RESEARCH ARTICLES
Between suffering and pleasure: vulnerability for nurses in their interpersonal relationships
Érick Igor dos SantosI; Antonio Marcos Tosoli GomesII; Denize Cristina de OliveiraIII; Caren Camargo do Espírito SantoIV
INurse, PhD student and Master in Nursing from the State University of Rio de Janeiro, Professor of the Augusto Motta University Center, for the Undergraduate and Graduate program in Nursing. Researcher in the research group "Health Promotion and Practice of Nursing Healthcare in population groups", Rio de Janeiro, Brazil, E-mail: eiuerj@gmail.com
IINurse, PhD in Nursing from the Federal University of Rio de Janeiro, Professor and Assistant Coordinator of the Graduate Program in Nursing, State University of Rio de Janeiro, Professor at the Faculty of Nursing, State University of Rio de Janeiro, Department of Medical-Surgical Nursing, Researcher in the research group "Health Promotion and Practice of Nursing Healthcare in population groups", Rio de Janeiro, Brazil, E-mail: mtosoli@gmail.com
IIINurse, PhD in Public Healthcare, University of São Paulo (USP), Professor in the Nursing Graduate Program at the State University of Rio de Janeiro, Professor in the Faculty of Nursing at the State University of Rio de Janeiro, Department of Nursing Fundamentals, Leader of the research group "Health Promotion and practices of nursing care and Healthcare in Population Groups", Rio de Janeiro, Brazil. E-mail: dcouerj@gmail.com
IVNurse, PhD student and Master in nursing from the State University of Rio de Janeiro, Researcher of the research group "Health Promotion and practices of nursing care and Healthcare in Population Groups", Rio de Janeiro, Brazil, E-mail carencamargo.enf@gmail.com
VIntegral part of the dissertation entitled: Vulnerability of nurses in caring for patients with HIV/AIDS - a study of social representations, linked to the research group Health Promotion and practices of Nursing Care and Health of Population Groups and approved in February 2012 by the Graduate Program of the Faculty of Nursing at the State University of Rio de Janeiro.
ABSTRACT
This study aimed to analyze the social representations developed by nurses on their vulnerability concerning their interpersonal relations maintained with patients who live with HIV/AIDS. In this qualitative and exploratory study, the Social Representations theory and method in its procedural approach was adopted. By means of semi-structured interviews, thirty nurses at a municipal hospital in Rio de Janeiro, Brazil, in 2009 participated in the study. With regard to the data analysis, the thematic content analysis was performed through the software NVivo 9. Nurse’s vulnerability that was verbalized in fear, underestimation and in suffering for the patient’s suffering, contributes to empowerment configuration, that was expressed in terms like personal satisfaction with the nurse’s activity, the patient’s trust and time of experience in caring for seropositive people. It is concluded that interpersonal relationships between nurses and patients are affected positively or negatively by episodes arising in the expression of vulnerabilities.
Keywords: Nursing care; occupational health; health vulnerability; acquired immunodeficiency syndrome
INTRODUCTION
This researchv aims to study the social representations made by nurses about their vulnerability in the context of interpersonal relationships they maintain with human immunodeficiency virus (HIV) seropositive patients.
The chronic illness, de per si (by itself) can lead to feelings of impotence against the disease1, either by the patient or the nurse who cares for the individual. However, caring for people in which is in a stage of irreversible and stigmatizing illness as is the case of Acquired Immune Deficiency Syndrome (AIDS) may affect the self-esteem of the caregiver who witnesses the fatality as a result of the disease process, regardless his dedication efforts. This illustrates how the experiences within the care scope can make nurses to revisit their knowledge and practices from the moment of care2 that they experience together with the HIV seropositive patients. Thus, it is postulated that the weaknesses of one may influence the other.
From these constructs, has been established the aim of this study which is to analyze the social representations made by nurses about their vulnerability in interpersonal relationships which they maintain with HIV seropositive patients who are under their care. In addition to the lack of scientific production about the vulnerability of nurses in the context of care - mainly in its psychosocial dimension - the multidimensional character of the intertwining of personal and professional vulnerabilities under the aegis of AIDS makes this study even more relevant.
In the case of nursing care to the seropositive individual, because AIDS and its historic, biomedical and social constructions concern on the daily lives of nurses and patients, the relationships maintained between them can affect negatively and/or positively their lives. Regarding these relationships, two recent3,4 studies have concluded that, under the vulnerability perspective, the ties between patients and nurses may have the tenacity and the narrowing necessary to encounter fragilities which, in turn, reconfigure themselves from the moment they touch.
Some authors3-5 start from the assumption that, to a greater or lesser degree, we are all vulnerable of falling ill, and assume that the factors that make someone susceptible to AIDS are not limited to the individual dimension, but must include environmental, economic, social, psychosocial, cultural and gender, for example. These propositions are in addition to the approach of some other authors6-10 that excels in trying to develop indicators that can measure the state of vulnerability of different population groups.
In this study, the following definitions apply to vulnerability as the dynamic and changeable state of fragility or disability typically human, holder of different dimensions and fruit of many different factors and intrinsic and extrinsic situations to the health system user or professional imbued with its care. This state drives them to formulate strategies to face, setting up thus their empowerment ante the experience of procedural intercourse health-illness-care3,4.
According to this proposition, the vulnerability is not limited to susceptibility or to contamination by a pathogen. It encompasses everything that poses a threat to the physical, moral, mental, spiritual, social or emotional for nurses and patients in care.
It is worth mentioning the uniqueness that nursing holds in relation to studies of the manifestations of the phenomenon of vulnerability11,12. Through their interactive essence, includes knowledge and socio-professional practices that, when applied, have the ability to uncover fragilities and ways of protection that would hardly be accessed by other health professionals4. Moreover, when providing care to patients, nurses often are too hard on themselves, beyond their physical, emotional and mental capacities. In this sense, the vulnerability that integrates the practice of nursing, gains expression in the encounter, in the conversation, in the exchange of values and in the implementation of procedures that enable the experience of interpersonal relationships.
THEORETICAL METHODOLOGICAL REFERENTIAL
A theoretical and methodological approach was adopted for this work, the Theory of Social Representations13 in its procedural approach14, developed in a Social Psychology perspective. The social representations are present in culture, communication processes and social practices, they are therefore multifaceted and constantly moving which is triggered by social interaction15. The procedural approach was chosen to outline this research for its guidance to the constituents’ aspects of representations.
This study was composed of thirty nurses who performed their work activities in the scenario chosen for the study, at a municipal hospital in Rio de Janeiro - Brazil, a reference in treatment for HIV/AIDS and/or tuberculosis. The reason for this number is the consensus within the Theory of Social Representations as a minimum quantity to recover the social representations in a group15,16. Professionals with less than six months in the professional activity in the context of the scenario were exclude by the time factor set as a determinant in the development of social representations. No other attribute was set up as a justifiable exclusion criterion.
The chosen techniques for data collection were the sociodemographic questionnaire to characterize the subjects and an in-depth semi-structured interview. The interviews were guided within the study scenario and captured on a digital recorder and audiotape, being transcribed and then analyzed. The data were collected from June to August 2009.
The analysis technique selected was the thematic17 content after systematization18, operationalized by QSR NVivo 9. This computerized tool was chosen to instrumentalize the qualitative researchers for the exploration, organization, analysis and graphical presentation of information until now, unstructured, whether they be textual, iconographic, videographic, phonographic, video phonographic, tabulated, among others. Its operation is based on the principle of coding and storage of data in specific categories, which is consistent with theoretical postulates of thematic analysis.
The ethical principles of human research were adopted and obeyed, in accordance with the standards of Ministry of Health resolution 196/96. The project to which this study belongs was submitted to the Ethics Committee of the Health Department of the Municipality of Rio de Janeiro and was approved under the protocol No. 200/08.
Throughout of the textual body the transcription of discursive excerpts will be carried out which best represent the topics of categories under discussion. In order to guarantee the anonymity of the subjects was assigned to each of them, the letter E of Interviewed - "Entrevistado" (in Portuguese) - followed by the number of their testimony.
RESULTS AND DISCUSSION
The subjects are mostly female (87%), belonging to the age group 41-45 years (27%), Catholic (40%), with a partner (70%), with post-graduation lato sensu (90%), with 16 or more years of institutional experience (37%), 16 or more years of working together with HIV patients (30%), due care at the time of data collection (63%) and with access to scientific information (77%).
The instrumentalized analysis by NVivo 9.0 resulted in 1696 Units Registry (RU), distributed into seven categories, which represent 100% of the analyzed corpus. The present study will further the category of number four, which holds 159 UR, divided into 13 topics and equivalent to 9.4% of the corpus.
This study will further the category of number four, which holds 159 UR, divided into 13 topics and equivalent to 9.4% of the corpus. These are understood as components of human3 empowerment.The empowerment by owning affective, attitudinal, symbolic, practical, cognitive and others dimensions will be addressed as an object of representation4 that emerged in association with the vulnerability. Considering the complexity of the results, a discussion will be performed on two axes whose distinction is more didactic than real in representational framework of the nurses in this study: one linked to vulnerability and the other to empowerment.
Axis 1: manifestations of vulnerability in interpersonal relationships maintained between nurses and patients with HIV/AIDS
The time of care2 experienced by the patient with HIV/AIDS can increase the vulnerability of nurses who assist them. The vulnerability is present in the relationship with the patient, because of its re-signification by nurses, in addition to being asymmetric, harms them and makes them as targets of devaluation.
There are patients who think that you are there as if you were a mere person to do any job. They don’t appreciate you. (E12)
[...] He thinks I am his housekeeper [the patient] Housekeeper in the pejorative sense. [...]They do not analyze you are their main care figure. Therefore, I still see that we are far from the patient seeing us as essential. (E22)
The devaluation of labor activity performed or the overlap of the figure of other professionals to the detriment of his are conflicting traits to the self-image of the protagonist of constructed care by nurses. In addition to identifying the devaluation, the subjects attribute its occurrence to the lack of consideration by patients on the situation of being cared by nurses. In the context of basic care, a study19 identified no social representation of the nurse's own practice among users of the National Policy on Sexually Transmitted Diseases and AIDS. It is believed that the visibility of nursing and nurses be viable from massive initiatives to make explicit what is private and nuclear to the profession that, for the similarity of professional autonomy while social reconstruction of reality, is in the construction process20.
In sum to the perception of devaluation of its making by patients, seem to exist in the inter-subjective relations between nurses and patients with AIDS, professional fragilities triggered by the involvement with those fragilities arising from the patient.
That [the patient's suffering] have already generated a discomfort for me, you know? A malaise and, often, I could not even do the care, you know? [...] because I end up with pitying them, thinking that I can't do anything [...][E1]
[...]I used to get very fond of the patients. I had friendship with them, with the family. I used to bring that problem to home, stayed home concerning about the patient. I used to get too much involved and it was making me suffer. (E12)
In the perspective of nurses, involving yourself too much is something that implies in certain degree of suffering. The discomfort and pity likewise emerge from the interaction of perception of nurses about the barriers that are faced by patients towards their survival. The vulnerability in this case is shown to be shared. This sharing is verbalized by nurses using terms such as involving yourself too much, suffer together and put in their place.
The nurses in the study are struggling to address the patient towards the uncertainty of his reaction to know their diagnosis.
I do not know how to deal [with the patient]. How do I give the news to the patient if I do not know what kind of reaction they may have and how I will deal to support them on that? Will he run out of here? Will he kill himself? (E2)
Many are aggressive with us! They think that because they are calling you have to serve them at that moment. My colleague was pregnant and took a slap in the face by a patient with AIDS because he was angry. (E29)
In the settings of the subjects, the expressions I do not know how to deal with and limitation suggest that the interaction with the patient is sometimes tense, particularly for fear of violence that threatens them as caregivers. In the psychosocial thoughts of nurses about their vulnerability are included various forms of violence used by patients, such as verbal, characterized by uttering offensive expressions derived from the state of revolt, and physically, against others or themselves that says about the attempt, threat or aggression itself to physical domains of the nurses’ body or themselves, including the suicide attempt. It is interesting to note that, regardless of how or to whom violence is directed, it affects nurses in different ways, causing them worry, fear, apprehension, anxiety and restlessness3, which contributes to the enhancement of their resignified vulnerability.
By combating violence mentioned by the subjects of this study, it is postulated that the psychic load and overload21 settle as factors that enhance the vulnerability of nurses in the everyday care for people with HIV / AIDS. It is clear, then, that in the context of hospital organization, the professional is a being who is vulnerable, as well as the patients who are care targets2. The psychosocial stressor agents that are explicit in the speech of the subjects are so powerful that they can be considered as factors that reveal the stressful nature of nursing work22-23.
Axis 2: empowerment settings in the interpersonal relations between nurses and HIV seropositive patients
As previousluy mentioned, the patient’s irritability constitutes as one of the threats felt by the nurses, whose mode of dealing with the patient modifies the condition of their mental state. There is a coping mechanism of the status of vulnerable regarding the management of violent situations based on reciprocity, where the patient's irritability is answered with the loss of patience, then verbalization of their state of stress.
Sometimes there comes a point that ends the professional’s patience that is being mistreated all the time. For better that he does, for more that they give themselves and works well! There comes to a point where the professional stresses with the patients for has being assaulted by them either verbally or with the same lack of manners. (E8)
The possibility or the concreteness of being disrespected, harassed or minimized, seems foment a particular form of coping among nurses, in their representational field, relocates them in a more favorable position, in other words, more empowered. This form of confrontation is the result of stress caused by the irritability of patients, in which they take a stronger position and try to impose more respect in their professional figure and practices.
Not that I think the person is there because they deserved it. But I am not sorry. If they don´t know how to impose their respect, they will not get it. (E27)
Among nursing assistants, another study24 found similar results. According to this study, the nursing assistants perceive themselves in verbal and/or physical situations committed by individuals under their care. The origin of violence in this case is attributed by assistants to patients who are revolted against their HIV seropositivity diagnosis.
Empathy is an ability that requires sensitivity, respect and appreciation of each other's feelings. To be able to practice empathy in nursing care for patients with HIV/AIDS, nurses must be receptive, aware of the perspective of the patient state of convalescence and hospitalization, as well as being sensitive to worries, anxieties, fears and insecurities that they and their family may present.
In parallel to this essentially negative framework, the empowerment, in the representations of the subject, also has a strong and positive affective dimension. They expressed feelings of personal satisfaction in the face of patient recovery.
They are always coming and going. I find so rewarding! For example, the other day I was taking my grandmother to the doctor. I was stopped in traffic when a man said bye to me. He was a patient from here. I think it is really cool! We are always meeting, because most patients live here in the community. And I like that part. (E5)
[...] I am very pleased when I see patients getting better, or when I see that I can pass a little more hope and encouragement to the patient. I feel accomplished by working with these types of patients. (E18)
The proximity of those involved in the care process inside and outside the hospital walls can result in personal and professional satisfaction, mainly by the clinical recovery of the patient under care. This recovery provides a resolutive insight within the character of nursing care, which motivates nurses to give continuity to their engaged professional activity by visualizing themselves able to perform1-4, actions restoring, transforming power or minimally comforting. Nurses regard the manifestation of patient trust placed in them, such as the presence of praise and appreciation of their practice, as well as empowerment factors, where its rewards correspond to the suffering experienced while administering care.
[...] it is very rewarding when the patient looks at you and says: Oh good! Today you are on duty! For me, it makes my day when they said that. It is a prize for me! Because I feel that at this time they are showing that they have confidence in me. (E11)
The respect and gratitude from the patients in representational constructs developed by the subjects arise as to make the feeling of love by nurses for working with HIV / AIDS reciprocal. Which, itself shows to be interesting for revealing that, despite the daily hostility faced, the love for their profession and for the activity of taking care of seropositive patients shows itself explicit in the discourse of the subjects stating that there is, in fact, a significant degree of empowerment that alternates to the difficulties that make them vulnerable in the work context3.
The presence of AIDS in the routine of nurses culminates on the observation of uncertainty and suffering, due to the fatal character of the syndrome and the feeling of punishment26,27. However, it is clear that the time factor has strong ability to harmonize interpersonal relationships between nurses and patients, especially for making the personal appreciation in working with seropositive patients comes up.
For me it is part of my routine [the work].I do not know if it's because I’ve work here for so long... I like it. Even though we have so much suffering, I like it. (E5)
[...] You put the love for the profession, the love for the human being above everything. Have the desire to help people, help minimize that suffering. It is putting love and humanization first. (E19)
The individual being cared for may present a more positive and calm attitude in face of their experiences with a seropositive status, disability or even imminence of death due to AIDS, among other things, the trust relationship with their caregivers. In what concerns the caregivers2,28, working in the AIDS field can be as a deliberate attitude, authentic and spontaneous. Otherwise, the connection between work and worker does not hold4. Feeling grateful, serving with love and feeling accomplished are some of the expressions used by nurses to express their level of satisfaction, despite the working conditions which they face. Such constructs are, possibly, come from the opportunity to help or to render more humane and comprehensive care, deeds belonging to the nature of the profession in their ontological foundations29-31.
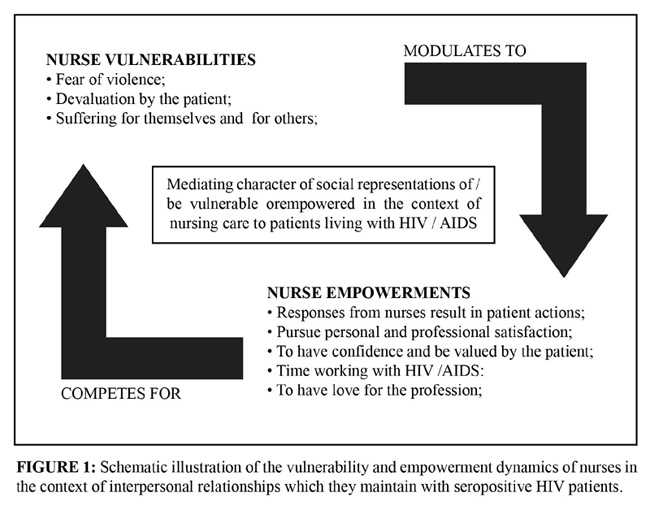
The content of social representations made by nurses about their vulnerability contribute to the setting of those who embody empowerment, and the latter, in turn, modulate the vulnerability for responding to the fragile factors (or potentially fragile) and for demanding from the subjects the reevaluation of the social thoughts above the initially constructed vulnerability. This movement is possibly, through the mediating role of social representations in the context of nursing care. From the results obtained in this study, it appears that the presence of vulnerability and empowerment in interpersonal relationships between nurses and patients, as well as its dynamics are illustrated as follows:
CONCLUSION
It was concluded that the set of representational vulnerability for nurses includes negative or dangerous elements such as fear, devaluation and suffering, the empowerment representational set changes to respond to the status of vulnerable and also to provide greater control for the subject or group on its state of vulnerability to encompass knowledge and protective practices in the context of social interactions with seropositive patients. In this sense, the personal and professional satisfaction with the work that was done, the fact of receiving confidence from patients on their care giving activities and their time of experience in the nurse activity with that type of patient means, for the subjects of this study, the largest state of empowerment.
The interpersonal relationships among nurses and patients, although show success in most cases, expose the professional at risk of recurrent maneuvers episodes, fruits of the expression of different forms of vulnerability. Under these evidences, it appears that, despite the constant initiative for approximation, diligence, dedication and love by the nurses - which is consistent with the ethical and aesthetic postulates of nursing - there is, at moments of violence, an apparent care nursing mischaracterization in their philosophical foundations, derived from the difficulties and challenges faced by nurses in their everyday institutional activities. On the other hand, from the everyday relationship with patients with HIV/AIDS, nurses can feel transformed as human beings perceiving themselves therefore potentialized, improved and/or satisfied with what they do and therefore more empowered. This situation, at certain times, can put nurses between suffering and pleasure.
Despite its limitations related to the small number of subjects in a single scenario, this study reached its proposed objective. In addition, it points out how future research may explore the presence of vulnerability and empowerment in other contexts and scenarios in terms of social thought, especially in the world of nursing as a caring profession.
REFERENCES
1. Berardinelli LMM, Santos I, Santos MLSC, Clos AC, Pedrosa GS, Chaves ACS. Cronicidade e vulnerabilidade em saúde de grupos populacionais: implicações para o cuidado. Rev enferm UERJ. 2010; 18:553-8.
2. Waldow VR, Borges RF. O processo de cuidar sob a perspectiva da vulnerabilidade. Rev Latino-Am Enfermagem. 2008; 16:765-71.
3. Gomes AMT. A vulnerabilidade como elemento organizador do cuidado de enfermagem no contexto do HIV/AIDS: conceitos, processos e representações sociais [tese de professor titular]. Rio de Janeiro: Universidade do Estado do Rio de Janeiro; 2011.
4. Santos EI. Vulnerabilidade de enfermeiros no cuidado a pacientes com HIV/AIDS: um estudo de representações sociais [dissertação de mestrado]. Rio de Janeiro: Universidade do Estado do Rio de Janeiro; 2012.
5. Mann JM, Tarantola DJM, Netter TW. Como avaliar a vulnerabilidade à infecção pelo HIV e AIDS. In: Parker R, Galvão J, Pedrosa JS, organizadores. A AIDS no mundo. Rio de Janeiro: Relumé Dumará; 1993. p. 275-300.
6. Sousa PKR, Miranda KCL, Franco AC. Vulnerabilidade: análise do conceito na prática clínica do enfermeiro em ambulatório de HIV/AIDS. Rev Bras Enferm. 2011; 64:381-4.
7. Santos TL, Abud ACF, Inagaki ADM. Vulnerabilidade às doenças sexualmente transmissíveis entre mulheres com alta escolaridade. Rev enferm UERJ. 2009; 17:502-5.
8. Mandú ENT, Antiqueira VMA, Lanza RAC. Mortalidade materna: implicações para o programa de saúde da família. Rev enferm UERJ. 2009; 17:278-84.
9. Silva KL, Dias FLA, Maia CC, Pereira DCR, Vieira NFC, Pinheiro PNC. A influência das crenças e valores culturais no comportamento sexual dos adolescentes do sexo masculino. Rev enferm UERJ. 2010; 18:247-52.
10. Souza JN, Bertolozzi MR. A vulnerabilidade à tuberculose em trabalhadores de enfermagem em um hospital universitário. Rev Latino-Am Enfermagem. 2007; 15:259-66.
11. Barboza MCN, Milbrath VM, Bielemann VM, Siqueira HCG. Doenças oesteomusculares relacionadas ao trabalho (DORT) e sua associação com a enfermagem ocupacional. Rev Gaúcha Enferm. 2008; 29:633-38.
12. Barra DCC, Lanzoni GMM, Maliska ICA, Sebold LF, Schlindwein BH. Processo de viver humano e a enfermagem sob a perspectiva da vulnerabilidade. Acta Paul Enferm. 2010; 23:831-6.
13. Moscovici S. A representação social da psicanálise. Rio de Janeiro: Zahar Editores; 1978.
14. Jodelet D. Folie et représesentations sociales. Paris (Fr): PUF; 1989.
15. Sá CP. A construção do objeto de pesquisa em representações sociais. Rio de Janeiro (RJ): EdUERJ; 1998.
16. Oliveira DC. A enfermagem e as necessidades humanas básicas: o saber/fazer a partir das representações sociais [tese de professor titular]. Rio de Janeiro: Universidade do Estado do Rio de janeiro; 2001.
17. Bardin L. Análise de conteúdo. Lisboa (Por): Edições 70; 2000.
18. Oliveira DC. Análise de conteúdo temático-categorial: uma proposta de sistematização. Rev enferm UERJ. 2008; 16:569-76.
19. Britto FVS. Representações sociais da prática do enfermeiro entre usuários do Programa Nacional de DST e AIDS [dissertação de mestrado]. Rio de Janeiro: Universidade do Estado do Rio de Janeiro; 2009.
20. Gomes AMT, Oliveira DC. A representação social da autonomia profissional do enfermeiro na saúde pública. Rev Bras Enferm. 2005; 58:393-8.
21. Lorenz VR, Benatti MCC, Sabino MO. Burnout e estresse em enfermeiros de um hospital universitário de alta complexidade. Rev Latino-Am Enfermagem. 2010; 18:1084-91.
22. Fonseca AM, Soares E. Desgaste emocional: depoimentos de enfermeiros que atuam em ambiente de hospital. Rev Rede Enferm Nordeste. 2006; 7:91-7.
23. Stacciarini JMR, Tróccoli BT. The stress in nursing profession. Rev Latino-Am Enfermagem. 2001; 9:17-25.
24. Formozo GA, Oliveira DC. Representações sociais do cuidado prestado aos pacientes soropositivos ao HIV. Rev Bras Enferm. 2010; 63:230-7.
25. Takaki MH, Sant’ana DMG. A empatia como essência no cuidado prestado ao cliente pela equipe de enfermagem de uma unidade básica de saúde. Cogitare Enferm. 2004; 9:79-83.
26. Tura LFR. AIDS e estudantes:a estrutura das representações sociais. In: Jodelet D, organizadora. AIDS e representações sociais: à busca de sentidos. Natal (RN): EdUFRN; 1998. p. 159-85.
27. Gomes AMT, Barbosa BFS, Oliveira DC, Wolter RMCP, Silva MVG. As representações sociais de enfermeiros sobre a criança soropositiva para HIV: interface com o cuidar. Rev enferm UERJ. 2011; 19:14-19.
28. Pinheiro PNC, Vieira NFC, Pereira MLD, Barroso MGT. O cuidado humano: reflexão ética acerca dos portadores do HIV/AIDS. Rev Latino-Am Enfermagem. 2005; 13:569-75.
29. Santos ÉI, Gomes AMT, Oliveira DC, Valois BRG, Braga RMO. Comprehensiveness in nurse’s care practice in primary health care context. Rev enferm UFPE on line. 2011; 5:1054-63.
30. Santos ÉI, Gomes AMT, Oliveira DC, Santo CCE, Felipe ICV, Lima RS. O princípio da integralidade no contexto do HIV/AIDS: uma revisão integrativa. Rev Pesq Cuidado é Fundamental Online. 2010; 2:1387-98.
31. Gomes AMT, Oliveira DC, Santos ÉI, Santo CCE, Valois BRG, Pontes APM. As facetas do convívio com o HIV: Formas de relações sociais e representações sociais da AIDS para pessoas soropositivas hospitalizadas. Esc Anna Nery. 2012; 16:111-20.
Received: 04.10.2012