were given guidelines for nursing care, considering the dimensions; psychobiological, emotional, mental/intellectual, psychosocial and psycho-spiritual.
Although the educational practices that, constitute one of the nursing professional tasks as well as aspects regarding the model centered in health promotion.The dissemination of the results is scarce in their activities for the identification of the needs for self-care of clients with obesity and coronary artery disease, in outpatient clinics. Whereas the multi factorial dimensions political, social, economic, behavioral.
The control of modifiable risk factors can be encouraged since the interrelationships with health professionals, including nurses, by being constantly closer to the client and their practice of care / education / research committed to providing them with information that the leads to reflection, awareness, interference on their lifestyle and self-care autonomy. However, the anxiety for that other proposals are articulated, faced with the reality of the subject's living conditions of life of individuals, it is a challenge to overcome a prevention model that responsibility alone adherence to therapy or not driven professional.
The perspective of this work, in order to emphasize future interventionist acts in nursing in the struggle for autonomy in the application of essential knowledge of this profession, incorporates other dimensions for comprehensive service to the client. The intention is this it will become a foundation for further development of new studies; referring to the more extensive philosophical, theoretical and technological reasoning that proposes the reconstruction of practices in caring, educating and nursing research.
The need to encourage nursing consultation systematically including the evaluation of the results obtained with nursing interventions. Therefore, this study's contribution is essential for the reduction of obesity indexes through self-care guidance. Remember that the effective development of the nursing consultation requiresprofessional qualification, in terms of competence, ability and interaction with the client,and institutional decision to be made in their amplitude.
REFERENCES
1. Lalonde M. A new perspective on the health of canadians: a working document. Ottawa (Ca): Editors April; 1974.
2. Cavalcante TF, Moreira RP, Araujo TL, Lops MVO. Fatores demográficos e indicadores de risco de acidente vascular encefálico: comparação entre moradores do município de Fortaleza e o perfil nacional. Rev Latino-Am Enfermagem [Internet]. 2010 [citado em 12 mar.2013]; 18 (4): [06 telas]. Available at: http://www.scielo.br/pdf/rlae/v18n4/pt_07.pdf
3. Santos I, Caldas CP, Gauthier J, Erdmann AL, Figueiredo NMA. Cuidar da integralidade do ser:perspectiva estética/sociopoética de avanço no domínio da enfermagem. Revenferm UERJ. 2012; 20: 4-9.
4.Sakraida TJ. Nola J Pender: Modelo de promoción de la salud. In: Alligood MR, Tomey AM. Modelos y teorías en enfermería. 7ª ed. Madrid (ES): Elsevier-Mosby; 2011. p 434-53.
5.Santos I, Alves ACS.[Promoting the self care of the elderly for healthyaging: application of Nola Pender Theory]. Texto e contexto enferm [Internet] 2010 [citado em 12 mar 2013]; 19: 745-53. Available at http://dx.doi.org/10.1590/S0104-07072010000400018
6. Pender NJ, Murdaugh CL, Parsons MA.Health promotion in nursing practice. 4thed. Upper Saddle River (NJ) : Prentice-Hall; 2002.
7. Victor JF, Lopes MVO, Ximenes LB.[Analisys of diagram the health promotion model of Nola J.Pender]. Acta Paul Enferm. [Internet]2005 [citado em 12 mar 2013]. 18: 235-40. Portuguese. Available at: http://dx.doi.org/10.1590/S0103-21002005000300002.
8. Ferraz F, Silva LWS, Silva LAA, Reibnitz KS, Backes VMS.Education and care in nursing: passport to the learning, education, and care in health. Rev Bras Enferm. [Internet] 2005 [citado em 12 mar 2013]. 58: 607-10. Portuguese. Available at: http://dx.doi.org/10.1590/S0034-71672005000500020.
9. Khawali C, Ferraz MB, Zanella MT, Ferreira SRG. Evaluation of quality of life in severely obese patients after bariatric surgery carried out in the public healthcare system. Arq Bras Endocrinol Metab. 2012; 56: 33-8.
10. Organização Mundial de Saúde. Obesidad y sobrepeso. Nota descriptiva, nº 311. Genebra (Swi):OMS; 2006.
11. Buss PM. Promoção e educação em saúde no âmbito da Escola de Governo em Saúde da Escola Nacional de Saúde Pública. Cad Saúde Pública. 1999; 15: 177-85.
12. Guedes NG, Moreira RP, Cavalcante TF, Araujo TL, Lopes MVO, Ximenes LB et al. Intervenções de enfermagem relacionadas à promoção da saúde em portadores de hipertensão. Acta Paul Enferm. 2012; 25:151-6.
13. Soares CS, Santos I, Berardinelli LMM. Obesity as a social problem: identifying guindance needs of nursing. Rev Enferm UFPE On line. 2010; 4:18-27.
14. Caetano JA, Soares E. Client's quality of life after myocardial infarction. Esc Anna Nery [Internet] 2007 [citado em 12 mar 2013]. 11: 30-7. Portuguese. Available at http://dx.doi.org/10.1590/S1414-81452007000100004.
15. Polit DF, Beck CT, Hungler BP. Fundamentos de pesquisa em enfermagem: métodos, avaliação e utilização. 6ª ed. Porto Alegre (RS): Artmed; 2011.
16. Amorim LC, Santos I, Albuquerque DC. Nursing assessment: research/care through the sensible listening in the heart failure clinic.2008; Online Brazilian Journal of Nursing 7: 30-6.
17. Santos SSC, Barlem ELD, Silva BT, Cestari ME, Lunardi. Promoção da saúde da pessoa idosa: compromisso da enfermagem gerontogeriátrica. Acta Paul Enferm. 2008; 21: 649-53.
18. Tarastuchuk JCE, Guérios EE, Bueno RRL, Andrade PMP, Nercolini DC, Ferraz JGG et al. Obesity and coronary intervencion: should we continue to use body mass index as a risk factor? 2008; Arq Bras Cardiol. 90:311-6.
19. Ferreira VA, Magalhães R.Obesity among the poor in Brazil: female vulnerability. Ciência & Saúde Coletiva. 2011; 16:2279-87.
20. Santos I, Rocha RPF. Needs of nursing guidance for self-care of clients on hemodialysis therapy. [Internet] 2011 [citado em 12.06.2013]; Rev Bras Enferm. 2011; 64: 335-42. Available http://dx.doi.org/10.1590/S0034-71672011000200018.
21. Silva MCS, Lautert L. O senso de autoeficácia na manutenção de comportamentos promotores de saúde de idosos. Rev esc enferm USP. 2010; 44:61-7.