
(*) Note: Most of the elderly women had more than a health problem.
ORIGINAL RESEARCH
Frailty, illness and functional capacity in older women
Marcella Costa Souto DuarteI; Maria das Graças Melo FernandesII; Rosalina Aparecida Partezani RodriguesIII; Maria Miriam Lima da NóbregaIV
I
PhD in Nursing. Professor of the Nursing Course at the University Center of
João Pessoa and member of the Group for Studies and Research on Adult and
Elderly Health. João Pessoa, Paraíba, Brazil. E-mail: marcellasouto@hotmail.com
II
PhD in Sociology. Professor at the Department of Clinical Nursing of the
Federal University of Paraíba. Leader of the Group for Studies and Research
on Adult and Elderly Health. João Pessoa, Paraíba, Brazil. E-mail:
graacafernandes@hotmail.com
III
PhD in Nursing. Professor of the Postgraduate Program in Fundamental
Nursing at the Ribeirão Preto School of Nursing, University of São Paulo.
Brazil. E-mail:
rosalinapartezani@yahoo.com.br
IV
PhD in Nursing. Professor of the Postgraduate Program in Nursing at the
Federal University of Paraíba. João Pessoa. Brazil.. E-mail: miriam@ccs.ufpb.br
V
Extracted from DUARTE, MCS. Frailty and associated factors in elderly women
in the city of João Pessoa-PB. (Masters' dissertation). Postgraduate
Program in Nursing, Federal University of Paraíba, 2012, linked to the
project Life conditions, health and aging: a comparative study, funded by
the National Program for Academic Cooperation Novas Fronteiras /
Coordination for Improvement of Higher Education Personnel, 2428/08.
DOI: http://dx.doi.org/10.12957/reuerj.2016.6801
ABSTRACT
Objectives: to estimate the prevalence of frailty in older women living in the city of João Pessoa (Paraíba) and find the association, in this group, between frailty and the clinical variables 'reported disease' and 'functional capacity'. Method: the sample consisted of 166 women aged 60-96 years. Data were collected using the interview technique. The empirical material was collected from April to June 2011 and was analyzed quantitatively using descriptive statistics. Results: most of the women (60.8%) had some degree of frailty, including 21.7% apparently suffering from vulnerability, and the remainder, from weakness: 23.5% mild, 7.8% moderate and 7.8% severe. Regarding the determinants of frailty, was found its association with performance in activities of daily living. Conclusion: differential healthcare is needed for elderly women, with a view to preventing this event.
Keywords: Frail older adults; aging; morbidity; activities of daily living.
INTRODUCTION
The increase of the elderly populationV has been a worldwide phenomenon, but in Brazil, there has also been an accelerated increase. These data are the result of declining of fertility and mortality rates. With the change in the health profile of the population, there has been an increased incidence of chronic diseases, which may be accompanied by sequelae, limit the functional performance and generate dependence 1.
On the national scene, there are 20.5 million seniors, representing 11% of the population. Estimates of the Brazilian Institute of Geography and Statistics show that by 2050 the number of elderly is expected to reach 56 million, representing 24% of the population2. In this context, there is another phenomenon, the feminization of old age, which arouses the interest of scholars, society and government 3 and it is explained in part by the higher life expectancy of women, associated with factors such as lower consumption of alcohol and tobacco and differences in attitude toward health problems, and their ability to perform duties4.
Whereas chronic diseases and functional disabilities impact the family, the health system and the daily lives of older people, as these cause more vulnerability and dependence, the aforementioned health condition often culminates in a frail status5. It is a state of vulnerability to stressors that result in the decline of physiological reserves, with subsequent decrease in efficiency of homeostasis6. For this reason, there must be efforts to prioritize its progress with a view to ensuring longevity to seniors with adequate health conditions, autonomy, independence and better quality of life 7. It is important to note that the loss of the elderly's capacity, due to physical or mental illness, can lead to the need for intervention and adjustments to keep the routine activities and lifestyle, requiring constant efforts from professionals working especially in primary health care8.
In this perspective, considering the factors associated with frailty among the elderly, different studies have pointed morbidities and functional impairment affecting, in particular, their lifestyle and increase their exposure to health risks9. However, studies on the incidence and factors associated with frailty in the elderly are still scarce10, which brings the need to evaluate these aspects in this population, especially among those living in the community and women. Thus, in order to contribute to fill gaps in knowledge regarding the factors involved in the occurrence of this phenomenon, particularly in older women, this study aimed to estimate the prevalence of frailty in older women living in the city of João Pessoa (Paraíba) and investigate the association between frailty, morbidity and functional capacity in this group of women.
The study is justified because it provides significant scientific and social relevance in the health field, with emphasis on the importance of screening and early detection of frailty in older women, which obviously will contribute to provide them with a differentiated care in the health services, particularly in nursing care.
THEORETICAL FRAMEWORK
The definitions found for frail elderly during the 1980s included characteristics such as age equal to or over 75 years old, vulnerability, physical and / or cognitive impairment, participation in geriatric programs, need for institutional care and dependence to perform the Activities of Daily Living (ADLs). In the 1990s, the index of the Journal of the American Geriatrics Society published, for the first time, the term frail elderly, which aroused the interest of researchers in this area11.
In modern days, two international research groups have stood out by trying to achieve a consensus definition of frailty and by their studies of tools to deal with the said condition: in the United States, the Johns Hopkins University; and in Canada, the Canadian Initiative on Frailty and Aging (CIF-A).
The Johns Hopkins University, USA, conducted a study12 in order to set objective and measurable criteria to define frailty in the elderly based on the hypothesis that it is a syndrome that can be identified by a phenotype. Based on this proposition and its application in a group of 5,317 elderly aged ≥ 65 years, who lived in the community, the authors of the study found the prevalence of the syndrome of 6.9% and incidence of 7.2%, in four years, especially among women.
The research (CIF-A), developed between Canada, the European Union, Israel and Japan, began in 2002 and sought to increase knowledge on frailty in the elderly, through a careful study of the causes and the course of the phenomenon, with an emphasis on its prevention and treatment, considering the phenomenon in a multidimensional perspective. In this assumption, the identification of frailty in seniors involves evaluating elements such as cognition, humor and social support13. In line with this perspective, currently, frailty is understood as an event determined by biological and psychosocial aspects. This way of understanding the phenomenon was adopted in this study.
METHODOLOGY
This is a cross-sectional research conducted in the city of João Pessoa, the capital of Paraiba state. It is a subproject of the research Condições de vida, saúde e envelhecimento: um estudo comparado (Living conditions, health and aging: a comparative study), funded by PROCAD / CAPES, a partnership between the Federal University of Paraíba and Ribeirão Preto School of Nursing - University of São Paulo.
The base population for sample calculation comprised a group of elderly aged sixty years or older and living in the said municipality. The sample was probabilistic, by double-stage conglomerates, of which 240 elderly were selected, and 166 (69.16%) were women, who met the following inclusion criteria: aged equal to or less than sixty years old and living in the area of the municipality defined in the sampling process.
Data collection was carried out through structured interviews in the homes of the elderly, from April to June 2011. For this, authors used an instrument with questions regarding the clinical variable referred morbidity, the Katz Index and the Lawton Scale to assess the functional capacity of these women, regarding their performance of basic and instrumental activities of daily living, as well as the Edmonton Frail Scale (EFS)14, which was validated and culturally adapted to the elderly population of Ribeirão Preto (São Paulo)15 and that identifies the frailty from nine domains: cognition, general health status, functional independence, social support, use of medication, nutrition, humor, continence and functional performance. In the interpretation of scores to analyze frailty, it is considered that: individuals with score 0-4 do not present frailty; 5-6 are apparently vulnerable to frailty; 7-8 have mild frailty; 9-10, moderate frailty; and 11 or more, severe frailty. It should be noted that the maximum score is 17, which represents the highest level of frailty.
Data analysis was carried out in a quantitative approach, using descriptive statistics and the Statistical Package for Social Sciences (SPSS) - version 15.0, to be appropriate to achieve the objectives of the study and to enable accuracy and generalization of the results. The descriptive analysis was developed using mean, standard deviation and absolute and relative frequencies. In the stage of the confirmatory analysis, contingency tables were built for qualitative variables and the chi-square test Pearson (x2) or the Fisher's exact test was applied to identify possible association between the independent variables (morbidity and functional capacity) and the dependent variable (frailty). For the quantitative variables, the analysis of variance (ANOVA) or the Mann-Whitney test was used, and to verify the correlation between these variables, authors used the Pearson's test or nonparametric Spearman's test. The significance level used in the study was 5%.
It is worth noting that the research followed the guidelines and ethical standards established in Resolution. 196/96 by the National Health Council16, regulating research involving human beings, especially with regard to the consent of the participants and their anonymity and confidentiality of private data. Therefore, according to the ethical requirements of the said Resolution, the research was assessed by the Research Ethics Committee of the Lauro Wanderley University Hospital of the Federal University of Paraiba, and approved under Opinion No. 680/10.
RESULTS AND DISCUSSION
Sociodemographic characteristics, morbidity and functional capacity
Of the 166 elderly women who participated in the study, 41 (24.7%) were aged 80 years or older. The age ranged between 60 and 96 years, with an average of 73.25. Regarding marital status, 70 were widows (42.2%). Regarding the level of education of the elderly, the average years of study was equivalent to 6.48 and standard deviation (SD) of 6.1. Among them, 48 (28.9%) had between 5 and 8 years of study, and 45 (27.1%) were illiterate. With regard to individual income, the average was R$ 1,299.38, and the average household income, including the elderly, was R$ 2,990.23. Regarding the type of income, 123 (74.1%) of the surveyed seniors received retirement.
Considering the characteristics of these elderly women related to socio-demographic indicators, there was the prevalence of women aged 80 and older, low level of education and income, as well as multigenerational family arrangement as living scenario. This reflects the reduced access to school and underemployed occupied by them, which has led to lower incomes and poorer quality of life.
Regarding the multigenerational family arrangement, this was a domestic organization characteristic of the poorest elderly Brazilians, which is composed of children, grandchildren and the elderly person. This finding is worrying, since among the families of Brazilian low-income seniors, the elderly person is often the main member to provide economic support to their household.
As for the reported morbidities, there was a highlight to hypertension (62.7%), as shown in Table 1. A study conducted in Bambuí, Minas Gerais, Brazil, corroborates this finding, in which there was a prevalence of 62%of hypertension among elderly17. It should be noted that chronic diseases, especially hypertension, generate great economic impact on society18. Moreover, they represent a significant and growing demand for health services, and this highlights the need to monitor their prevalence, because their remarkable characteristics are duration and risk of complications, which requires strict control scheme and permanent care because of the possible sequelae that may involve functional disability and highlight the role of the family, with regard to their responsibilities in the elderly care19.
Besides, the health problems most often expressed by the elderly women were spine problems (77 - 46.4%), impaired vision (71 - 42.8%), rheumatoid arthritis / osteoarthritis (57 - 34.3%) and osteoporosis (48 - 28.9%), according to Table 1.
TABLE 1: Distribution of elderly women according to referred morbidity, João
Pessoa, PB, Brazil, 2011 (N=166).
(*)
Note: Most of the elderly women had more than a health problem.
Considering the functional capacity for the activities of daily living, as assessed by the Katz index, 123 (74.1%) of the elderly women are independent. As for the instrumental activities of daily living (IADL) - preparing meals, performing household chores, washing, handling money, using the telephone, taking medications, shopping and using means of transportation - assessed by Lawton Scale, 83 (50%) of the older women said they need help to carry out these activities. Thus, it was found that 83 (50%) of the women surveyed presented functional impairment for the realization of Instrumental Activities of Daily Living (IADL).
Nevertheless, some studies 17-20 have shown that sociodemographic variables such as age, gender, family structure and education influence on the functional capacity of the elderly. Similarly, there is association between chronic disease and functional disability among the elderly21.
Prevalence of frailty and association with referred morbidity and functional capacity
Regarding the prevalence of frailty, it was found that 65 (39.2%) elderly women had no frailty, 36 (21.7%) were apparently vulnerable, while 65 (39.2%) showed different levels of frailty, namely: 39 (23.5%) had mild frailty, 13 (7.8%), moderate, and 13 (7.8%), severe. In a study 12 that evaluated 5,317 elderly of a community of the United States, it was found frailty in 7% of them. In another study15 where the Edmonton Frail Scale was used in 137 elderly of a community of São Paulo, it was found that 4.5% of them had severe frailty. These findings point to the variability of prevalence rates of frailty according to the measuring instrument used.
In the analysis of possible association between frailty and morbidity, it was observed that the prevalence of frailty was more frequent among those who showed higher averages for the following health problems: neurological disease (Parkinson / sclerosis), stroke and depression. Thus, the data show that the elderly women having these health problems were among those who had some degree of frailty, according to Table 2. Besides the signs and clinical symptoms of frailty, there are other important components that can lead its occurrence, such as changes in mood and in cognition22.
TABLE 2: Distribution of elderly women according to morbidity and average score of
frailty, João Pessoa, PB, Brazil, 2011 (n=166).

As for the factors involved in determining frailty, the literature shows that individuals with installed morbidities are more likely to frail aging 13. Regarding this reality, a study on frailty and quality of life related to seniors' health, held in Mexico, found that the majority of elderly patients with frailty had at least one chronic disease23 . Corroborating these findings, other study22 found that the presence of morbidity in the elderly predisposes the onset of frailty. Thus, the development of chronic diseases can accelerate the onset of frailty, since these health changes require the body to use the available resources, which may lead to depletion of body reserves23.
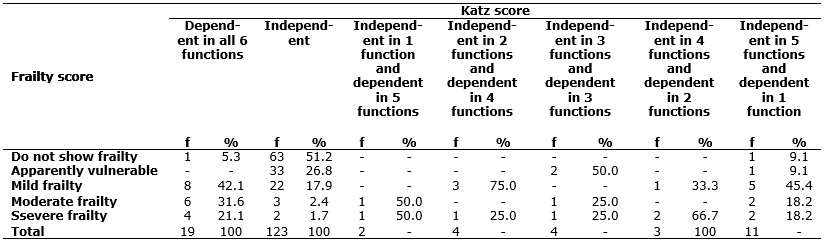
The correlation between the raw scores of frailty and the performance of ADLs, using the ANOVA test, showed a statistically significant correlation between these variables (p <0.0001), since among the elderly women dependent in all six functions, 8 (42.1%) had mild frailty, 6 (31.6%), moderate frailty, and 4 (21.1%) evidenced severe frailty. Concerning the elderly women independent in five functions and dependent in one function, 5 (45.5%) had mild frailty, 2 (18.2%) had moderate frailty, and 2 (18.2%) evidenced severe frailty. The correlation between the variables frailty and performance of IADL found that among the elderly women independent for the performance of these activities, 47 (67.1%) did not have frailty, 12 (17.1%) were apparently vulnerable to frailty, and 11 (15.7%) had mild frailty. It should be noted that no independent elderly women presented higher levels of frailty. Therefore, one can infer that the higher the level of independence in IADL, the lower the degree of frailty, according to Table 3.
TABLE 3: Distribution of the elderly women according to frailty and performance in
activities of daily living. João Pessoa, PB, Brazil, 2011 (N=166).
The mentioned situation is corroborated by the findings of this study, as it was found a greater association between frailty and performance in ADLs (p <0.0001). It is noteworthy that deficits in the ability to perform ADLs are usually associated with frailty24. This is explained, in particular, because it is related to the individual's ability to remain in the community, enjoying independence until an older age. In this sense, the promotion and maintenance of functional capacity in the elderly result in better quality of life and successful aging.
Considering these aspects, a study13 reinforces the importance of considering the multidimensionality of the phenomenon as it states that, in addition to social factors such as insufficient income, low education level, lack of social support and lifestyle, the clinical variables, such as the existence of morbidities and impaired functional capacity, may aggravate the pathophysiology of frailty. Moreover, authors assert that appropriate interventions on these factors and variables point to the possibility of reversing the event. It should be stressed that the main goal of elderly care is the maintenance of the independence and autonomy for their basic activities of daily life, which can be directly related to quality of life25.
CONCLUSION
The research in question made it possible to estimate the prevalence of frailty in older women living in the city of João Pessoa (Paraíba), and its association with morbidities and functional capacity. This contributed to deepen the analysis of epidemiological aspects and factors related to the frailty.
Considering the findings, the elderly women with higher levels of frailty were those who self-reported suffering from at least one morbidity, especially cardiovascular and neurological, and had impaired functional capacity. Based on the results and the observed associations, one can infer that the phenomenon investigated has a multifactorial nature, which can be understood as a natural outcome of the physiological process of aging or of the decline of biological resilience enhanced by qualifying social conditions of those who show such a problem.
However, it is imperative to point out that this study presents a transversal character of observation of data and, therefore, it cannot determine a causal network for frailty, which is a limitation.
Given the above, this study is a significant contribution to the scientific community, particularly to a better understanding of frailty as experienced by women, as it provides knowledge of some risk variables to frailty in older women, in order to prevent the occurrence of the problem and of adverse outcomes and undesirable results, such as disability and worsening of health conditions of elderly people associated with it, and enables the establishment of preventive measures and screening of the event among older women.
REFERENCES
1. Veras R. Envelhecimento populacional contemporâneo: demandas, desafios e inovações. Rev Saude Publica. 2009; 43:548-54.
2. Instituto Brasileiro de Geografia e Estatística (IBGE) Departamento de População e Indicadores Sociais [internet]. Censo Demográfico 2010. [cited 2015 Nov] Available from: http://www.ibge.gov.br
3. Carvalho CMRG, Brito CMSB, Sampaio IN, Fortes MLF. Prevenção de câncer de mama em mulheres idosas: uma revisão. Rev Bras Enferm. 2009; 62:579-82.
4. Fernandes MGM, Garcia LG. O corpo envelhecido na percepção de homens idosos. Rev Bras Enferm. 2011; 64:472-7.
5. Gallucci M, Ongaro F, Amici GP, Regini C. Frailty, disability and survival in the elderly over the age of sevently: evidence from the trevisolongeva study. Arch Gerontol Geriat. 2008; 5:281-3.
6. Fried L, Ferruci L, Darer J. Untangling the concepts of disability, frailty, and comorbidady: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. 2004; 59:255-63.
7. Camargos MCS, Rodrigues RN, Machado CJ. Expectativa de vida saudável para idosos brasileiros, 2003. Ciênc saúde coletiva. 2009; 14:1903-9.
8. Souza EA, Scochi MJ, Maraschin MS. Estudo da morbidade em uma população idosa. Esc Anna Nery. 2011; 15:380-8.
9. Topinková E. Aging, disability and frailty. Ann Nutr Metab. 2008; 52:6-11.
10. Macedo M, Gazzola JM, Najas M. Síndrome da fragilidade no idoso: importância da fisioterapia. Arq brás ciênc Saúde. 2008; 33:177-84.
11. Woo J, Goggins W, Shan A, Ho SC. Social determinants of frailty . J gerontol. 2005; 51:402-8.
12. Fried L, Tangen C, Waltson J, Newman A, Hirsch C, Mecbrunie MA, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001; 56:146-56.
13. Rockwood K. Frailty and its definition: a worthy challenge. JAGS 2005; 53:1067-70. Frailty and comorbidady: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. 2005; 59:255-63.
14. Rolfson DB, Majumdar SR, Tsuyuki RT, Tahir A, Rockwood K. Validity and realibility of edmonton frail scale. Age Aging. 2006; 17:526-11.
15. Fabrício-Whebe SCC, Schiaveto FV, Vendrúsculo TRP, Haas VJ, Dantas RAS, Rodrigues RAP. Adaptação cultural e validade da Edmonton Frail Scale – EFS em uma amostra de idosos brasileiros. Rev Latino-Am Enfermagem. 2009; 17:1043-9
16. Ministério da Saúde (Br). Resolução 196/96. Pesquisa envolvendo seres humanos. Brasília (DF): Ministério da Saúde, 1996.
17. Virtuoso Júnior JS, Guerra RO. Incapacidade funcional em mulheres idosas de baixa renda. Ciênc saúde coletiva. 2011; 16:2541-8.
18. Henrique NN, Costa PS, Vileti JL, Corrêa MCM, Carvalho EC. Hipertensão arterial e diabetes mellitus: um estudo sobre os programas de atenção básica. Rev Enferm UERJ. 2008; 16:168-73.
19. Barros MBA, Francisco PMSB, Zanchetta LM, César CLG. Tendências das desigualdades sociais e demográficas na prevalência de doenças crônicas no Brasil, PNAD: 2003- 2008. Ciênc saúde coletiva. 2011; 16:3755-68.
20. Torres GV, Reis LA, Reis LA, Fernandes MH. Qualidade de vida e fatores associados em idosos dependentes em uma cidade do interior do Nordeste. J bras psiquiatr. 2009; 58(1):39-44.
21. Campolina AG, Dini PS, Ciconelli RM. Impacto da doença crônica na qualidade de vida de idosos da comunidade em São Paulo (SP, Brasil). Ciênc saúde coletiva. 2011; 16:2919-25.
22. Lang, P.O. Frailty syndrome: a transitional state in a dynamic process. J Gerontol. 2009; 55:539-49.
23. Bergman H, Béland F, Karunananthan S, Hummel S, Hogan D, Wolfson C. Canadian iniciative on frailty and aging: developing a working framework for understanding frailty. Gérontol et Soc. 2004; 106:15-29.
24. Siqueira AB, Cordeiro RC, Perracini MR, Ramos LR. Impacto funcional da internação hospitalar de pacientes idosos. Rev Saude Publica. 2004; 38:687-94.
25. Fhon JRS, Fabrício Wehbe SCC, Vendruscolo TRP, Stackfleth R, Marques S, Rodrigues RAP. Quedas em idosos e sua relação com a capacidade funcional. Rev Latino-Am Enfermagem. 2012;20(5):1-8.