RESEARCH ARTICLES
Long term home oxygen therapy: users' profile and costs
Cristina Shizue WatanabeI; Leonardo Francisco Campos de AndradeII; Manoel Quintino da Silva NetoIII; Silvia de Fátima Tamini dos SantosIV; Lauren Suemi KawataV
I
Graduated in Nursing from Barão de Mauá University Center. Ribeirão Preto, São Paulo, Brazil. Email: cristinashizuewatanabe@hotmail.com
II
Graduated in Nursing from Barão de Mauá University Center. Ribeirão Preto, São Paulo, Brazil. Email: leonardoandradeef@hotmail.com
III
Graduated in Nursing from Barão de Mauá University Center. Ribeirão Preto, São Paulo, Brazil. Email: mqsneto@hotmail.com
IV
Graduated in Nursing from Barão de Mauá University Center. Ribeirão Preto, São Paulo, Brazil. Email: tamini.silvia@gmail.com
V
Nurse. PhD in Sciences. Full Professor I in the Undergraduate Nursing Course at Barão de Mauá University Center. Nurse for City Hall of Ribeirão Preto. São
Paulo, Brazil. Email: lsuemi@hotmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2015.7117
ABSTRACT
Exploratory-descriptive, quantitative study aiming at identifying and analyzing the profile of users of long term home oxygen therapy (HOT), as well as identifying the monthly cost of the HOT for the city. Secondary data were obtained from medical records, in July, 2012. The population consisted of 40 users registered in HOT North Home Care in Ribeirão Preto, São Paulo, Brazil. Among the users, 67.5% were female; 30% were smokers; 67.5% were 60 years or older; 62.5% had chronic obstructive pulmonary disease; 75% showed improvement in oxygen saturation levels after initiation of HOT; 87.5% used nasal catheter, and 50% used concentrator as a source. Monthly cost was R$19,410.00. Conclusions show that users' profile mirrors the ageing of the population and the prevalence of chronic diseases related to lifestyle. Keywords: Oxygen inhalation therapy; home nursing; health profile; costs and costs analysis.
INTRODUCTION
Home care, which is subsidized by the Unified Health System (SUS, as per its acronym in Portuguese), was established to decrease hospital bed occupancy and high hospitalization costs, reduce risks of infection and improve quality of life for patients who, despite being discharged, require intensive care and technological resources1. Home care also allows social interaction with family members, and their participation contributes to patients' improvement and resumption of daily activities1. Long-term home oxygen therapy has been used within the context of home care.
The provision of home oxygen therapy is a health service that should be organized and offered by cities. It should be emphasized that the provision of effective services that meet the needs of users is the duty of the government, justified on the basis of human dignity2. The obligation to provide such services is based on the principles of comprehensiveness of health care and resolution of medical problems. In order to effectively set up services that enable these principles to be implemented, it is necessary to identify the profile of home oxygen therapy users.
Since it is the responsibility of cities to provide this therapy, it is necessary to collect cost information. Cost management is an essential component of information systems, since it can help supply administrators with better information for decision making. It is useful for any kind of organization and provides a more accurate view of reality, since it allows examination of how available funds are spent3.
In light of the above, this study asked: What is the profile of home oxygen therapy users in the North District of Ribeirão Preto? What is the monthly cost to the city? The objective of the present study was to identify and analyze the profile of home oxygen therapy users, showing the monthly cost of home oxygen therapy to the city of Ribeirão Preto, São Paulo, Brazil.
LITERATURE REVIEW
Home oxygen therapy requires symptoms that include partial pressure of oxygen in arterial blood (PaO2) ≤ 55 mmHg or arterial oxygen saturation (SaO2) of 88% or less, at rest or exercising4.
This therapy is a costly procedure and selection of patients for treatment must be extremely rigorous and abide by international recommendations. The prescription for using it needs to be very detailed in terms of oxygen source, delivery method, duration of use and flow5. It is considered the main non-pharmacological treatment for patients with chronic obstructive pulmonary disease (COPD) and chronic hypoxemia. Its primary objectives are: reversal of hypoxemic changes, maintenance of hemoglobin, cardiac output and adequate tissue perfusion6.
Using home oxygen therapy for at least 15 hours a day has a positive impact, with benefits in the following areas: pulmonary hemodynamics, hematologic parameters, exercise capacity, lung mechanics and mental state. It is one of the few therapies that change the prognosis for patients, since it reverses secondary polycythemia, hypoxemia, pulmonary arterial hypertension, possible cardiac arrhythmias and dyspnea, in addition to improving neuromuscular and neuropsychic function and boosting physical endurance5-7.
A number of studies have found other benefits: satisfactory evolution of most patients receiving home oxygen therapy8; decreased use of emergency services by hypoxemic patients after starting therapy9; and improved quality of life for patients with COPD and chronic hypoxemia 10.
Home oxygen therapy has been studied in populations of different ages. A study with children11 showed that the underlying diseases that lead to the use of home oxygen therapy are: cystic fibrosis, bronchopulmonary dysplasia, obliterative bronchiolitis, neurodeficiencies and secondary pulmonary hypertension. As for adults, one study12 showed the main underlying diseases to be pulmonary emphysema, hypoxemia, bronchitis, and pulmonary fibrosis, among others. Another study cited13 COPD and hypoxemia. With respect to home oxygen therapy in different age groups, it should also be noted that children have relevant particularities. This makes it necessary to take into account things such as physical growth and neurological development, as well as the need for adult supervision and the supply of home oxygen therapy in schools14.
Lastly, the literature points to the low number of studies on the subject of home oxygen therapy5-10,12-15. The aspects most addressed are those related to the underlying disease (which lead the patients to receive such treatment) and the importance of using strict criteria for its prescription. Studies on the use of home oxygen therapy have been conducted in different regions of Brazil and the world, showing that information and experience on the subject are being collected and disseminated.
METHODOLOGY
This was a document-based, descriptive, exploratory, quantitative study that took place in Ribeirão Preto, a city located in the northeast of the State of São Paulo, Brazil, 313km from the capital, with a population of 612,339 inhabitants16.
Ribeirão Preto is characterized as a regional health care hub with 15 hospitals. The municipal health care network is divided into five districts (east, west, north, south and central), each containing basic health units with 24-hour service. There are 46 basic health units, with 21 family health teams 17. The city also provides home care services, officially implemented in 1996.
The goal of home care service is to train professionals who provide home care, establish criteria for inclusion and discharge of home care patients, decrease the length of hospital stays and readmissions, optimize beds and reduce costs, assist and support families, promote the development of family responsibility, and implement home care actions aimed at improving quality of life16. Home care utilizes multidisciplinary teams consisting of one nurse coordinator, three nurses, two nursing technicians and ten nursing assistants, four nursing interns, a physiotherapist, three doctors, a dentist, seven nursing graduates in training, two administrative assistants and eight drivers. There is a home care service team for each district; the team follows up on patients receiving home oxygen therapy18.
The researchers conducted this study in the North Home Care Service, since this is the district that engages in administrative activities and provides services for the institution.
Data collection was carried out in July 2012; secondary data was used, obtained from the medical records of home oxygen therapy users filed at the home care service headquarters. A collection instrument was prepared containing the following variables: date of birth; gender; age at the time home oxygen therapy was started; presence or absence of health insurance; underlying diseases; smoking; oxygen saturation (PaO2) at the start of and during home oxygen therapy; type or source of oxygen support (O2); and length of time of use. The data was entered into an Excel database.
On the basis of the medical records examined, the target population was composed of the 40 registered home oxygen therapy users in the home care service of the North District, without exclusions.
The study complied with the regulations of the National Research Ethics Commission (CONEP), expressed in Resolution No. 196 of the National Health Council (CNS). The research project was submitted to the Ethics Committee for Research of Barão de Mauá University Center, through the Brazil Platform, and was approved under Protocol No. 33992.
Descriptive statistics were used for the presentation and analysis of data related to the profile of home oxygen therapy users.
With regard to costs, for cylinder users, the total number of liters of O2 consumed per month was calculated for each patient, using the formula: total liters/month = (n x 60) x h x 30, where n = the number of liters/minute of O2 and h = the amount of O2 used per hour. From there, the number of cylinders used in a month was calculated. That number was then multiplied by the cost of the cylinders. For concentrator users, the monthly rental cost of the devices was calculated. For mixed source users (cylinders and concentrators), the two calculations described above were performed.
RESULTS AND DISCUSSION
In the age analysis of the 40 home oxygen therapy users registered in the home care service of the North District, there was a range from 3 to 91 years of age (mean: 61.4, median: 64, standard deviation: 20.1): 3 (7.5%) were from 3 to 19 years of age and 27 (67.5%) were 60 or over. This data corroborates another study, which found that it is mostly older people who use home oxygen therapy2. It should be noted that with progression of age, some physiological changes become more apparent and the functional capacity of elderly people can be or become affected, requiring constant care19.
It was also observed that 10 (25%) users were from 20 to 59 years old, representing a population that would be expected to be economically active. The use of home oxygen therapy limits the performance of certain professional activities and can generate loss of productivity, thus indicating that the impact of chronic conditions extends far beyond health-related costs20.
In relation to gender, 27 (67.5%) users were female and 13 (32.5%) were male. When observing the predominant age range and gender, a relationship can be established with life expectancy in the Brazilian population. According to a study conducted on the life expectancy of Brazilians, women live an average of 77.32 years and men, 69.73 years21. Given that older people were the group that stood out among home oxygen therapy users, it can be expected that a higher percentage of women will be using this therapy, since life expectancy for women is higher than for men.
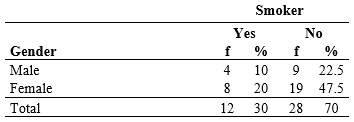
With respect to the use of tobacco, 12 (30%) of the users were smokers, according to Table 1. Of the total number of non-smokers, 14 (40%) had been smokers at some time in their lives. It is important to note that smoking constitutes a health threat and its negative consequences have been recognized for over four decades20. In addition, a study carried out in the United States demonstrated the continual problem of burns secondary to smoking among home oxygen therapy users22.
Table 1: Distribution of home oxygen therapy users registered with the home care service in the North District of Ribeirão Preto, according to gender and tobacco use. Ribeirão Preto, São Paulo, July 2012.
When analyzing gender and tobacco use, it was noted that the data found and presented in Table 1 differs from the results of a survey on smoking in Brazil 23, which showed that from 2002 to 2009 men were predominant among smokers in each region of the country. It is therefore important for professionals to develop actions (surveys, prevention and health promotion) raising awareness among smokers about seeking smoking cessation therapies 24.
In terms of health care services, 8 (20%) users had health insurance plans. This data shows that, although some home oxygen therapy users have health insurance plans, such plans do not always ensure the provision of therapy, making the city responsible for ensuring its provision. This is because the plans shift patients to the SUS for home oxygen therapy after they are discharged from the hospital in order to reduce expenses. The percentage of home oxygen therapy users with health insurance plans in the district may differ substantially from other health districts, since the North District covers an area with a population that has a low socioeconomic level and Supplementary Health System coverage varies according to household income class: [...] In the class of less than 1 monthly minimum wage, coverage is 2.9%; in the class of 1-2 minimum wages, 6.7%; in the class of 2-3 minimum wages, 14.1%; in the class of 3-5 minimum wages, 24.9%; in the class of 5-10 minimum wages, 43.5%; in the class of 10-20 minimum wages, 65.8%; and in the class of more than 20 minimum wages, 83.9% 25:54.
When observing the clinical profile of the users, it was found that 25 (62.5%) had COPD as the underlying pathology, corroborating another study which also identified this disease as the primary reason for home oxygen therapy13.
Therefore, as mentioned earlier, home oxygen therapy is currently the main non-pharmacological treatment for patients with COPD and chronic hypoxemia 6. One study on quality of life of patients with chronic obstructive airway disease concluded that such users experience impaired quality of life that can be improved through regular use of home oxygen therapy10.
Also in relation to the total of 25 (100%) home oxygen therapy users with COPD, it was found that 10 (40%) were smokers, even while using the therapy, and 11 (44%) had used tobacco at some point in their life. From these results, it is clear that smoking, the leading cause of COPD, has a multi-factor impact on society, especially as measured by high mortality rate.
When analyzing the length of time the person had the disease, it ranged from 2 months to 31 years. The majority, 22 (55%), reported that they had first been diagnosed within the last 10 years, as can be seen in Table 2.
Table 2: Distribution of home oxygen therapy users registered with the home care service in the North District of Ribeirão Preto, according to length of time of disease. Ribeirão Preto, São Paulo, 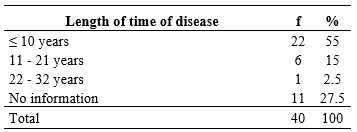
No articles were found that discussed the variable involving length of time the person had the disease, which may be related to the fact that this aspect is individualized, according to biotype, clinical status and severity of the disease.
In a detailed analysis of length of time of the disease, it was noted that although COPD was the most common pathology, it had been diagnosed, on average, within the last eight years. It is worth noting that patients who had had the disease for a longer period of time were those who had came down with bronchial asthma (20 years) and cystic fibrosis (31 years).
In 11 (27.5%) medical records, there was no information on length of time of the disease, which shows the need to determine the causes of the absence of such data, which helps identify the history and clinical status of users.
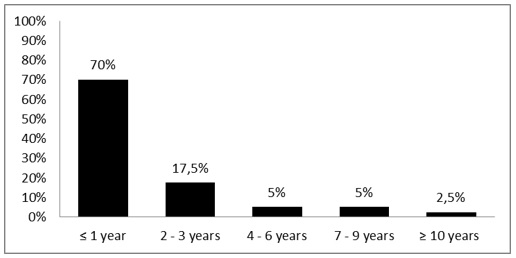
Length of time of home oxygen therapy use ranged from 2 months to 22 years (with a mean of 2.34 years and a median of 1.1 years). The results indicated that, last year, there was a major increase in home oxygen therapy use in the population studied, since 28 (70%) registered users had been using home oxygen therapy for one year or less. It is interesting that 7 (17.5%) users had been using home oxygen therapy for two or three years, as shown in Figure 1, which may indicate increased access to the therapy.
When observing the initial saturation level in the treatment, most users (30, or 75%) had saturation lower than 88%, which justified the need for home oxygen therapy. During treatment, 22 (55%) patients had saturation ≥ 90%, which demonstrated the effectiveness of oxygen therapy. This data further supported another study5 that stated that home oxygen therapy treatment is expected to obtain a flow of oxygen greater than or equal to 90% in patients with chronic hypoxemia5.
In terms of PaO2 results, 25 (62.5%) users had PaO2 ≤ 55 mmHg, showing that the PaO2 values serving as indicators for starting home oxygen therapy coincided with those reported in the literature: patients who should use home oxygen therapy are those with PaO2 <55 mmHg or SaO2 <88% with or without hypercapnia26. Heat treatment may be prescribed for those with PaO2 from 55 mmHg to 60 mmHg or SaO2 of 88%, if there is evidence of pulmonary arterial hypertension, peripheral edema suggestive of congestive heart failure or polycythemia5.
As for the O2 source, 3 (7.5%) patients used a mixed source, 17 (42.5%) used cylinders and 20 (50%) used concentrators. This data may be connected to cost, since some researchers have mentioned that cylinders empty quickly and need to be constantly replaced, which increases the cost of the therapy, unlike concentrators that use ambient air in order to capture O2 5. Another factor that determines the source is family income and household structure, since concentrators require electricity consumption. Furthermore, in places where constant power outages occur, home oxygen therapy users must have cylinders in their homes27.
Regarding the route of administration of O2 , 35 (87.5%) patients used nasal catheters and 5 (12.5%) used other routes, such as face masks or tracheal masks. Each type of route of administration was prescribed according to the degree of impairment of the patient's respiratory system. Another study also revealed that most patients used catheters as the route of administration, indicating that they did not require large amounts of O2 , because O2 catheters support a maximum flow of 6 liters/minute4.
Concerning O2 flow, the O2 dose administered must be prescribed individually, according to the flow needed to obtain a PaO2 value of at least 60 mmHg and SaO2 greater than 90%, with the patient at rest28. In this study, 18 (45%) maintained the O2 flow (remaining clinically stable, without improvement), 13 (32.5%) required increased O2 flow (indicating deterioration in clinical status) and 9 (22.5%) reduced the O2 flow.
The analysis of the clinical profile of the home oxygen therapy users showed that they were within the home oxygen therapy inclusion criteria of the home care service and conformed to the standards established in literature reviews26-28.
As for determining home oxygen therapy treatment costs, at the time of the study the supplier was charging R$110 per 10-cubic-meter cylinder (10m3), which is the size used in home oxygen therapy in the city, and R$160 for the monthly rental of a concentrator.
It was found that 20 (50%) home oxygen therapy patients used a concentrator. Multiplying total concentrator users (20) by the monthly rental price of the device (R$160), the overall cost was R$3,200.
In terms of O2 source, it was observed that 17 (42.5%) patients used only cylinders. The formula set forth in the methodology section to calculate the total number of liters of O2 consumed in a month was used for each patient.
The 17 (42.5%) cylinder users consumed a total of 140,000 liters of O2 per month. This amount, divided by 10,000 (equivalent to a 10m3 cylinder), resulted in a total of 140 10m3 cylinders per month. Multiplying the number of cylinders (140) by the cost of each 10 m3 cylinder yielded a cost of R$15,400.
The research revealed that 3 (7.5%) patients used mixed sources of O2 , i.e., concentrators and cylinders. Multiplying 3 (number of users) by R$160 (monthly rental price of the concentrator), came to a cost of R$480. For these users a calculation was performed, multiplying R$110 (price of a cylinder) by 3 (number of users), amounting to a cost of R$330. It was not possible to obtain information on the way in which patients used mixed sources, so it was therefore considered that these users were supplied with at least one cylinder/month. Adding together the cost of the cylinders (R$330) and concentrators (R$480), the total cost for mixed source home oxygen therapy users was R$810.
These costs showed that, in the context of this research, cylinders were more expensive than concentrators, which corroborated another study in which cylinders had a higher cost than concentrators21. Note that electricity costs for the use of concentrators were not calculated.
Adding together all the above expenses (R$3,200 + R$15,400 + R$810), the city spent a total of R$19,410 on home oxygen therapy in the month under study.
When calculating the total days that home oxygen therapy users received home care, it can be inferred that 34,283 days of hospitalization were avoided. It was not possible to obtain the cost of a one-day stay in the hospital, since this calculation depends on a variety of factors (resources provided, such as food, multidisciplinary team, etc.).
In a study involving 40 children receiving home oxygen therapy, the authors reported that if these users had stayed in the hospital, the estimated cost of their 16,984 days of hospitalization for the health care system would have been approximately R$186,824. In that study, a cost calculation was performed, based on R$11 per day in the hospital8. Using the same figure in this study to obtain avoided hospitalization costs, an expense of R$377,113 (multiplying R$11 by 34,283 days) would be avoided through providing home oxygen therapy in patients' homes. The actual cost is undoubtedly much higher, since the above study was published in 20018.
It is important to consider here a limitation of this study; it was not possible to determine the cost of a one-day stay in the hospital, because it varies according to many factors (sector, materials, and route of administration, among others).
As mentioned earlier, cylinders were responsible for 15,400 (79%) of the costs linked to the therapy, showing that it is more costly in the North District. Replacing cylinders with concentrators would significantly reduce costs for the city. On the other hand, social issues related to users must be analyzed before considering the possibility of making this change, due to the high electricity consumption generated by concentrators.
CONCLUSION
The results of this study reflect the reality of a specific region of the city, providing knowledge of a local context that may help managers and workers to develop actions in their day-to-day work.
The profile of users (prevalence of older people with chronic diseases who have used tobacco at some point in their lives) depicts a situation experienced in Brazil and the world: demographic transitions and changes in morbidity profile, i.e., population aging and prevalence of lifestyle-related chronic diseases, generating demand for long-term treatments. As noted previously, the clinical profile of users conforms to the parameters of the home care service and the literature for prescribing home oxygen therapy.
Finally, when considering the costs and number of days of hospitalization avoided by using home oxygen therapy in home care services, it can be concluded that implementing this therapy would help reduce the problems faced by the system in regulating hospital beds, thus underscoring the importance of home care services within the SUS network in Ribeirão Preto.
REFERENCES
1.Ministério da Saúde (Br). Lei nº 10.424 de 15 de abril de 2002. Dispõe sobre as condições para a promoção, proteção e recuperação da saúde [...] regulamentando a assistência domiciliar no Sistema Único de Saúde. [cited on Apr 14, 2014]. Available at: http://www.objnursing.uff.br/index.php/nursing/article/view/738/168
2.Oliveira LM. Responsabilidade municipal pela prestação do serviço de oxigenoterapia domiciliar e seus contornos. Rev Direito Sanitário. 2009; 10(1): 39-50.
3.Almeida AG, Borba JA, Flores LCS. A utilização das informações de custos na gestão da saúde pública: um estudo preliminar em secretarias municipais de saúde do Estado de Santa Catarina. Rev Administração Pública. 2009; 4: 579-607.
4.Perry A. Oxigenação. In: Potter PA, Perry A. Fundamentos de enfermagem. Rio de Janeiro: Elsevier; 2009. p.907-65.
5.Bartholo TP, Gomes MM, Noronha Filho JA. DPOC: o impacto da oxigenoterapia domiciliar no tratamento. Pulmão RJ - Atualizações Temáticas. 2009; 1 (1): 79-84.
6.Viegas CAA, Adde FV, Paschoal IA, Godoy I, Machado MCLO. Oxigenoterapia domiciliar prolongada (ODP). J bras pneumol. 2000; 26: 341-50.
7.Alves MV, Godoy I, Luppi CH. Levantamento das características dos pacientes atendidos no serviço de oxigenoterapia da Faculdade de Medicina de Botucatu-UNESP. Rev Ciên Ext. 2004; 1 (1): 53-4.
8.Mocelin HT, Fisher GB, Ranzi LC, Rosa RD, Philomena MR. Oxigenoterapia domiciliar em crianças: relato de sete anos de experiência. J bras pneumol. 2001; 27: 148-52.
9.Munhoz AS, Adde FV, Nakaie CMA, Doria Filho U, Silva Filho LVRF, Rodrigues JC. Oxigenoterapia domiciliar prolongada em crianças e adolescentes: uma análise do uso clínico e de custos de um programa assistencial. J Pediatr. 2011; 87 (1): 13-8.
10.Tanni ES, Vale SA, Lopes PS, Guiotoko MM, Godoy I, Godoy I. Influência do sistema de fornecimento de oxigênio na qualidade de vida de pacientes com hipoxemia crônica. J bras pneumol. 2007; 33: 161-7.
11.Balfour-Lynn IM. Oxigenoterapia domiciliar prolongada: uma perspectiva britânica. J Pediatr. 2011; 87 (1): 1-3.
12.Baldi BG, Pereira CAC, Rubin AS, Santana, ANC, Costa AN, Carvalho, CRR et al. Destaques das Diretrizes de Doenças Pulmonares Intersticiais da Sociedade Brasileira de Pneumologia e Tisiologia. J bras pneumol. 2012; 38: 282-91.
13.Nocturnal Oxygen Therapy Trial Group. Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease: a clinical trial. Annals of Internal Medicine. 1980; 93: 391-8.
14.Adde FV, Alvarez AE, Barbisan BN, Guimaraes BR. Recommendations for long-term home oxygen therapy in children and adolescents. J Pediatr. 2013;89(1):6−17
15. Comité Nacional de Neumonología. Guías para el manejo de la oxigenoterapia domiciliaria en pediatría. Arch Argent Pediatr. 2013;111:448-54.
16.Instituto Brasileiro de Geografia e Estatística. IBGE. Estimativa populacional 2011. [cited on Apr 14, 2014]. Available at: http://ibge.gov.br//.
17.Ribeirão Preto (SP). Secretaria Municipal da Saúde. Divisão de Planejamento em Saúde. Plano Municipal de Saúde 2010-2013. Ribeirão Preto (SP): Secretaria Municipal da Saúde; 2009.
18.Ribeirão Preto (SP). Secretaria Municipal da Saúde. Protocolo de atendimento em oxigenoterapia domiciliar prolongada (ODP). Ribeirão Preto (SP): Secretaria Municipal da Saúde; 2007.
19.Martins JJ, Nascimento ERP, Erdmann AL, Candemil MC, Belaver GM. O cuidado no contexto domiciliar: o discurso de idosos/familiares e profissionais. Rev enferm UERJ. 2009; 17:556-62.
20.Organização Mundial da Saúde. Cuidados inovadores para condições crônicas de saúde: componentes estruturais de ação: relatório mundial. Brasília (DF): Organização Mundial da Saúde; 2003.
21.Instituto Brasileiro de Geografia e Estatística. Tabuas completas de mortalidade 2010. [cited on Apr 14, 2014]. Available at http://www.ibge.gov.br
22 Al Kassis S, Savetamal A, Assi R, Crombie RE, Ali R; Moores C, Najjar A, Hansen T, Ku T, Schulz JT. Characteristics of patients with injury secondary to smoking on home oxygen therapy transferred intubated to a burn center. J Am Coll Surg . 2014; 218:1182-6.
23.Ministério da Saúde (Br). Instituto Nacional de Câncer INCA. A situação do tabagismo no Brasil: dados do inquérito do sistema internacional de Vigilância, da Organização Mundial da Saúde, realizado no Brasil, entre 2002 e 2009. Rio de Janeiro: INCA; 2011.
24.Scherer EA, Scherer ZAP. Opinião de pacientes, familiares e profissionais sobre o hábito de fumar em uma enfermaria psiquiátrica. Rev enferm UERJ. 2014; 22:376-82.
25.Conselho Nacional de Secretários da Saúde. SUS: avanços e desafios. Brasília (DF): CONASS; 2006.
26.Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Global Initiative for Chronic Obstructive Lung Disease (GOLD), executive summary, 2006. [cited on Apr 14, 2014]. Available at: http//goldcopd.com
27.Sato K, Morita R, Tsukamoto K, Sato N, Sasaki Y, Asano M, Okuda Y, Miura H, Sano M; Kosaka T, Watanabe H, Shioya T, Ito H. Questionnaire survey on the continuity of home oxygen therapy after a disaster with power outages. Respir Investig. 2013; 51(1):9-16.
28.Cedano S, Belasco AGS, Traldi F, Machado MCLO, Bettencourt ARC. Influência das características sociodemográficas e clínicas e do nível de dependência na qualidade de vida de pacientes com DPOC em oxigenoterapia domiciliar prolongada. J bras pneumol. 2012; 38: 331-8.