RESEARCH ARTICLES
Prevalence of mammographic examination in Brazilian women in the period from 2009 to 2010
ABSTRACT: To analyze the prevalence and factors associated with the mammography examination undertaken by Brazilian women. This is an epidemiological and cross-sectional study. We have analyzed secondary data from the Brazilian Information System on Breast Cancer. We found that 86,01% (n=742.004) of women subjected to mammography in 2009 and 87,42% (n=2.231.668) in 2010 belonged to the age group from 40 to 69 years old. With regard to schooling, the significant prevalence of incomplete elementary school reached 52,42% in 2009 and 54,24% in 2010. Our findings indicate that 90,1% (n=777.194) of women who underwent mammography in 2009 and 89,98% (n=2.297.490) in 2010 did not report high risk factors for breast cancer. A greater number of women showed positive attitudes in relation to mammography, which is a factor that is considered positive for conducting such an examination.
Keywords: Women's Health; Breast Neoplasms; Mammography; Epidemiology.
INTRODUCTION
Neoplastic diseases represent one of the main causes of morbidity and mortality across the world, highlighting breast cancer in the female population. It is estimated that occurs more than 1.050.000 new cases of breast cancer in the world each year, which makes this type of cancer one of the most prevalent among women1. By corroborating this configuration, Brazil showed incidence rates of 49.000 cases of breast neoplasm per 100.000 in the year 2011, following the same profile of the magnitude observed for Latin America2.
Based on the high incidence rates caused by this neoplasm, Brazilian health authorities have been concerned to encourage women to perform an early detection of this disease, since in many cases it is only diagnosed in advanced stages. Thus, early detection is the most effective method to reduce the morbidity and mortality rates of breast cancer3-5.
The main procedures used in early detection of breast neoplasms in Brazil are: clinical breast examinations and mammography6,7, corroborating with international studies8-10. The accomplishment of mammography fosters the diagnosis and the monitoring of breast alterations, whether they have a benign or malignant nature, whether they are invasive and that raise the suspicion of malignancy and, thereby, contribute to darkest prognoses. In both cases, the benefits established by early diagnosis might expedite the health assistance and, consequently, favors a decrease in the amount of women affected by processes in advanced stages, i.e., with little possibilities of treatment11.
Among the factors that contribute to late detection of breast cancer in the female population in Brazil, one can cite low schooling level and poor access to information, deficiency in the development of public policies for women and the fear generated by this neoplasm associated with lack of knowledge about this pathology and the diagnostic methods11,12.
Before this reality, the Brazilian Ministry of Health, through the National Plan of Policies for Women, seeks to reduce morbidity and mortality from breast cancer among this audience. For this purpose, it has expanded access to health services, both in prevention attendance and in assistance focused on treatment and rehabilitation13.
In this sense, it is important to identify the factors influencing with the non-adherence of women in facing mammography, assisting nursing professionals to target their care shares towards the most appropriate type of intervention for that the accomplishment of the examination is materialized and the overcoming problems might be reached in health services, thus encouraging development and investment of public policies aimed at conducting an early diagnosis of breast cancer.
The goal of this study was to analyze the prevalence and the factors associated with the accomplishment of mammography by the female population of Brazil.
METHODOLOGY
This is an epidemiological and cross-sectional study. We have analyzed secondary data from the Information System on Breast Cancer in Brazil (SISMAMA). Among the strategic priorities in the plan for controlling cancer in Brazil, the strengthening of information systems is the method that supports the implementation and continuous assessment of programs for early detection. The strategic importance of using clinical data generated in the National Cancer Institute, in partnership with the Computer Science Department of the Unified Health System (DATASUL), to develop the Information System for the Control of Breast Cancer (known by its abbreviation SISMAMA : SIS for the System; MAMA for breast – in Portuguese, breast is translated into mama). The SISMAMA was designed as a management tool to capture, organize and disseminate epidemiological data available on the tested population, with emphasis on test results, monitoring of unusual cases, quality of services, as well as other essential information generated in the course of providing screening tests. We chose to study women in all age groups, whose data were obtained in 2009 and 2010.
In order to further improve the SISMAMA, the Department of the Brazilian Unified Health System (DATASUL), in partnership with the National Cancer Institute, developed the first version of the SISMAMA (1.0), a computerized system for managing information of health units, being that it is continuously updated. The SISMAMA is a management tool of local, state and municipal integration, also encompassing health laboratories and clinical units of mammography. Then, the data are consolidated in the SISMAMA, with a national profile of the programs for controlling breast cancer.
Structured forms provided by all institutions able to perform benchmark tests of breast continuously feed this database. These tools request sociodemographic and clinical characteristics of the patient. After collecting information, on the part of the professional, the data are plotted in the SISMAMA. The database is available for internet access. Accordingly, in our study, we present updated data of the SISMAMA.
The data processing and analysis were performed by using the TabWin (DATASUL) and Excel (Microsoft®) softwares. In order to assess the epidemiological and operational indicators of this population, we have considered the standards of the World Health Organization (WHO), which are recommended by the Brazilian Ministry of Health.
The demographic data, based on the last Brazilian census (2010), were obtained from the Brazilian Institute of Geography and Statistics (IBGE). We have assessed the following variables: age, schooling, breed / color, increased risk of cancer, clinical examination and prior mammography, as well as time interval between mammography examinations, when the patient had been subjected to more than one.
RESULTS AND DISCUSSION
Based on the SISMAMA report, the amount of mammographies in Brazil tripled in 2010 compared to 2009. This is mainly due to the fulfillment of the Law nº 11.664 of the Brazilian Ministry of Health, which ensures assistance to breast health for women throughout the country. This law ensures the free completion of the mammography through the public health system, after 40 years of age. Enacted in 2009, this Law has fostered mammography examinations in public health unit across the country and has encouraged health professionals to sensitize patients towards the development of preventive measures against breast cancer. Nonetheless, only in 2010, the majority of the population was aware of the Law at stake, which generated a greater demand for examination, triggering an increased demand for public health services and, therefore, overloading the system.
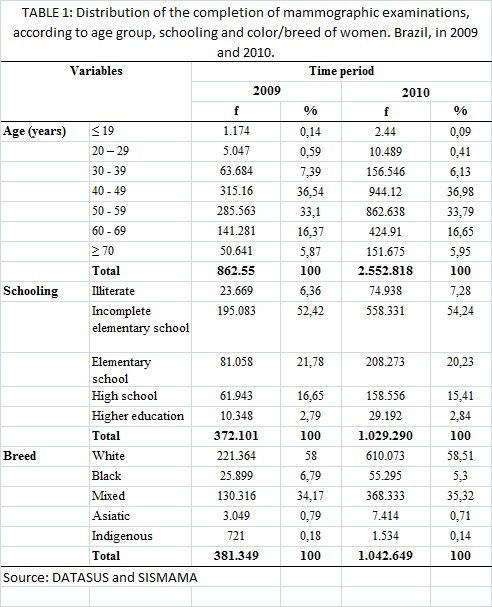
As to sociodemographic characteristics, 86,01% (n=742.004) of women who underwent mammography, in 2009, and 87,42% (n=2.231.668), in 2010, were aged from 40 to 69 years. It was found that women who had 19 years or less had the lowest rates of adherence to mammography, since this specific population portion does not constitute a risk group for the detection of breast cancer. Regarding the schooling level, the significant prevalence of incomplete elementary school was observed among those who were assessed, reaching 52,42% (n =195.083) in 2009, followed by complete elementary school with 21,78% (n=81.058). In 2010, the data were similar, with 54,24% (n=558.331) denoting the incomplete elementary school and 20,23% (n=208.273) reaching the complete elementary school. The high rates of underreporting in relation to educational levels still are configured as a problem, representing more than 50% in both years. Cases with unknown information recorded in the questionnaire were excluded from the analysis. Women who underwent mammography in the years 2009 and 2010 were mostly whites, which is equivalent to 58% (n=831.437) and 58.51% (n=610.073) of the total of reports, respectively. Women who had been classified as blacks also showed high rates of adherence to mammography, which represents 34,17% (n=130.316) in 2009 and 35,32% (n=368.333) in 2010, as shown in Table 1.
The data presented here indicate a significant increase in completion of mammographies by women aged from 40 to 49 years (36,9%) and from 50 to 59 years (30,76%), followed by the age group of 60 to 69 years (14, 83%). The same outcomes were found in other researches14,15.
A study, conducted with 16.570 women aged from 50 to 59 years and 10.722 women aged from 60 to 69 years, showed significant and positive associations for all indicators of health services, including mammography15. In contrast, another study showed that women between 51 and 60 years old performed fewer mammography examinations16. In addition, corroborating our data, another study found that most women under the age of 35 years never underwent a mammographic examination17.
Other researchers16 have identified that breed (probably associated with economic issues) is a factor that influences with the adherence to mammography as a method of secondary prevention, given that 81,1% of 439 women subjected to this examination belonged to the white breed. Our study reinforces that the Brazilian white women are the majority of users of this type of examination.
Although we have not found studies that prove the relationship between high risk for breast cancer and the accomplishment of the mammographic examination, one can identify that there is a greater number of women who are subjected to mammography when there is the presence of high risk. Some researchers argue that the recognition of a risk factor in the patient consists of a warning sign to raise awareness in relation to cancer, which consequently leads them to the search for preventive measures of the disease before it is installed17.
In the current study, we have found that the schooling level is an important factor for the adherence towards the mammography, as found by other authors16. Factors such as age, schooling level and breed influence actions for the secondary prevention of breast cancer. It should be emphasized that the higher education is strongly correlated with better prevention measures. The authors also mention income, religion and hormone therapy as other factors that influence this practice. The economic and educational classes are factors that significantly influence with the performance of preventive actions. Nevertheless, according to a survey conducted with older women, the non-completion of mammographies is associated with the following topics: to be older, to live without a partner, low schooling level and family income less than three minimum wages18.
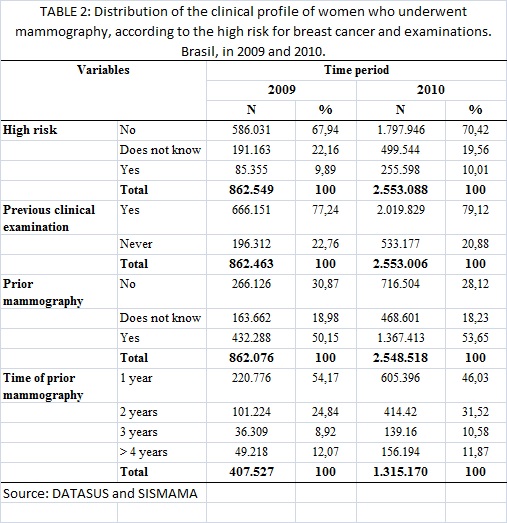
In Brazil, 90,1% (n=777.194) of women who underwent mammography in 2009 and 89,98% (n= 2.297.490) in 2010 reported no risk factors for breast cancer. Furthermore, most of them underwent previous clinical examinations: 77,24% (n= 666.151) and 79,12% (n=2.019.829) of cases in 2009 and 2010, respectively. In relation to a prior mammography, it was found that 50,15% (n= 432.288) of women in 2009 and 53,65% (n=1.367.413) in 2010 already had at least one previous mammography examination. However, there is a high number of women who do not know the answer or have never had a previous accomplished mammography examination, accounting for nearly half of the cases recorded in the two analyzed years, as shown in Table 2.
Similar to another study19, our data revealed that certain social characteristics, such as family risk for developing breast cancer, the clinical breast examination and prior mammography are factors that lead to the completion of mammography.
In this study, we have reviewed the official data that demonstrated an increase in the amount of mammographies conducted in 2010, especially for women who had undergone previous breast examinations. Similarly, a study involving 48.421 women showed that 75,3% of women reported that their breasts were examined in the last gynecological consultation, which denotes correlation between the performance of clinical breast examination and mammography20. Interestingly, there was a relationship between the number of reports of women who had visited a gynecologist in the last two years and the marked increase in the referral appointed by physicians to mammographic examinations in 2000, if it is compared with the rates of 199421. We believe that this change is of great interest, whether the oncologist plays a key role in women's access to prevention programs against breast cancer.
The completion of a previous mammography might positively influence with the accomplishment of next mammographic examination, especially if there is a short time interval among examinations. It was also observed in another study22 that 61,5% of American women of 40 years who were subjected to mammography had attended at least one mammographic appointment before.
CONCLUSION
The study found improvements in the mood of Brazilian women for the accomplishment of mammographic examinations in 2010 compared to 2009. A larger number showed positive attitudes towards the practice of mammography, being that it is a key factor for the completion of such a clinical procedure. Early prevention and identification are important requisites for reducing morbidity and mortality rates caused by breast neoplasm.
It is relevant to note that, in most cases, breast cancer has a good prognosis when diagnosed early and treated in an appropriate way. Therefore, the nursing care shares to support and/or encourage women to conduct breast examinations are crucial for early detection and treatment of breast cancer, thus contributing to the improvement of the life quality of this population.
REFERENCES
1. Matos JC, Pelloso SM, Carvalho MDB. Fatores associados à prevenção secundária do câncer de mama. Cad Saúde Pública. 2011; 27: 888-98.
2. Ministério da Saúde (Br). Instituto Nacional de Câncer. Estimativa 2010: Incidência de Câncer no Brasil. Rio de Janeiro: INCA; 2009.
3. Ministério da Saúde (Br). Instituto Nacional de Câncer do Brasil. Estimativa da incidência de câncer para 2008 no Brasil e nas cinco regiões. [citado em 6 set 2012] Available at: http://www.inca.gov.br.
4. Viana LC, Martins M, Geber S. Ginecologia. Rio de Janeiro: Medsi; 2001.
5. Gonçalves ATC, Jobim PFC, Vanacor R, Nunes LN, Albuquerque IM, Bozzetti MC. Câncer de mama: mortalidade crescente na Região Sul do Brasil entre 1980 e 2002. Cad Saúde Pública. 2007; 23: 1785-90.
6. Inagaki ADM, Prudente LR, Gonçalves LLC, Abud ACF, Daltro AST. Prática para detecção precoce do câncer de mama entre docentes de uma universidade. Rev enferm UERJ. 2008; 16: 388-91.
7. Ministério da Saúde (Br). Instituto Nacional de Câncer do Brasil. Detecção precoce do câncer de mama. [citado em 20 set 2012] Available at: http://www.inca.gov.br/conteu do_view.asp?id=1932.
8. Brown SR, Nuno T, Joshweseoma L, Begay RC, Goodluck C, Harris RB. Impact of a community-based breast cancer screening program on Hopi women. Prev Med. 2011; 52: 390-3.
9. Van Schoor G, Moss SM, Otten JD, Donders R, Paap E, den Heeten GJ, Holland R, Broeders MJ, Verbeek AL. Increasingly strong reduction in breast cancer mortality due to screening. Br J Cancer. 2011; 104: 910-4.
10. Williams KP, Mabiso A, Todem D, Hammad A, Hill-Ashford Y, Hamade H, Palamisono G, Robinson-Lockett M, Zambrana RE. Differences in knowledge of breast cancer screening among African American, Arab American, and Latina women. Prev Chronic Dis. 2011; 8: 1-11.
11.Gonçalves LLC, Lima AV, Brito ES, Oliveira MM, Oliveira LAR, Abud ACF, et al. Mulheres portadoras de câncer de mama: conhecimento e acesso às medidas de detecção precoce. Rev enferm UERJ. 2009; 17: 362-7.
12. Jácome EM, Silva RM, Gonçalves MLC, Collares PMC, Barbosa IL. Detecção do câncer de mama: conhecimento, atitude e prática dos médicos e enfermeiros da estratégia saúde da família de Mossoró, RN, Brasil. Revista Brasileira de Cancerologia. 2011; 57: 189-98.
13. Ministério da Saúde (Br). Secretaria Especial de Políticas para as Mulheres. Plano Brasileiro de Políticas para as Mulheres. 2005. [citado em 20 set 2012] Available at: http://www.portal.saude.gov.br.
14. Marconato RRF, Soaréz PC, Ciconelli RM. Custos dos mutirões de mamografia de 2005 e 2006 na Direção Regional de Saúde de Marília, São Paulo, Brasil. Cad Saúde Pública. 2011; 27: 1529-36.
15. Lima-Costa MF, Matos DL. Prevalência e fatores associados à realização da mamografia na faixa etária de 50-69 anos: um estudo baseado na pesquisa nacional por amostra de domicílios (2003). Cad Saúde Pública. 2007; 23: 1665-73.
16. Matos JC, Pelloso SM, Carvalho MDB. Fatores associados à realização da prevenção secundária do câncer de mama no Município de Maringá, Paraná, Brasil. Cad Saúde Pública. 2011; 27: 888-98.
17. Lima ALP, Rolim NCOP, Gama MEA, Pestana AL, Silva EL, Cunha CLF. Rastreamento oportunístico do câncer de mama entre mulheres jovens no Estado do Maranhão, Brasil. Cad Saúde Pública. 2011; 27: 1433-9.
18. Novaes CO, Mattos IE. Prevalência e fatores associados a não utilização de mamografia em mulheres idosas. Cad Saúde Pública. 2009; 25: 310-20.
19. Fernandes AFC, Viana CDMR, Melo EM, Silva APS. Ações para detecção precoce do câncer de mama: um estudo sobre o comportamento de acadêmicas de enfermagem. Cienc Cuid Saude. 2007; 6: 215-22.
20. Amorim VMSL, Barros MBA, César CLV, Carandina L, Goldbaum M. Fatores associados a não realização da mamografia e do exame clínico das mamas: um estudo de base populacional em Campinas, São Paulo, Brasil. Cad Saúde Pública. 2008; 24: 2623-32.
21. Matos SL, Santos MMP. Diferencias en los factores relacionados con el uso de la mamografía en las mujeres españolas en los años 1994 y 2000. Rev Esp Salud Publica. 2005; 79: 517-20.
22. Feig SA. Screening mammography: a successful public health initiative. Rev Panam Salud Publica. 2006; 20:125-33.