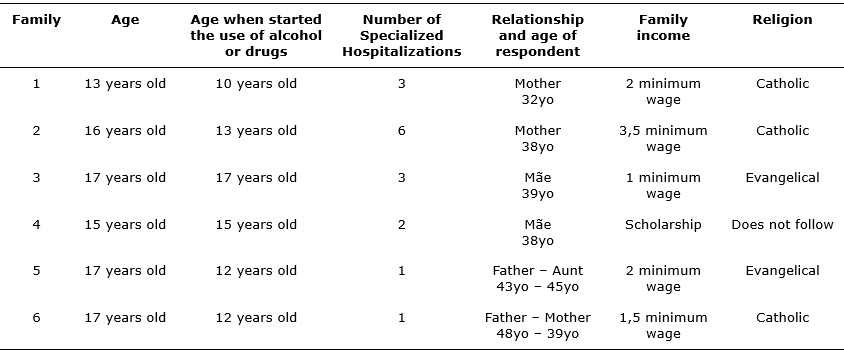
FIGURE 1: Characteristics of teenagers users of alcohol and psychoactive substances and their main caregivers admitted to psychiatric referral hospital. Paraná, 2008.
ORIGINAL RESEARCH
Teenage drug users' care needs according to their relatives
Adriano BrischiliariI; Sheila Cristina Rocha-BrischiliariII; Sonia Silva MarconIII
I
Nurse. Doctorate Student. Post Graduate Program in Nursing, Universidade
Estadual de Maringá. Nurse at UPA Zona Sul, Town Hall of Maringá. Maringá,
Paraná, Brasil. E-mail:
adriano.enfermeiro@hotmail.com
II
Nurse. Doctorate Student. Health Sciences. Universidade Estadual de
Maringá. Professor, Nursing School, Universidade Estadual do Oeste do
Paraná. Foz do Iguaçu, Paraná, Brasil. E-mail:
sheila.brischiliari@gmail.com
III
Nurse. Doctor. Professor, Post Graduate Program in Nursing Master/Doctorate
in Nursing at Universidade Estadual de Maringá. Maringá, Paraná, Brasil.
E-mail: ssmarcon@uem.br
DOI: http://dx.doi.org/10.12957/reuerj.2016.6888
ABSTRACT
Objective: to understand the care needs teenage alcohol and psychoactive substance users, as expressed by relatives. Method: this descriptive, qualitative study of six relatives of teenage alcohol and other drug users, who had been hospitalized for treatment in northwest Paraná State. Data were collected from March to June 2009 by open interview and then subjected to content analysis. Results: show that suffering is intense and calls for monitoring of family conflicts. The family perceive professionals' carelessness with the teenagers, characterized by a lack of continuity in care, lack of encouragement and information needed for family members to understand situations arising from drug use and how to deal with them better. Conclusion: there is an urgent need for professionals to support families, offering effective guidance and monitoring of both teenagers and family.
Keyword: Family relations; nursing; mental health; substance-related disorders.
INTRODUCTION
Adolescence is a stage of life characterized by important biological, cognitive, emotional and social changes1, in which the individual intensively search his/her universe of trials and own identity2.
The increase in the consumption of licit and illicit drugs by children and adolescents is concern in contemporary society3, because it has consequences and/or anticipated losses in life2. The main reasons for the use of psychoactive substances at this stage of life are personal problems, need for social appreciation, curiosity/experimentation, pursuit of pleasure, stress relaxation and idleness4.
Other factors are the conflicts between parents and children, and the fact that the person become part of the social group as a way of personal identification6 and even as a search for group approval, mutual trust and, above all, increased self esteem7.
The consumption of psychoactive substances by children and adolescents is a serious public health problem5. A study conducted in southern Brazil found a high prevalence of drug experimentation among adolescents, especially alcohol, in which 60.7% had used at least once in their lifetime and 33% in the last 30 days8. This way, great efforts should be made in search of knowledge about this phenomenon3 although teenagers related studies are scarce in low and middle rincome9, and that involve the families of the interface of drug use10 in this population.
Given the above, the following question came up: How the family has lived with the adolescent user of alcohol and psychoactive substance and what are his/her needs? That way, it was defined as the objective of the study to understand the need for care expressed by relatives of adolescent alcohol and psychoactive substances users.
LITERATURE REVIEW
The concern with the increase in the prevalence of drug use among young people and adults led the Brazilian government to make specific laws to guide, integrate and coordinate actions in the prevention and treatment of these substance users11-16.
Regarding the approach to the drug issue, there are several theoretical perspectives, advocating different ways to deal with the issue, some more restrictive, such as in North America, other more permissive, as European, however the National Policy Anti Drugs (PNAD) focus enforcement actions, and treatment and prevention actions17 but do not deepen the vision nor the family of teenage drug user care needs.
Although the teen's attention is directed out of the home and focused on groups of colleagues and friends, to understand it, it is necessary to insert him/her in the family and socio-cultural context, because the family - nuclear and extended - integrated to the culture is the one which provides the basis for his/her development18.
METHOD
Descriptive qualitative study conducted with families of six teenage users of alcohol and other drugs who were hospitalized in a psychiatric referral hospital for the treatment of male adolescents from all over the state of Paraná. Of the 252 beds, 12 are intended for these cases, with structure and specific therapeutic designed for this purpose.
Randomly, it was selected as relatives interviewed, people over 18, who lived with the teenager in the city of Maringa, and who visited them during the stipulated period for the initial contact and invitation to participate in the study. The interviews, previously scheduled, were carried out from March to June 2009, in their homes, with the consent of family members. Had an average duration of 90 minutes, and were recorded.
The collected data were fully transcribed and subjected to content analysis thematic modality, which is given in three steps - pre-analysis, exploration and data processing19.
In the first, the pre-analysis, there were made three successive readings of the interviews, occasion in which the points of interest were underlined, data organized according to the objectives of the study and the initial coding was performed. In the second stage, called the exploration, categorizing was done, organizing the data into groups in order to guarantee associations to respond to the objective of the study, resulting in one category and two subcategories. In the third and final stage was held thematic content analysis itself, characterized by inference on data19, relating them with the literature.
Ethical standards were met in research involving human beings20, and the project was approved by the Ethics Committee of the signatory institution (CAAE no. 621/2008). All participants signed a free and informed consent. To protect their identity was used a code by order of the interviews of family (F1, F2..., F6).
RESULTS AND DISCUSSION
Presenting the families
Studied family were in most were separated mothers, with more than one child, low education, Catholic, employees and users of the Unified Health System (SUS). Adolescents were between 13 to 17 years old. All began using drugs early, before the age of fourteen were using alcohol and crack and did not go to school, as shown in Figure 1.
FIGURE 1:
Characteristics of teenagers users of alcohol and psychoactive substances
and their main caregivers admitted to psychiatric referral hospital.
Paraná, 2008.
Adolescents who start early consumption of psychoactive substances tend to have higher levels of problems related to use and are more likely to develop psychiatric disorders, however, the search for treatment for addiction is not characteristic of this age21. Low education is a common characteristic among adolescents drug addicts/users and may limit individual development opportunities with repercussions throughout life22.
While in the hospital under study are met only male adolescents, it is important that sex ends up being a socio-demographic variable often associated with the use of alcohol and drugs among adolescents5, and consumption tends to be more frequent among male teenagers23,24.
Although very young, the number of admissions shows several relapses in this type of treatment leading us to some questions: is the form of treatment that is not the most appropriate? The social reintegration program is not happening in a way to support the needs of these adolescents and their families?
Relapse is the act of using alcohol or drugs after considerable periods of abstinence23. Recurrence may result from the fact that chemical dependence is strongly influenced by the lack of family and social support. However, relapse is usually preceded by symptoms, which if detected in time, can contribute to the return to the recovery process, where the individual is strengthened through learning25.
Social support can help reduce clashes and improve interpersonal interaction of users and society. This can help maintain abstinence, to take a new social role, and also to respect the society. This concept approaches the idea of psychosocial rehabilitation as promoting autonomy and social reinsertion of individuals26.
Another aspect relates to the assistance of service to families, for not knowing how to deal with this situation, they get sick with their teens, making the living unbearable. This way, the higher the support that the drug user can gather, the greater the chance of maintaining abstinence and also modify their behavior27.
Care needs expressed by the family
Out of this category emerged subcategories- the usual complaints from family and shortcomings of integrate- care analyzed below.
The usual complaints of family
The families expressed their needs in relation to health services and professionals, declaring abandonment situations at certain times, or times when they felt abandoned by the health service and also by the Guardian Council. Also reported moments of neglect, in which they were not heard, nor supported or assisted. In this sense, the main complaints of the family referred to the lack of proper care to their needs, including guidance, monitoring, appreciation, respect, understanding, involvement, among others. Study shows unsteadiness between demand and care provided, since disarticulated interventions are performed without intersectoral projects, and without the necessary coordination of integral care network28.
The progressive marginalization, resulting from drug use, stigma of society in relation to the user, determined as character deviation or lack of shame and prejudice make the family feel guilty and ashamed to have someone in this situation29. That way, when one is immersed in this reality, he/she will use all resources until the end, and only after that, when there is no more than human or financial resources to solve the family problem will seek professional help.
So, when looking for help for the family is because one has used all his/her potential and hoarded resources throughout his/her history and cultural life (spirituality, friendship, counseling, religion). So it is the duty of health professionals to act in order to allow the return of confidence in better days, looking for alternatives to resolve this complex issue and difficult for parents, professionals and society. This task would be facilitated if the current National Policy of the Brazilian Ministry of Health to provide comprehensive care to users of alcohol and other drugs were respected30.
It is common the occurrence of conflicting family relationships involved with the drug use31. In this study, although evident for the family the seriousness of the problems that drug use brings to the child, parents feel helpless, incompetent, guilty and, above all confused and divided between right and wrong and do not know what actions they should take anymore. So expect health professionals to act as facilitators and enhancers of their ability. However, what was found in the reports is that professionals are not taking effective care to this population, making the family feel alone in seeking resolution for their conflicts.
I said I will now fight for my son, for myself, I'll find a rehab clinic, I will not wait anyyhiung from them. It seems that they are no longer interested, [...] I think I was abandoned by health professionals. (F2)
[...] You get concerned,, you want to help, to do,it, but there is not an authority figureto help after discharge. They only assist in the beginning and then leave. It's when I go and fight. There are times we get discouraged because I took him four times to rehab. (F3)
Deponents express their anguish at the issues related to the treatment of their children. To hope for a treatment that seems to be appropriate, internment in a rehab, believes the professionals lost interest in the recovery of their son. Their hopes, before founded upon the professionals promoting care, were in disbelief state. However, with the perception of abandonment plus the feeling of sadness, also triggers the need to take charge of the situation.
The public policies point the basic health services as a gateway for users of alcohol and other drugs, but not always families feel welcomed, guided and cared for at this level of care. The community-based network is not able to account for the host or the maintenance of the bond, which is essential for both the beginning and for the continuity of treatment. Current policy guidelines direct assistance to a dignified care 11, suggesting that through social participation and debate, many of the difficulties faced by family members, users of the mental health network and even by health professionals can be minimized. It is very important the union of sectors such as education, social assistance, health and public safety, so that interventions are effective32.
Deficiency of whole care
Families who have members involved in problems with drug use/addiction need support and encouragement from the professionals. Without this support they even try to move forward, but they feel that it is easier to give up when faced with so many difficulties to be confronted. Usually the family knowledge is ignored, not being shared their anxieties, doubts and troubles, depriving them of knowing and especially to participate in the treatment of his family member.
They called me and just told they were taking my son to another city. I asked howcome taking? I have to go along to see where this place is, know how it works, I do not know where this city is. They did not say anything, just took him. [...] I called and said I would have to tell where my son.is [...] Idid not talk to my son in these three months was hospitalized. No contact. He was completely isolated from me. (F1)
Discontinuation of family ties became something traumatic, and the development of this feeling was hindered until this bond was reconstituted. In this case the cure has to stay in the background, it was necessary then to know where her son was; the conditions and the treatment to which it would be subjected. However, this relationship remained broken, every day of hospitalization, so that the feeling of isolation was not therapy, until his son was discharged from treatment.
However, the family should be considered as support strategy and support to the treatment and recovery for adolescent user/drug addict. Study with relatives of deinstitucionalized people makes it clear that when the patient goes home, professionals need to worry about providing an appropriate and healthy coexistence between him and the family33 . For this, specialized service is needed that support, clarify doubts and guide difficulties. This way, they can lead their lives with quality and without compromising their mental health.
Families also mentioned that professionals do not provide information nor necessary guidance so that they understand and know how to deal with situations resulting from the use of drugs.
There is lack on monitoring, better talk and guidance We do not know these things, but the professional who accompanies does, only for a while and leaves you. I realize that is not a complete treatment. There is always something missing. It is discouraging to know the need to hospitalize him again. (F3)
There is anger because they do not know what to do to help the child. The feeling is of helplessness, because the situation ends up running away from our hands. (F2)
Not receiving the proper orientation is at odds with public policies to ensure that parents and/or guardians, and other social actors, continued training on prevention of drug abuse34, it should still allow these teenagers to be heard by the professionals and be able to express their ideas about the effects of drugs35.
Families report that their children are accompanied by psychiatrists who prescribe medication and schedule new return. However, it is clear the lack for these families regarding a most effective guideline that will prepare them to deal with the problem on a daily basis. In this sense, when referring to specific situations, such as emergency care, and afterwards situations, such as after hospital discharge, reveal not having support or monitoring of the cases, making it easier to relapse and need for new admissions.
Another important issue is that professionals are exempt from caring for these adolescents, attributing success of recovery fully to the will of the same as if alone they were able to take and hold that decision.
[...] every day I would take him to the session, when one day the psychologist told him that if he did not want to go anymore, he would not have to. Al he had to do was to say he did not want treatment. She told him that, but did not tell me anything. Then, he never want to go back to the psychologist. [...] I found it wrong She should have spoken to me that would cut down the sessions or that he did not have to go to queries. (F1)
Lack of attitude stimulus and disengagement of health professionals, for the continuation of treatment, are considered inconceivable by the family. The lack of dialogue and clarification leads them to feel left behind, reflecting on the professional´s actions neglect towards his/her condition of main caregiver, and for this reason, the most interested in the child´s recovery.
The drug user, as much awareness and information they have about the drug harms, as much as they understand their own suffering and his family´s suffering, they feel difficulty to overcome alone the relationship established with the drug. In the conception of families, the position of asking the drug user to stop the use of drugs, slows the substance abandonment process for them. The point is not just to want to stop using drugs, because it depends not only on their good will, although they often claim that they can stop whenever they want to. Leaving up to their will is to attribute to them a great responsibility. There is a need to share this responsibility with parents, health professionals, and society, more experienced to address this issue, although the study emphasize that the user autonomy can promote strengthening of own choice and rebuild their lives36. This way, health workers have as challenge to realize that the events of the life of users at the moment are transient, requiring human assistance, characterized by greater sensitivity to listening and devoid of prejudices37.
According to respondents, the assistance services also do not provide adequate and sufficient support services, including the Center for Psychosocial Care (CAPS).
They took us to CAPS and said that he would make a therapeutic treatment. He went on that day and two others. Then he didn´t go back because he was not asked to go. (F1)
I would send him to CAPS, but he did not fit because there are people of various ages, [...]there are things they do that make him not fit in treatment. (F6)
Drug addiction affects people in different ways and for different reasons, in various contexts and circumstances. A care policy must focus on the needs of users who often do not correspond to the health professional expectations regarding abstinence, a factor that makes it difficult to treatment adherence and preventive practices or promotion focused to users who do not feel welcomed in their differences26.
In this sense, the poor quality of health care services of these adolescents makes them very vulnerable, requiring from family, health care and education professionals, an analysis of the problems, and a proper systematization of actions aiming to an efficient service to this group38.
Study of adolescents asserts that for a good treatment, the activities should be attractive and motivating, so that will help them to choose to be in treatment at the expense of being in drug exposure situations. It also suggested that treatment should be restricted to this age group2 .
Therefore, the need for treatment programs specially designed for the younger age groups is unquestionable, since their needs are different from those of adults. The interest of young people is increasingly moving to outside activities, interaction with mates and heterosocial relations, spending less time in close contact with their families38.
On the other hand, even the same family reporting exhaustion with consequences of the drug abuse by adolescents, they keep the frequent search for any kind of aid
[...] I love him, but I got tired, I do not want to hospitalize him anymore. I always hospitalize him believing that there will be a change, but in a little, while, where is the help? It seems that professionals have no liability after discharge. (F4)
I went to the child council and said that I can not be chasing him, they have a car, it's easier than for me, who just have a bike. The child protection agency´s fellow said that my son has no cure, and that they already gave up on him. (F5)
Desperate with the condition of a drug addict family member, the last family sought the help of the child protection agency and concluded that the institution has already given up on him. It is concerning this abandonment to the family, in which the public agency, in theory would be an interventionist alternative to such severe reality, but, in practice, claims that there is nothing to do or simply do not take responsibility.
An adequate mental health care should be promoted by maintaining the quality of care offered in a comprehensive and humane way, taking into account the reality of each individual and their relationship with family and territory, and aspects of culture and leisure, supported by the apparatus that constitute the Psychosocial Care Network (RAPS).
CONCLUSION
It is noticed that the greatest need reported by family members is the lack of guidance from health professionals. For an effective treatment is necessary to have bond between adolescent and professional and the family participation in this process. In this sense, the health services should adopt strategies that meet the needs of the family so that they extend the treatment at home. Currently the public health system has a network ruled by the integration of devices for the provision of care and specific treatment needs of each adolescent users/addicted to alcohol, crack and other drugs.
In this sense, health services need to rescue activities involving the family in the process of guidance and treatment of adolescents to ensure greater results in their recovery and, consequently, improved living conditions of their families.
It is noteworthy among the limitations of this study the difficulty of contacting the families as they hardly visited adolescents and, some, gave up participating justifying to be awkward and embarrassing to admit and talk openly about the addiction of their children. Also are recommended the expansion of the universe of families to be interviewed and more consistent prospective epidemiological methods than the cross-sectional design in future research in order to get results that can be extrapolated to similar populations.
Acknowledgments: The authors thank and honor, in memoriam, Maria Angélica Pagliarini Waidman. RN, PhD, Former Professor, State University of Maringa, the collaboration in the construction of this study.
REFERENCES:
1.Malta DC, Porto DL, Melo FCM, Sardinha LMV, Monteiro RA, Lessa BH. Família e proteção ao uso de tabaco, álcool e drogas em adolescentes, Pesquisa Nacional de Saúde dos Escolares. Rev. bras. epidemiol. 2011;14(supl1):166-77.
2.Vasters GP, Pillon SC. O uso de drogas por adolescentes e suas percepções sobre adesão e abandono de tratamento especializado. Rev Latino-Am Enfermagem. [Scielo-Scientific Electronic Library Online] 2011 [cited 2016 Aug 31]. 19: [08 telas]. Available from: http://goo.gl/cvDV5
3.Oliveira MLF, Arnauts I. Intoxicação alcoólica em crianças e adolescentes: dados de um centro de assistência toxicológica. Esc Anna Nery. 2011;15(1):83-9.
4.Rodriguez VMR, Scherer ZAP. Motivação do estudante universitário para o consumo de drogas legais. Rev Latino-Am. Enfermagem. [Scielo-Scientific Electronic Library Online] 2008 [cited 2016 Sep 2]. 16:572-6. Available from: http://goo.gl/g4qNT
5.Malbergier A, Cardoso LRD, Amaral RA. Uso de substâncias na adolescência e problemas familiares. Cad Saúde Pública. [Scielo-Scientific Electronic Library Online] 2012 [cited 2016 Sep 2 ]. 28(abr):678-88. Available from: http://goo.gl/cKDDU
6.Rozin L, Zagonel IPS. Fatores de risco para dependência de álcool em adolescentes. Acta Paul Enferm. 2012(2);25:314-8.
7.Monteiro EMLM, Nascimento CAD, Almeida Filho AJ, Araújo AKA, Carmo DRB, Gomes IMB. Percepção de adolescentes infratoras submetidas à ação socioeducativa sobre assistência à saúde. Esc Anna Nery. 2011(2);15:323-30.
8.Vieira PC, Aerts DRGC, Freddo SL, Bittencourt A, Monteiro L. Uso de álcool, tabaco e outras drogas por adolescentes escolares em município do sul do Brasil. Cad Saúde Pública. [Scielo-Scientific Electronic Library Online] 2008 [cited 2016 Sep 2]. 24(3):2487-98. Available from: http://goo.gl/GkwKp
9.Machado Neto AS, Andrade TM, Fernandes GB, Zacharias HP, Carvalho FM, Machado APS et al. Reliability of a questionnaire on substance use among adolescent students, Brazil. Rev Saude Publica. 2010;44(5):830-9.
10.Seleghim MR, Oliveira MLF. Structure, relationships and history of drug use in families of crack cocaine users. Rev. Eletr. Enf. [Scielo-Scientific Electronic Library Online] 2014 [cited 2016 Sep 3]. 16(3):527-34. Available from: https://goo.gl/1uYN48
11.Conselho Nacional de Saúde (Br). Relatório Final da IV Conferência Nacional de Saúde Mental – Intersetorial, 27 de junho a 1 de julho de 2010. Brasília (DF): Ministério da Saúde, 2010.
12.Brasil.Senado Federal(Br) Lei nº 11.343, de 23 de agosto de 2006. Institui o Sistema Nacional de Políticas Públicas sobre Drogas - Sisnad; prescreve medidas para prevenção do uso indevido, atenção e reinserção social de usuários e dependentes de drogas; estabelece normas para repressão à produção não autorizada e ao tráfico ilícito de drogas; define crimes e dá outras providências. [cited 2016 Aug 31]. Available from: http://goo.gl/lHseJ
13.Brasil. Senado Federal(Br) Decreto nº 5.912, de 27 de setembro de 2006. Regulamenta a Lei no 11.343, de 23 de agosto de 2006, que trata das políticas públicas sobre drogas e da instituição do Sistema Nacional de Políticas Públicas sobre Drogas - SISNAD, e dá outras providências. [cited 2016 Aug 31]. Available from: http://goo.gl/Abno0
14.Duarte PCAV, Branco APUA. Legislação Brasileira Sobre Drogas. In: Governo Federal(Br). Legislação e Políticas Públicas sobre Drogas. Presidência da República Brasília(DF): Secretaria Nacional de Políticas sobre Drogas; 2010. p. 27-44.
15.Senado Federal(Br). Decreto nº 6.117, de 22 de maio de 2007. Aprova a Política Nacional sobre o Álcool, dispõe sobre as medidas para redução do uso indevido de álcool e sua associação com a violência e criminalidade, e dá outras providências. [cited 2016 Sep 1]. Available from: http://goo.gl/Pf4Py
16.Brasil. Decreto nº 7.179, de 20 de maio de 2010. Institui o Plano Integrado de Enfrentamento ao Crack e outras Drogas, cria o seu Comitê Gestor, e dá outras providências. [cited 2016 Sep 1]. Available from: http://goo.gl/GBILq
17. Tribunal de Contas da União(Br); Sistema Nacional de Políticas Públicas sobre Drogas. Relatório de auditoria operacional. Brasília: TCU, Secretaria de Fiscalização e Avaliação de Programas de Governo; 2012.
18.Pratta EMM, Santos MA. Reflexões sobre as relações entre drogadição, adolescência e família: um estudo bibliográfico. Estud Psicol. 2006;11(3):315-22.
19.Bardin, L. Análise de conteúdo. Tradução de Luis Antero Reto e Augusto Pinheiro. São Paulo: Edições 70/Livraria Almedina Brasil; 2011.
20.Conselho Nacional de Saúde (Br). Comitê Nacional de Ética em Pesquisa em Seres Humanos. Resolução no. 466/2012, de 12 de dezembro de 2012. Brasília(DF): CNS; 2012.
21.Capistrano FC, Ferreira ACZ, Silva TL, Kalinke LP, Maftum MA. Perfil sociodemográfico e clínico de dependentes químicos em tratamento: análise de prontuários. Esc Anna Nery. [Scielo-Scientific Electronic Library Online] 2013 [cited 2016 Sep 1]. 17(2):234-41. Available from: http://goo.gl/zQjI6k
22.Chatterji P. Illicit drug use and educational attainment. Health Econ. 2006;15(5):489-511. DOI: 10.1002/hec.1085
23.Galduróz JC, Sanchez ZVDM, Opaleye ES, Noto AR, Fonseca AM, Gomes PLS, et al. Fatores associados ao uso pesado de álcool entre estudantes das capitais brasileiras. Rev Saude Publica. 2010; 44(2):267-73.
24.Poulin C, Hand D, Boudreau B, Santor D. Gender differences in the association between substance use and elevated depressive symptoms in a general adolescent population. Addiction. [Scielo-Scientific Electronic Library Online] 2005 [cited 2016 Aug 31]. 100(4):525-35. Available from: http://goo.gl/Q0P5d
25.Sanches RP, Leopardi MT. Tecnologia de abordagem para o cuidado ao usuário de drogas. Sau & Transf Soc. 2012;3(3):03-10.
26.Pinho PH, Oliveira MA, Almeida MM. A reabilitação psicossocial na atenção aos transtornos associados ao consumo de álcool e outras drogas: uma estratégia possível? Rev Psiquiatr Clin. [Scielo-Scientific Electronic Library Online] 2008. [cited 2016 Aug 31]. 35(3):82-8. Available from: http://goo.gl/7eyC7
27.Dietz G, Santos CG, Hildebrandt LM, Leite, MT. As relações interpessoais e o consumo de drogas por adolescentes. SMAD, Rev Eletrônica Saúde Mental Álcool Drog. [Scielo-Scientific Electronic Library Online] 2011 [cited ago 31 2016]. 7(2):85-91. Available from: http://goo.gl/xg3ZQ
28.Claro HG, Oliveira MAF, Ribeiro APR, Fernandes CC, Cruz AS, Santos EGM. Profile and pattern of crack use by children and adolescents living on the streets: an integrative review. SMAD, Rev Eletrônica Saúde Mental Álcool Drog. [Scielo-Scientific Electronic Library Online] 2014 [cited 2016 Aug 27]. 10(1)35-41. Available from: http://goo.gl/ePhEex
29.Seleghim MR; Galera SAF, Oliveira MLF. Study with Crack users and their Families: Experience Report. Saúde Transform. Soc. [online]. [Scielo-Scientific Electronic Library Online] 2014 [cited 2016 Sep 2], 5(1):36-41. Available from: http://goo.gl/2iCUZp
30.Brasil. Portaria nº 2.197/GM, em 14 de outubro de 2004. Redefine e amplia a atenção integral para usuários de álcool e outras drogas, no âmbito do Sistema Único de Saúde - SUS, e dá outras providências. Brasília (DF): Gabinete Ministerial; 2004.
31.Pereira VCLS, Pimentel LF, Espínola LL, Azevedo EB, Ferreira Filha MO. Psychological distress in adolescents who experience changes in family dynamics as a result of alcoholism. Rev enferm UERJ. 2015; 23(6):838-44.
32.Oliveira MAF, Gonçalves RMDA, Claro HG, Tarifa RR, Nakahara T, Bosque RM, Silva NN. Profile of homeless children and teens drug users. Rev enferm UFPE on line. [Scielo-Scientific Electronic Library Online] 2016 [cited 2016 Sep 2], 10(2):475-84. Available from http://goo.gl/Z1HXXT
33.Waidman MAP, Radovanovic CAT, Scardoelli MGC, Estevam MC, Pini JS, Brischiliari A. Estratégia de cuidado a famílias de portadores de transtornos mentais: experiências de um grupo de pesquisa. Cienc cuid saude. 2009;8(10):9724
34. Presidência da República (Br) Legislação e Políticas Públicas sobre Drogas Brasília (DF), Secretaria Nacional de Políticas sobre Drogas; 2010.
35.Silveira HS, Ferreira VS, Zeitoune RCG, Ana Maria Domingos AM. Efeitos das drogas lícitas e ilícitas na percepção de adolescentes: uma abordagem de enfermagem. Rev enferm UERJ. 2013 dez; 21(6):748-53.
36. Oliveira GC, Cíntia Nasi C, Lacchini AJB, Camatta MW, Maltz C, Schneider JF. Psychosocial rehabilitation: process of reconstructing drug users' subjectivities. Rev enferm UERJ. 2015; 23(6):811-6.
37.Pereira MO, Vargas D, Oliveira MAF. Reflexão Acerca da Política do Ministério da Saúde Brasileiro para a atenção aos usuários de álcool e outras drogas sob a óptica da sociologia das ausências e das emergências. SMAD, Rev Eletrônica Saúde Mental Álcool Drog. [Scielo-Scientific Electronic Library Online] 2012 [cited 2016 Aug 28]. 8(1):9-16. Available from: http://goo.gl/MVu2f
38.Davim RMB, Germano RM, Menezes RMV, Carlos DJD. Adolescente / Adolescência: revisão teórica sobre uma fase crítica da vida. Rev RENE. 2009;10(2):131-40.