RESEARCH ARTICLES
Primary Care and infertility: knowledge and practice of nurses working in the family health strategy
Escolástica Rejane Ferreira MouraI; Rebeca Pinho Romero VieiraII; Andrezza Alves DiasIII; Danielle Rosa EvangelistaIV; Camila Félix AméricoV
INurse, PhD in Nursing, Professor of the Nursing Department at the Federal University of Ceará, Researcher for the National Council of Scientific and Technological Development, Fortaleza, Ceará, Brazil, email: escolpaz@yahoo.com.br.
IINurse, Master’s student in Nursing through the Graduate Program in Nursing at the University Federal of Ceará, Fortaleza, Ceará, Brazil, email: rebecaprv@hotmail.com.
IIINurse, Master's Degree in the Graduate Nursing Program at the Federal University of Ceara, Fortaleza, Ceará, Brazil, email: andrezzaalvesdias@hotmail.com.
IVNurse, PhD in Nursing, Professor at the Federal University of Tocantins, Tocantins, Palmas, Brazil, email: enfadanielle@yahoo.com.br.
VNurse, Master's in Nursing, Doctoral Student at the Graduate Program in Nursing at Federal University of Ceara. Fortaleza, Ceará, Brazil, email: cfamerico@yahoo.com.br.
ABSTRACT: To assess the knowledge and practices of nurses concerning infertility in primary care. Quantitative, cross-sectional study, carried out with 171 nurses in the Municipal Health System of Fortaleza-CE, Brazil. Data were collected through interviews, from November 2009 to April 2010. Likert scales were used to assess the knowledge and practice of nurses. The predominant sex was female, age and time of work in family planning varied from 25 to 53 years of age and one younger than 23 years, respectively. The knowledge level of 100 (58.5%) nurses on the concept of infertility was limited; of 169 (99%) on types of infertility none; and 106 (62%) and 65 (57%) had limited knowledge and slightly appropriate practice on the actions that can be offered in primary care focused on infertility, respectively. Nurses need training targeted at infertility.
Keywords: Infertility; family health program; professional competence; primary health care.
INTRODUCTION
Procreation is fundamental to the life of the majority of individuals, in particular women, which have maternity reaffirmation of femininity, indeed inherent in society since antiquity, in women who conceived were extolled, while considered infertile were punished by the gods, discriminated against in society and symbol of death1.
Infertility is the inability of a couple to conceive or carry a conception to term after a year or more of regular intercourse without the use of contraceptive technology2. The causes may be associated with the male and female factors, where men account for approximately 40% of cases3.
It is estimated that, in the world there are 50 to 80 million infertile couples, with the occurrence of approximately two million new cases per year3. In Brazil, more than 278 thousand married couples have difficulty in generating a child at any time in life, due to some type of infertility, primary or secondary. Primary infertility is one in which the couple never conceived, and the secondary occurs when the couple has one or more conceptions4.
Study found association between psychosexual problems and infertility, finding association with decreased libido in both partners, especially when infertility exceeded five years; transient impotence and premature ejaculation in men, as the most prevalent. In associating the infertility with emotional reactions, anxiety, was the most common in women, and depression, in men5. Stress can be present in the period of examinations for discovery of the causes of infertility, being the most critical period for many couples. In addition, the fear of receiving an infertility diagnosis and the reason that women do not seek help in health services, because, for many, this is a condition that they prefer hide to protect themselves from the social stigma1.
In view of the foregoing, the infertility was demonstrated as a problem that affects a significant portion of couples of reproductive age, however, actions offered in basic healthcare can result in success in the conception of these couples. Therefore, the question was elaborated: which knowledge and practice of nurses working in the Family Health Strategy (FHS) about infertility and assistance actions developed this level of care focused on the conception? Replying to this inquiry is relevant, because it will culminate in significant contributions to family planning services (FP), in order to guide and perform actions favorable to the conception of infertile couples in basic healthcare. In this context, the objective of this study was to assess knowledge and practice of nurses in relation to infertility in basic healthcare.
LITERATURE REVIEW
The Decree no. 426, of March 22, 2005, instituted under the Unified Health System (SUS), the National Policy of Integral Attention in Assisted Human Reproduction, (AHR) which, among other recommendations, establishing the identification of the causes of infertility among couples of childbearing age and defines technical criteria for the effective operation of the services that they perform with AHR techniques. Primary healthcare should be the gateway for the infertile couple to SUS, this should be performed anamnesis, clinical and gynecological laboratory exams to diagnose diseases that interfere with pregnancy such as Pap smears, serology for HIV, hepatitis B, hepatitis C, syphilis, toxoplasmosis IgG, fasting glucose, spermogram and rubella vaccination4,6.
It is estimated that 70% of infertility cases are resolved in primary care, with the deployment of low cost actions and procedures, of which only 30% are worthy of referral to services of greater complexity7.
Recognizing the female fertile period may be the solution for many infertile couples, which may be guided in primary health care. According to the Decree no. 388, of July 06, 2005, which deals with the organization and deployment of networks state and municipal attention in), AHR, and allocation of the health professional's basic care provide guidance on the identification of the fertile period and concentrate sexual relations during this period, as well as eliminate any factor that interferes in the warehouse of semen into the vagina or hinders the sperm migration through the female genital tract4.
In the clinical practice of health education (CEPS), the University of Sagrado Coração (USC), for example, patients who sought care by the team of medical genetics, with the desire to conceive, were forwarded to receive instruction regarding the method of Billings or ovulation. Of the 16 couples accompanied with complaints of infertility, nine managed to pregnancy and three babies were born. Usually, the couples can achieve pregnancy after two years after the adoption of the method. Some had already been forwarded to banks of semen and in vitro fertilization, but managed to get pregnant by using the natural method8.
METHODOLOGY
Cross-sectional survey, the type survey, with a quantitative approach, performed in Municipal Health System (MHS) in the city of Fortaleza, with nurses in the FHS, from November 2009 to April 2010.
The MHS was composed of six Regional Executive Secretariats (BE), in which worked 319 ESF teams. Of these, 306 worked with nurses, being 39 crowded on SER I, 37 in SER II, 57 in SER III, 32 in SER IV, 67 in SER V and 74 in SER VI9.
The population consisted of 306 nurses of the FHS and the probabilistic sample was generated on the basis of the formula for calculating with finite populations, corresponding to 171 nurses. Stratifying the sample between the be obtained: 22 Nurses in SER I, 21 in SER II, 32 in SER III, 18 in SER IV, 37 in SER V and 41 to be seen. For each SER, was chosen for convenience of accessibility to researchers, the Centers for Family Health (FSC), necessary to contemplate on each of them, and visited a total of 65 of the 90 FSC of t he MHS.
The data was collected through a structured interview, held in a private place and on occasion scheduled, so as not to interfere in the activities of nurses.
The data were organized in Statistical Package for Social Science (SPSS), version 18.0 for Windows and Epi Info version 3.3. They were analyzed by means of descriptive statistics to include absolute frequency, relative frequency, average (χ), standard deviation (S) and confidence intervals (CI).
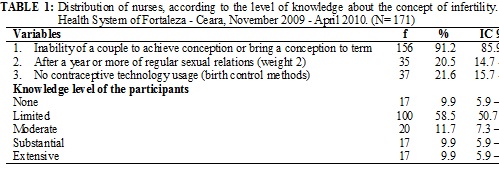
To assess the knowledge of nurses on the concept of infertility, the actions to be offered in primary care in the area, as well as the application of them, Likert scales were used. The scale for the assessment of knowledge about the concept of infertility consisted of three items taken on the basis of the concept of the World Health Organization (WHO)2. They corresponded to: the inability of a couple to achieve the conception or lead a conception the term (weight 1); after a year or more of regular sexual relations (weight 2); and without use of conception technology (weight 1), so that if the nurses did not mentioning any of the conditions, your knowledge would be evaluated as none ; citing at least one of the conditions, except the second, limited knowledge ; quoting two of the conditions, except for the second, or just want to mention the second, moderate knowledge; quoting two of the conditions, always contemplating the Second, substantial knowledge ; and citing the three conditions, extensive knowledge .
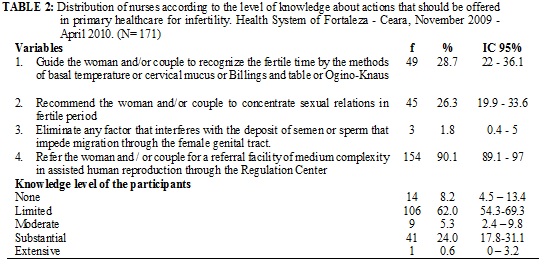
The evaluation of knowledge and practice about the actions for infertile couples consisted of four items, as recommended by the Decree no. 388, July 06, 2005: guide to women and/or couples to recognize the fertile period by means of the methods of baseline body temperature, Billings or cervical mucus and Ogino-Knaus or table; recommend the woman and/or couple to concentrate sexual relations in the fertile period; eliminate factors that interfere with the deposit of semen into the vagina or hinders the sperm migration through the female genital tract; and forward the woman and/or couple to a reference service for medium complexity), AHR, through the Regulation Center4.
With regard to knowledge, when the nurse did not mention any of the actions, their knowledge was rated as none, to name at least one of the actions, limited knowledge; citing two actions, moderate knowledge; citing three of actions, substantial knowledge; and citing all actions, extensive knowledge.
In the same way, when the nurses did not mention any of the actions, their practice was assessed as inadequate ; to quote one of the actions, slightly adequate; quoting two of the actions, moderately adequate; citing three shares, substantially adequate ; and citing all the actions, completely adequate.
The research project was approved by the Ethics Committee of the Federal University of Ceara (UFC), obtaining assent through the protocol no. 293/09. The guideline requirements and standards of research in human beings we met, presented in Resolution no.196/96, of the National Health Council (NHS), on the ethical issues in research involving human beings10. The participants signed the consent form, agreeing to voluntarily participate in the study.
RESULTS AND DISCUSSION
Characterization of the participants
Most of the group, that is, 152 (88.9%) consisted of women, sex historically predominant in nursing. The age ranged between 25 and 53 years, with an average of 35.68 years and S of 6.048. The time of graduation ranged from 2 to 30 years, with an average of 11.16 years and S of 5.141, with a higher percentage of participants with up to 10 years of training, corresponding to 92 (53.8%) nurses. The length of time working in FP ranged from less than one to 23 years, with an average of 9.29 years and S of 4.156. Therefore, the survey included young nurses, thus recent graduates, and older nurses. This condition is common in the composition of the FHS teams, for which converge newly graduated professionals and even professionals at the end of their career, which give preference to a life more hinterlands, far from large urban centers. The time of graduation between 2 and 30 years corroborates the aspect of age, covering professionals less and more experienced. The length of time working in FP also corroborates the ages of nurses and the time of graduation, as it brought together nurses with less than 1 to 23 years working in their field.
The Federal University of Ceara (UFC), Universidade Estadual do Ceará (UECE) and University of Fortaleza (UNIFOR) were responsible for the training of 160 (93.6%) of participants, whose distribution was equitable in the three major universities in Fortaleza, 57 (33.3%), 54 (31.6%) and 49 (28.7%), respectively. Other universities outside the State formed 11 (6.4%) of the participants.
Knowledge of nurses on infertility
Of the 15 nurses who did not mention the item 1, one reported that infertility was the presence of hormonal deficiency of the couple, however, it is known that the infertility is not just a consequence of the absence or low hormone production, but a number of factors such as: endometriosis, cervical infections, varicocele, and antibodies production against sperm, among others. The other 14 reported that infertility was only because of the women, as shown in Table 1. In this respect, it is said that when it comes to infertility, there is a great impact on the woman's identity, since femininity is, generally, associated with motherhood11.
Of the 136 (79.5%) nurses who were unaware of the item 2, 10 (5.8%) mentioned that for a couple considered infertile, was required a minimum of two years of trying to get pregnant with unprotected intercourse, referring to the concept as no longer valid. Others, 2 (1.2 %) reported a minimum period of six months to one year and three to four years, therefore, inconsistent with the literature11-15. See Table 1. It is said that 25% of the couples get pregnant in the first month of exposure, 60% at six months and 80% within a period of one year. The remaining 20% on average 15% conceive in the second year of exposure and, therefore, a more conservative classification was used for the concept of infertility12.
For conception to occur, the couple should not be using contraceptives (CM), because by using them, the chances of pregnancy are reduced, varying according to the effectiveness and suitability of the chosen CM of use. Disregarding this criteria in the concept of infertility, as was done by 134 (78.4%), may incur false diagnosis and unnecessary interventions. Another aspect to be highlighted is the lasting effect of injectable contraceptive exclusively with progestin after suspension of the use, which can reach up to four months13.
The level of knowledge of nurses on the concept of infertility ranged between none and extensive, predominantly the number of nurses with limited knowledge, accounting for 100 (58.5%). It is noteworthy that 34 (19.8%) nurses presented substantial or extensive knowledge. See Table 1.
Regarding knowledge about the types of infertility (primary and secondary), 2 (1.0%) and 169 nurses answered correctly (99%) did not know. Limited knowledge on the types of infertility can compromise the quality of care delivered, because the finding of paternity / maternity former is an approach that identifies the type of infertility, which affects the flow of the interview and the approach to be followed.
The level of knowledge and practical suitability of nurses on the actions which can be carried out in primary care, in accordance with what is established in Decree no. 388, July 06, 2005 4, are analyzed below.
The fertile period corresponds to the period in which the conception is possible, i.e. , three to four days before the expected date of ovulation and the two days following this 3. The role of the primary healthcare professional is to clarify the patient and/or couple on the physiology of the conception, since many couples are unaware of the definition and the means for identification of the fertile period. For identification, the health professional must resort to methods of fertility awareness-based (FAB), which are techniques of self-observation for signs and symptoms of fertility that occur in the female body during the menstrual cycle: basal body temperature, or Billings cervical mucus and Ogino-Knaus or rhythm12. However, such clarification was not of professional knowledge, since 49 (28.7%) mentioned the importance of teaching the couple to recognize the fertile period and 45 (26.3%) reported the need to guide the couple to focus sexual relations during this period. See Table 2.
Research was conducted with 2,055 menstrual cycles of 851 healthy women and emphasized that in 601 pregnancies, 25% occurred with a single episode of sexual intercourse and that there was no increase in the rate of pregnancy with multiple sexual acts, which demonstrates that the occurrence of pregnancy depends on the time of coitus and not the quantity of sexual relations. The fertile period prescribed is the right time for intercourse results in pregnancy and can be realized by means of FAB14.
It is established that the primary care team should explain to patients about practices that hinder the conceptions, such as the use of lubricants or post coital vaginal douches13. However, only 3 (1.8 %) nurses said they know such information.
In addition, various styles of life have a negative impact on fertility, and may be aggravated when added to advanced age. Through educational activities, the professionals who work in the FHS must promote healthy lifestyles, encouraging the abandonment of practices detrimental to conception15.
Item 4 has been referred to, by 154 (90.1 %) nurses, as shown in Table 2. It discusses the need to know how to refer a patient complaining of infertility for a service of greater complexity, would be based on the knowledge about the parameters in which this routing should be performed? The study did not investigate this aspect, and also did not assess whether patients were referred through the Regulation Center or informally, which was recognized as limitations to be overcome in future studies.
The level of knowledge of nurses on the actions that should be undertaken in primary care focused on infertility also varied between none and extensive, with predominance of the number of nurses with limited knowledge, corresponding to 106 (62.0%). Only 1 (0.6%) nurses reached level of extensive knowledge. Forward the woman and/or couple for a reference service for medium complexity was the most common knowledge between the participants, cited by 154 (90.1%) of these. See Table 2.
Practice of the primary care nurses aimed at infertile couples
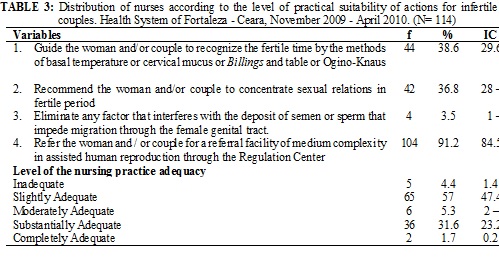
With regard to the receipt of women and / or couples with infertility need in the field last year, 114 (66.7%) nurses said they have rendered service in this area, thus justifying the reduction of 171 to 114 subjects in Table 3.
The practice of forwarding the woman and/or couple was cited by the majority, 104 (91.2 %) nurses, corresponding, also, the action of greater knowledge on the part of respondents, according to Table 3. Research conducted in seven cities in Turkey showed an inferior result to that found in this study, since the 748 participating physicians, 57.6% reported as activity provided assistance to infertile couples, the routing to a service of greater complexity16.
In general, there was a balance between what the nurses that demonstrated knowing and those reported performing, but were results that showed ignorance and inadequate care to infertile couples.
A study carried out in Belém, Salvador, Curitiba e Goiânia, in which interviews were conducted with the coordinator of women's health, coordinator of the FHS, managers at primary healthcare units and FHS teams, resulting in a total of 99 interviews, showed that the professionals of FHS teams not realized the FP as part of primary care. Although in the same survey in two cities in the country, assistance for FP did not include assistance for infertility, lacking a care protocol and referral system. In the other two capitals, infertility care was part of the actions in FP, including a referral system FHS teams to specialized services, however, in one of these municipalities there was no consistency between information of managers and professionals17.
Practices slightly adequate and substantially adequate were more common in the group surveyed, representing 65 (57%) and 36 (31.6%) of the nurses, respectively. Forwarding the woman and/or couple for a referral service for medium complexity was the most common practice, reported by 104 (91.2 %) of nurses, according to Table 3. This practice has proved to be effective in a study with 25 users of a FHS of Fortaleza, Ceara, which showed that the same is considered satisfied with the referral system for the SUS network18.
The FHS proposals facilitate a longitudinal user’s care, since the nurse meets the registered population, which allows establishing a bond with the community. As a FHS professional one should give an integral and effective care19, which cannot be observed in the study, since a considerable part of the nurses interviewed did not provide adequate care for infertile couples.
In a cross-sectional survey carried out in Brazil, with the objective of verifying the availability of the infertility service in the country, 19 (76%) state authorities have stated that there was no available service in their state. At the municipal level, 26 (66.7 %) authorities reported that their municipalities did not receive funding from the government for this purpose. Among the states and municipalities whose infertility services were available free of charge, only four (six states) and eight (13 cities), had implemented a standard for monitoring in infertility 20, which can justify the low quality care found in this study.
CONCLUSION
The research findings reflect the quality of care provided to infertile couples, since most nurses disowned their duties to act in this area and only one nurse demonstrated extensive knowledge about the health care activities that should be undertaken in primary care, in the field of infertility.
The plot was limited to a portion of nurses who knew and/or guided about the natural methods and their justifications for not conducting orientation proved to be permeated by prejudice.
It is suggested that, in future studies, the referral of patients to the secondary level of care is checked as occurs, since this information was not given in this study, it was recognized as a limitation of the study.
Moreover, it is reiterated that all health care professionals should have the responsibility to stay updated, however, is the role of MHS Fortaleza promote training in all areas of the FHS priority service, to improve the care provided in the field of infertility.
REFERENCES
1. Cunha MCV, Carvalho JA, Albuquerque RM, Ludermir AB, Novaes M. Infertilidade: associação com transtornos mentais comuns e a importância do apoio social.Rev psiquiatr Rio Gd Sul. 2008; 30: 201-10.
2. Direcção-Geral da Saúde (Por). Programa Nacional de Saúde Reprodutiva. Saúde Reprodutiva, Infertilidade. Lisboa (Por): DGS; 2008.
3. Gonçalves J. Avaliação do casal infértil. Rev Port Clin Geral. 2005; 21: 493-503.
4. Ministério da Saúde (Br). Portaria nº 388, de 06 de julho de 2005. Brasília (DF): Ministério da Saúde; 2005.
5. Omu FE, Omu AE. Emotional reaction to diagnosis of infertility in Kuwait and successful clients’ perception of nurses’ role during treatment. BMC Nurs. 2010; 9: 1-10.
6. Ministério da saúde (Br). Portaria nº 426/GM, de 22 de março de 2005: institui, no âmbito do SUS, a Política Nacional de Atenção Integral em Reprodução Humana Assistida e dá outras providências. Brasília (DF): Ministério da Saúde; 2005.
7. Pedrosa J. Jornal de Brasília [site de Internet]. Política prevê atenção integral. [citado em 30 jun 2005]. Available at: http://www.sistemas.aids.gov.br/imprensa/Noticias.asp?NOTCod=65742.
8. Universidade do Sagrado Coração. Clínica de Educação para a Saúde [site de Internet]. Método promove controle natural de fertilidade [citado em 28 ago 2012]. Available at: http://www.providafamilia.org.br./site/index.php.
9. Secretaria Municipal de Saúde. Célula de Atenção Básica. Informe do Programa de Saúde da Família. Fortaleza (CE): Secretaria Municipal de Saúde; 2009.
10. Ministério da Saúde (Br). Conselho Nacional de Saúde, Comitê Nacional de Ética em Pesquisa em Seres Humanos. Resolução nº 196, de 10 de outubro de 1996: diretrizes e normas regulamentadoras de pesquisa envolvendo seres humanos. Brasília (DF): Ministério da Saúde; 2003.
11. Khetarpal A, Sihgh S. Infertility: Why can’t we classify this inability as disability? Australas Med J. 2012; 5: 334-9.
12. Ministério da Saúde (Br). Assistência em planejamento familiar: manual técnico. Brasília (DF): Ministério da Saúde; 2002.
13. Agência para o Desenvolvimento Internacional dos Estados Unidos. Johns Hopkins University. Organização Mundial da Saúde. Planejamento Familiar: um manual global para profissionais e serviços de saúde. Baltimore (USA): OMS; 2007.
14. Bilian X, Heng Z, Shang-chun W, Xiao-ping J, Chang-hai H, Wen-qi S, Zhen-wu L. Concepcion probabilities at different days of menstrual cycle in Chinese women. Fertility and Sterility. 2010, 94: 1208-11.
15. Utting D, Bewley S. Family planning and age-related reproductive risk. The Obstetrician & Gynaecologist. 2011; 13: 35-41.
16. Hassa H, Ayranci U, Unluoglu I, Metintas S, Unsal A. Attitudes to and Management of fertility among primary health care physicians in turkey: an epidemiological study. BMC Public Health. 2005; 5.
17. Osis MJD, Faúndes A, Makuch MY, Mello MB, Sousa MH, Araújo MJO. Family planning in Brazil today: an analysis of recent research. Cad Saúde Pública. 2006; 22: 2481-90.
18. Clares JWB, Silva LMS, Dourado HHM, Lima LL. Regulação do acesso ao cuidado na atenção primária: percepção dos usuários. Rev enferm UERJ. 2011; 19: 604-9.
19.Baratiere T, Marcon SS. Identificando facilidades no trabalho do enfermeiro para o desenvolvimento da longitudinalidade do cuidado. Rev enferm UERJ. 2011; 19: 212-7.
20. Makuch MY, Petta CA, Osis MJD, Bahamondes L. Low priority level for infertility services within the public health sector: a Brazilian case study. Hum reprod. 2010; 25: 430-5.