FIGURE 1: Four-place chart of evocations of professionals from the Family Health Units to the inductor term family violence against elderly. Jequié-BA, 2012.
RESEARCH ARTICLES
Family health strategy personnel's representational structures regarding domestic violence against older adults
Elisama Nascimento RochaI; Alba Benemérita Alves VilelaII; Denize Cristina de OliveiraIII; Doane Martins da SilvaIV; Marta dos Reis AlvesV; Saulo Sacramento MeiraVI
I
Nurse. Master in Nursing by the Graduate Program in Nursing and Health, Universidade Estadual do Sudoeste da Bahia. Jequié, Bahia, Brazil. E-mail: elisamapq@hotmail.com
II
Nurse. PhD in Nursing. Associate Professor of the Graduate Program in Nursing at the Universidade Estadual do Sudoeste da Bahia. Jequié, Bahia, Brazil.
E-mail: albavilela@gmail.com.br
III
Nurse. PhD in Public Health. Professor of the Graduate Program in Nursing at the Universidade do Estado do Rio de Janeiro. Rio de Janeiro, Brazil. E-mail: dcouerj@gmail.com
IV
Nurse. Master in Nursing by the Graduate Program in Nursing and Health, Universidade Estadual do Sudoeste da Bahia. Jequié, Bahia, Brazil.E-mail: doane.ef@hotmail.com
V
Nurse. Master in Nursing by the Graduate Program in Nursing and Health, Universidade Estadual do Sudoeste da Bahia. Jequié, Bahia, Brazil. E-mail: martareisalves@yahoo.com
VI
Physical therapist. Master in Nursing by the Graduate Program in Nursing and Health, Universidade Estadual do Sudoeste da Bahia. Jequié, Bahia, Brazil.
E-mail: saulo_meira@hotmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2015.7450
ABSTRACT
Conducted from May to July 2012, this exploratory, quali-quantitative, descriptive study drew on the structural approach to Social Representations Theory to examine health professionals' representational structures regarding domestic violence against older adults. The study participants were 81 professionals from 16 family health care facilities in Jequié, Bahia State, Brazil. Data was collected by the technique of free evocation of words, and semi-structured interview. Evocations were analyzed using EVOC 2003 software, and the interviews were analyzed using thematic content technique. The representational structures identified were characteristically negative, underpinned by dimensions that shows professionals' confrontation of domestic violence against the elderly identified at Family Health Care facilities. Knowledge of these representations gives professionals and managers a sense of direction in developing strategies for promotion and prevention in the family and social contexts. Keywords: Violence; family; older adults; health professionals.
INTRODUCTION
Population aging is now a global phenomenon. From this perspective, in 1940, the Brazilian elderly population accounted for 4.1% of the total population, and now accounts for 12.1% in 2011. Thus, the absolute number increased from 1.7 million to about 23.5 million in the same period. Therefore, there has been a demographic trend since the 1970s: significant changes in the age structure of the population, towards aging. This is evidenced, in part, by the aging of families, which causes changes, and it is estimated that 9 million Brazilian elderly live in their adult children's, son or daughter-in-law's or other relatives' houses1.
Thus, it is emphasized that the population aging creates new demands on health services, inasmuch as it increases the number of elderly users in all levels of complexity 2.
They are mostly dependent elderly, who seek help from family to deal with their difficulties in daily activities and/or income. In this way, they become potential victims of family violence and potential demanding of a care policy1.
The domestic violence against the elderly encompasses any type of abusive relationship practiced in the private context of family against this group. It can be physical, psychological, financial, sexual or material, affecting elderly's quality of life3. In turn, this violence represents a major challenge for society in general and particularly for the health sector, since it causes deaths and also physical and emotional trauma, which creates a growing demand for health services4.
Therefore, the family health unit (FHU), which is the gateway of the local health system and composed of a multidisciplinary team, has a responsibility to take continuous and systematic monitoring of a number of families residing in a delimited territory, thus allowing knowledge of the living conditions of that population5.
Thus, the health professionals who compose the FHU teams are in a strategic position for early detection of potential situations of domestic violence and possible victims. Thus, it is clear that the beliefs, information and communication of health professionals who deal with these situations are embedded with representations that impact on their professional practice.
Therefore, the objective of this study was to analyze the representational structure of health professionals about domestic violence against the elderly.
THEORETICAL-METHODOLOGICAL FRAMEWORK
Study with multi-methodological approach: descriptive, exploratory, qualitative and quantitative. It was adopted as a theoretical and methodological approach of this work the Social Representations Theory in its structural perspective, also called the Central Core Theory. The social representation consists of a set of beliefs, information, opinions and attitudes of a group with similar characteristics, about a given social object. This set of elements is organized, structures and constitutes a social cognitive system of specific type6.
The Central Core Theory proposes the organization of social representations around a central core, which is the element that supports its fundamental and uncompromising sense. Thus, as an ontological characteristic of a central core of determined representation, it is emphasized the nature of the represented object, the kind of relationships the group has with this object and the system of social values and standards that constitute the living environment in the objective and subjective dimension of the individual and the group7.
The study population was 81 health professionals who worked in the chosen setting for the research, 16 FHU in the city of Jequié-BA, which were selected according to the following criteria: having the minimum team, according to the recommendations by the Ministry of Health, complete; teams with at least 6 months of implantation. We included professionals with more than 6 months professional activity in the context of the scenario chosen since the time factor is a determinant itself in the development of social representations. Professionals with less than 6 months professional activity in the context chosen were excluded, the time factor is a determinant in the development of social representations.
This study followed the ethical principles recommended by Resolution No. 196/96. We obtained approval by the Ethics and Research Committee of the Universidade Estadual do Sudoeste da Bahia (CEP/UESB) under Protocol 13355/2012; authorization from the Municipal Health Department of Jequié for the implementation of data collection; and signing the Informed Consent Form by each individual participant. The data collection period was from May to July 2012, for which we chose to use two instruments: the free evocation of words technique and a semi-structured interview.
The free evocation of words is a technique for collecting the constituent elements of representations. This technique enables to highlight the prominence and the hierarchical importance of the representation elements8. It also allows to highlight the semantic universe of the studied object, as well as its imagery dimension more quickly and objectively 9. The technique consisted in asking subjects to evoke five words or phrases when they heard the inducer term domestic violence against the elderly, which were immediately recorded and classified by subjects from most to least important.
A semi-structured interview allows the description, explanation and global understanding of a studied phenomenon, as well as the description of representational content relating to this phenomenon, making it possible to generate a communication interface between the researcher and the study's informant about a specific topic10.
Therefore, the free evocation of the 81 subjects was collected, and among these we chosen, at random, 22 professionals to participate in semi-structured interview. It is noteworthy that the evocation technique was performed first and was succeeded by the interview in order to prevent it from being influenced by interview.
The words from the evocation of words technique were typed and grouped in alphabetical order, generating a dictionary that guided the categorization of evocations, in which words with similar meanings were grouped. The product of the evocations was organized previously, constituting a corpus for analysis.
The material was then processed by EVOC (2003 version) software, which enables organizing the terms produced according to the hierarchy implicit in the frequency and average order of evocation (AOE) and favors the construction of the four-place chart. This program calculates and reports for the whole corpus, the simple frequency and average order of evocation of each word and the mean of the average orders of evocation or rang9, which in this study obeyed the average order of importance (AOI) assigned by subjects.
The use of this software generated reports that made possible the construction of the four-place chart, proposed by Vergès11. This technique, by combining two attributes related to the words or the evoked expressions, which are the frequency and the order in which they were raised or classified, enables the distribution of terms produced according to the importance attached by subjects9.
The four-place chart corresponds to four quadrants with four sets of terms. In the upper left quadrant are the truly significant terms for the subjects and that are probably the core of the study representation. The upper right quadrant is called as first periphery; in the lower left quadrant are located the contrasting elements; and the words located in the lower right quadrant are the second periphery of representation7,8,12.
Data from the interviews were analyzed following the thematic content analysis, according to Bardin13. Importantly, the quantitative procedure used in this study was restricted to the statistical analysis performed with the data obtained through the technique of free evocation of words. However, its results were analyzed qualitatively as well as the discourses that emerged from semi-structured interview. The testimonies of the study subjects were identified with the initial capital letter of the profession. For example, CHW acronym, in the case of community health worker, followed by an Arabic numeral.
RESULTS AND DISCUSSION
The subjects were 22 (27.1%) community health workers (CHW); 22 (27.1%) nursing assistants/technicians (A/T); 21 (25.9%) nurses (N); 7 (8.6%) doctors (DO); 5 (6.1%) dentists (DE) and 4 (4.9%) dental attendants (DA).
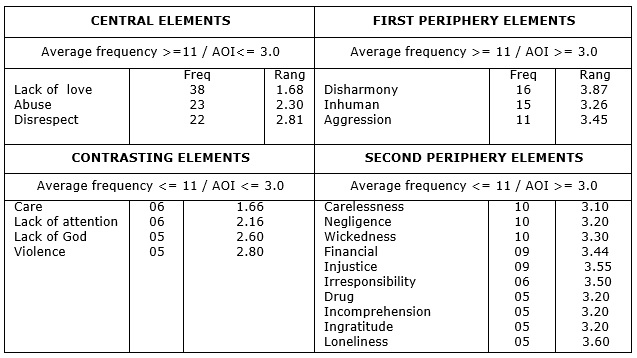
The analysis of the corpus formed by evocations of 81 informants revealed that in response to the inducer term domestic violence against the elderly, 394 words were mentioned, of which 115 were different. The rang, that is, the mean of the average order of importance was 3.0, while the average frequency was 11, and the minimum frequency, 5.
The crossing of the average frequency of words evoked with the mean of their average orders of importance allowed distributing the evocations in the four-place chart, which allows observing the contents of social representation as well as the structure and hierarchy of its elements, as shown in Figure 1.
FIGURE 1:
Four-place chart of evocations of professionals from the Family Health Units to the inductor term family violence against elderly. Jequié-BA, 2012.
It is observed in the upper left quadrant the possible central core of representation of domestic violence against the elderly to FHU professionals. In this quadrant, the following words are evident: lack of love, abuse and disrespect. These words are similar to be the most raised and classified in the first places, with a frequency exceeding 11. Also, the AOI is less than 3.0, being chosen by the subjects being as the most important in the hierarchy of words.
Importantly, the core is determined by the nature of the object represented, by the relationship the group has with that object and by the system of values and norms that guide the ideological environment of the moment and the group. Its elements stabilize and provide meaning to representations built by individuals.6
Therefore, the possible elements composing the core indicate the following dimensions: affective (lack of love), attitudinal (disrespect) and behavioral (abuse). These dimensions unfold in other quadrants, showing a semantic organization of the different elements constituting the social representation of the object under study.
In the first periphery (upper right quadrant) are the terms aggression, disharmony and inhuman, reflecting the behavioral (aggression), attitudinal (inhuman) and affective (disharmony) dimensions. Since the elements of the second periphery (lower right quadrant) suggest the presence of an imagery (drug-financial-loneliness), attitudinal (carelessness, negligence, incomprehension, ingratitude, irresponsibility) and behavioral (injustice, wickedness) dimension of family violence against seniors. Thus, there is a peripheral system that integrates the experiences and individual stories of social actors, which is sensitive to the immediate social context, but also flexible, allowing adaptation to the reality experienced by professionals14.
Among the contrasting elements (lower left quadrant), the following words were evoked: care, lack of attention, lack of God and violence. These words were chosen by the subjects as the most important in the hierarchy of terms produced; however, since their frequencies are below the average, they are not inserted within the core. It is observed, in that space of representational structure, three dimensions: attitudinal (lack of attention), affective (lack of God) and behavioral (violence).
In this context, when analyzing the aforementioned results, it can be stated that the subjects have a negative representation of domestic violence against the elderly, associated with four dimensions: emotional, attitudinal, behavioral and imagery.
In the affective dimension, the expression lack of love had the highest frequency (38) of evocations and was the second more readily classified of the entire set (1.68), appearing as the most important component of the central core, revealing that the subjects set the roots of this representation in this element. This dimension is unfolded in the second periphery by the word harmony, and in contrasting elements through the expression lack of God.
Thus, this dimension is anchored in elements that reflect the conflicts existing in family relationships, which can lead to situations of violence. At the same time, there is the influence of religion on anchoring this representation, when professionals report a lack of God pervading manifestations of domestic violence against the elderly.
It can be inferred that the occurrence of situations of domestic violence against the elderly reveals previous family conflicts that are expressed in the form of violence. So if there is violence because there is conflict; there may even be love, but it is a conflicted love15.
On the other hand, the attitudinal dimension appears recorded in terms of disrespect, carelessness, irresponsibility, incomprehension, ingratitude, lack of attention, inhuman and negligence. This dimension reflects the negative attitudes of family for the elderly, which are evidenced by violation of rights provided by law, psychological abuse and little or no responsibility in supplying the needs of this population. These manifestations are corroborated in the testimonies of professionals.
[...] disrespect to the old person [...], thinking that they did not have the right to take responsibility for the senior, [...] thinking that they did not have to be careful with them [...] he is 90 or so years old, he already has a very high disability. (N1)
[...] Lack of patience with the elderly, swearing [...]. (N76)
In this scenario, domestic violence against the elderly becomes a major problem, particularly with the growing aging population, accompanied by a low coverage of long-term health care and the decreased availability of family caregivers for these elderly16. Added to this context, new forms of household arrangements and stress of modern life provide to the family, the state and society major challenges to be faced.
The term inhuman is interconnected with terms injustice and evil, which appear in the second periphery of representation, expressing attitudes that are embedded in the phenomenon of violence, revealing the social devaluation of the elderly, begun in the family context. This context was elucidated in the reports of informants.
[...] because they ceases to be a human being, to be treated as a human being, and starts to be a human being treated like garbage, because even an animal is free to come and go, they let the elderly by themselves, and the bedridden elderly does not [...] they cannot get out of there, they are hostage to their own family [...]. (CHW61)
The behavioral dimension is expressed in concrete elements related to family violence, such as abuse, which appears in the central core with the second highest frequency of the entire analysis (23), and the contrasting element violence, which is part of the inductor term of the representation under study. On the other hand, the term abuse is also related to the various negligence demonstrations against the elderly, which the professionals of the family health strategy (ESF) identify in the daily life of many families. Similarly, these manifestations are evidenced in the subjects' speeches.
[...] lack of food at the right time to the elderly [...] they let the elderly without bathing for too long, with the diaper, let them hungry, give medication at the wrong time, that sort of thing [...] Regarding hygiene, they leave the room dirty, dark, stinking because they do not want to care [...]. (CHW61)
Also in this dimension, the element aggression, which appears in the first periphery together with the word inhuman, is a term that refers to a specific type of domestic violence against the elderly: physical violence. It is observed in the statements of informants the manifestation of physical aggression against elderly practiced by family members, in the context of FHUs, showing the contact of professionals with these situations.
[...] a son attacked his mother [...] and he beat her and the patient arrived here with problems and then she called the police, the police came, and then he pretended it was someone else, but he had attacked his mother [...]. (N70)
In Brazil, it is common cohabitation between different generations, as a reflect of the aging population and changes in family structures. Cohabitation intensifies the intergenerational interaction with different shared values, which may result in a favorable context for the establishment of conflict in the home environment that often result in violence against the elderly17.
With regard to imagery dimension, which is present only in the lower right quadrant on the periphery of the representation, it can be said that the words drug, financial and loneliness illustrate contributing factors for the occurrence of domestic violence against the elderly, which are present in daily life of professionals. It is required from these professionals, besides a special attention to this population, the development of prevention strategies in family and social context of the community under their responsibility. Thus, it is emphasized that the representations act as a guide for practices as also for the actions and social relations14.
In this context, the terms negligence and loneliness reflect the family's responsibility in the abandonment of the elderly, by exposing them to situations that threaten their safety and security. This reality was said in the subjects' speeches.
[...] they leave the senior alone, once it got to the point that the house was in fire and neighbors had to break the door to take the elder off of it [...]. (CHW50)
Thus, it noteworthy that the construction of violence against the elderly is determined by many factors that lead both the victim and the offender to a hostile environment, in which violence is developed. In this sense, there is in the imagery dimension the presence of the term drug, which portrays a social issue increasingly present in the context of FHU, which is the presence of alcohol and other drugs in the family context, interfering in its daily routine. Informants reported the identification of this problem as a predisposing factor to the occurrence of family violence against seniors.
[...] a son used the money from the elder to drink, inviting many people to drink and to use other things in the house, and the old man, was there, dirty, mistreated [...]. (CHW 50)
Therefore, it is highlighted that the misuse of alcohol and drugs becomes a potentiating agent for the occurrence of these events in the family 18. In a retrospective study, with data obtained from the Sistema de Informação de Agravos de Notificação (Notifiable Diseases Information System, Net version -SINAN Net), including reports of domestic, sexual violence and/or other types of violence in the elderly population, the physical violence, negligence and sexual abuse were related to the consumption of alcohol by offenders19.
Also in this dimension, the word financial reflects one of the strong reasons of domestic violence against the elderly, which are the economic issues. In this sense, the testimony portrayed manifestations of financial violence against the elderly within the family:
[...] they are exploited, the family has them at home as an income source [...] and does not use this income to the elderly's treatment, and they lack even medication. (CHW 16)
[...] often the elderly are providers not only for the children, but also for grandchildren and sometimes for great-grandchildren [...]. (N71)
Thus, it is observed that the dependency reported by respondents may contribute to intensify conflicts and generate violent behavior because the elderly are the financially responsible for the income; however, they are under the custody and responsibility of the family 18. It is observed that financial exploitation is accompanied by negligence demonstrations. Situations that mark the financial abuse against the elderly are in accordance with research conducted with professionals working in primary health care, whose findings revealed that the elderly are deprived of their resources for the benefit of family members, which is a frequently observed practice, increasing their vulnerability to conflict situations and the potential risk for violence20.
It is interesting to note the presence of word care as a contrasting element in the representational structure, that despite having low frequency (6), was the word ranked in first place, with the lowest rang of the entire analysis (1,66). It is noteworthy that, in a characteristically negative representation, the presence of a positive element in this area points to the existence of a subgroup of professionals who stresses the need for care of the elderly, as compensation or balance of violence effectively developed within the family.
In this regard, it is highlighted that the interpersonal relationship between the professional, the elderly and the family, representing the health care practiced by this professional, may prove important in the everyday care of this group.
In this context, it is noteworthy that the ESF team, when entering in the elderly/family's home, must foster care with actions directed to their health needs, considering their specificities, but also the family as a whole. Also, it is important to emphasize that for health services to fight against violence, it is required the development of inter-sectorial actions, not limited to isolated actions, guided by linearity, with health care coordination and other services21.
In this context, this study reveals that the approach to family violence by primary care professionals involves not only the discussion of the theme in the everyday life of health services, in professional training and interdisciplinarity, but also the establishment of inter-sectorial actions22.
CONCLUSION
The social representation of the studied group on domestic violence against the elderly is characteristically negative, sustained by the dimensions: emotional, attitudinal, behavioral and imagery, portraying thus the symbolic construction of these professionals in the daily work of FHU, faced with this multiple-facets phenomenon.
The representations evidence a scenario of different manifestations of violence against the elderly, practiced by family members, such as physical and psychological abuse, negligence, financial exploitation and abandonment. In this sense, the knowledge of this representation can enable better targeting in developing promotion and prevention strategies of violence in the family and social context of the FHU by professionals and managers.
Thus, the results of this study may provide support for professionals from various fields who are committed to tackling this problem.
There is need to broaden perspectives on the phenomenon of domestic violence against the elderly and rethink more effective actions, not only in political, economic and social perspective, but also encompassing the extent of public health and nursing.
This study was conducted in a context of primary care, specifically in the ESF, and therefore has limitations on the generalization of the results, given the qualitative approach adopted. In addition, it points out paths for further research to explore the presence of domestic violence against the elderly in other settings and contexts, in terms of social thought. Thus, it is pertinent that new studies on this subject are made.
REFERENCES
1.Instituto de Pesquisa Econômica Aplicada (IPEA). Tendências demográficas mostradas pela PNAD 2011. Rio de Janeiro: Comunicados do IPEA; 2012.
2.Oliveira MAS, Menezes TMO. A enfermeira no cuidado ao idoso na estratégia saúde da família: sentidos do vivido. Rev enferm UERJ. 2014; 22:513-8.
3.Organização Mundial da Saúde. Relatório mundial violência e saúde. Genebra (Swi): OMS; 2002.
4.Moraes CL, Aparatto Junior PC, Reichenheim ME. Rompendo o silêncio e suas barreiras: um inquérito domiciliar sobre a violência doméstica contra idosos em área de abrangência do Programa Médico de Família de Niterói, Rio de Janeiro, Brasil.Cad SaúdePública. 2008; 24: 2289-300.
5.Rosana A. Conhecendo o território. In: Aquino R, organizadores. Manual para treinamento introdutório das equipes de saúde da família. Salvador (BA): Pólo de Capacitação, Formação e Educação Permanente de Pessoal para Saúde da Família; 2001.
6.Abric JC. A abordagem estrutural das representações sociais. In: Moreira ASP, Oliveira DC, organizadoras. Estudos interdisciplinares de representação social. Goiânia (GO): AB Editora; 2000. p. 27-38.
7.Gomes AMT, Oliveira DC. A estrutura representacional de enfermeiros acerca da enfermagem: novos momentos e antigos desafios. Rev enferm UERJ. 2007; 15: 168-75.
8.Sá CP. Núcleo central das representações sociais. Petrópolis (RJ): Editora Vozes; 1996.
9.Oliveira DC, Marques SC, Gomes AMT, Teixeira MCTV. Análise das evocações livres: uma técnica de análise estrutural das representações sociais. In: Paredes AS. Perspectivas teórico-metodológicas em representações sociais. João Pessoa (PB): Editora Universitária UFPB; 2005. p. 573- 603.
10.Triviños ANS. Introdução à pesquisa em ciências sociais: a pesquisa qualitativa em educação. São Paulo: Atlas; 2009.
11.Vergès P. Approche du noyau central: propriétés quantitatives et structurales. In: Guimelli C. Structures et transformations des représentations sociales. Lausanne (Swi): Delachaux et Niestlé; 1994. p. 233-54.
12.Reis AT, Oliveira DC, Gomes AMT. Representações sociais sobre saúde entre adolescentes de escolas públicas do município do Rio de Janeiro. Rev enferm UERJ. 2009; 17: 473-8.
13.Bardin L. Análise de Conteúdo. Lisboa ( Pt): Edições 70; 2010.
14.Oliveira DC, Gomes AMT, Pontes APM, Salgado LPP. Atitudes, sentimentos e imagens na representação social da sexualidade entre adolescentes.Esc Anna Nery. 2009; 13: 817-23.
15.Goldfarb DC. Pensando nas origens da violência. Ciênc saúde coletiva. 2010; 15: 2669-76.
16. Jackson JL, Mallory R. Aggression and violence among elderly patients, a growing health problem. J Gen Intern Med.2009; 24: 1167-8.
17.Abath MB, Leal MCC, Melo Filho DA. Fatores associados à violência doméstica contra a pessoa idosa. Rev Bras Geriatr Gerontol.2012; 15(2): 305-14 . Aggression and Violence Among Elderly Patients, a Growing Health Problem Aggression and Violence Among Elderly Patients, a Growing Health ProblemAggression and Violence Among Elderly Patients, a Growing Health Problem
18.Santos ACPO, Silva CA, Carvalho LS, Menezes MR. A construção da violência contra idosos. Rev Bras Geriatr Gerontol. 2007; 10: 129-40.
19.Mascarenhas MDM, Andrade SSCA, Neves ACM, Pedrosa AAG, Silva MM, Malta DC. Violência contra a pessoa idosa: análise das notificações realizadas no setor saúde - Brasil, 2010. Ciênc saúde coletiva. 2012; 17: 2331-41.
20.Wanderbroocke ACNS, Moré CLOO. Significados de violência familiar contra o idoso na perspectiva de profissionais da atenção primária à saúde. Ciênc saúde coletiva; 2012; 17(8): 2095-103.
21.Gomes NP, Bomfim ANA, Diniz NMF, Souza SS, Couto TM. Percepção dos profissionais da rede de serviços sobre o enfrentamento da violência contra a mulher. Rev enferm UERJ. 2012; 20:173-8.
22.Lobato GR, Moraes CL, Nascimento MC. Desafios da atenção à violência doméstica contra crianças e adolescentes no Programa Saúde da Família em cidade de médio porte do Estado do Rio de Janeiro, Brasil. Cad Saúde Pública 2012;28:1749-58.