(*)One respondent did not answer
ORIGINAL RESEARCH
Predictive symptoms of depression in schoolchildren in different sociodemographic scenarios
Eliege BortoliniI; Rosane Maria KirchnerII; Leila Mariza HildebrandtIII; Marinês Tambara LeiteIV; Marta Cocco da CostaV
I
Nurse, graduated at the Federal University of Santa Maria/ Palmeira das Missões Campus, Rio Grande do Sul, Brazil.
Email:
eliegebortolini@hotmail.com
II
Ph.D. in Electrical Engineering – Methods of Decision Support. Professor at
the Federal University of Santa Maria/ Palmeira das Missões Campus, Rio Grande do Sul, Brazil.
Email: rosanekirchner@gmail.com
III
Nurse, Master's Degree in Psychiatric Nursing. Professor at the Federal
University of Santa Maria/Palmeira das Missões Campus, Rio Grande do Sul,
Brazil. Email:
leilahildebrandt@yahoo.com.br
IV
Nurse, Ph.D. in Biomedical Gerontology. Professor at the Federal University
of Santa Maria/Palmeira das Missões Campus, Rio Grande do Sul, Brazil.
Tutor of the PET Nursing Group UFSM/Palmeira das Missões Campus.
Email: tambaraleite@yahoo.com.br
V
Nurse, Ph.D. in Nursing. Professor at the Federal University ofSanta Maria/Palmeira das Missões Campus,Rio Grande do Sul, Brazil. Email: marta.c.c@ufsm.br
DOI: http://dx.doi.org/10.12957/reuerj.2016.6680
ABSTRACT
Objective: to examine symptoms predictive of depression in children at public and private schools, particularly by different sociodemographic scenarios. Method: this is a transverse, quantitative, descriptive study. Participants were 126 teenagers at one public and one private school in Rio Grande do Sul State, Brazil, in 2012. Data were collected using the Children's Depression Inventory and a sociodemographic questionnaire. Data analysis was based on descriptive statistics (chi-square), assisted by the Statistical Package for Social Sciences. Results: the results indicate significant percentages of symptoms predictive of depression in teenagers in grades 6 to 8 (17.5%), occurring more frequently in public school students. Conclusion: it was concluded that the depression in children and teenagers forms part of school life, requiring that people directly involved with schoolchildren be alert to symptoms of depression, in order to reduce the occurrence of depression and to construct prevention strategies and improve these individuals' quality of life.
Keywords: Infantile depression; school performance; educational practice; nursing.
INTRODUCTION
Currently, the concern about the issue related to mental health is growing, including depression. This is justified because there is an increase of people suffering from this disease, with individual, social, professional and family consequences. Estimates indicate that by 2020, depression will be the second highest incidence disease among the population in general 1. The Ministry of Health estimates that 10% to 20% of children and adolescents suffer from mental disorders. Of this total, 3% to 4% require intensive care2.
The depressive disorder comprehends a set of signs and symptoms including sleep reduction, lack of appetite, feelings of guilt persistent for weeks or months and that represent a marked deviation in the normal performance of the individual. The origin of the disorder could be in childhood or old age, but it affects all age groups3. Child depression consists of a disturbance involving biological, psychological and social aspects and is not a recent issue. The first reports of symptoms of depression and depression in children emerged in the seventeenth century. The condition is characterized by crying, feeding refusal and difficulty in school learning4.
The diagnosis of child depression was only accepted from the twentieth century, after the IV Child Psychiatry Congress of the European Union, which took place in Sweden in 1970. Until then, it was understood that the child, due to the immaturity of personality structure would not have the mental capacity to develop depression4. Stressful factors and repetition of failure situations are situations that directly affect the children behavior and may contribute to the emerging of symptoms and depressive thoughts in children5. Considering the aspects hitherto pointed this research aimed to verify predictive symptoms of depression in students from public and private schools, according to the different socio-demographic scenarios, in a city in the northern region of Rio Grande do Sul/Brazil.
LITERATURE REVIEW
The attention focused on the mental health of children and adolescents and its recognition as a matter of health and public health, is recent. It is considered a discovery field. Currently, the number of studies that take into account the care aimed at children and adolescents and its relationship with health services is reduced. The development of research with this focus is important because of the contemporary of the theme and also contribute to the production of mental health care, especially directed at children and adolescents6.
Health services have been faced with changes in the form of health care of children and adolescents, and this occurs due to the significant increase of the population in this age group seeking assistance, also involving situations of psychological distress. Children and youth mental health services should assume a social function that runs through the technicality, and that stands in actions such as welcome, listen, care and improve the quality of life of the subject of mental suffering. Also, it is important to consider this as a subject with rights and singularities 2.
Any action aimed at the mental health of children and adolescents need to connect with other public policies such as social work, education, culture, sports, human rights and justice. One can not also fail to establish interfaces with sectors of the society that provide relevant service in this area2. In this context, the school is included as a privileged locus of identification of health diseases, including aspects of mental health.
When depression is mentioned in children and adolescents, it is emphasized the same influence on school performance and the interrelationships because they solidify the personal, emotional and social relationships at school 5. Thus, it is emphasized that the incidence of emotional problems is frequent, specifically depression, in school children and are usually associated with other behavioral difficulties. Considering these aspects, this population stratum may have school performance below expectations and, consequently, decreased school performance7.
It is noteworthy that cognitive functions such as attention, concentration, memory and reasoning are altered in the depressed child, with a negative effect on school performance. Thus, they have difficulty in performing tasks and shows disinterest to carry out the activities, interfering with learning3. Thus, mental health problems in childhood and adolescence may be associated with risk of psychosocial disorders in adulthood8.
METHODOLOGY
This is a descriptive, cross-sectional and quantitative study, and all students of 6th, 7th and 8th grades of two schools participated, one public and the other one private, located in a municipality in the northern region of Rio Grande do Sul, Brazil. They are a total of 126 adolescents of both sexes, aged between 12 and 17 years old. The inclusion criteria were students between the ages of 12 to 18 years old, enrolled and attending classes. It is important to mention that this study considered adolescent students who are in the age group 12-18 years old, according to the Statute of Children and Adolescents, Law Number 8.069/909.
A socio-demographic questionnaire elaborated by the researchers was used for data collection. Also, the Children's Depression Inventory (CDI) was used, developed by Kovacs in 1992. It has been translated and validated for Brazil by Gouveia et al10, to assess emotional, cognitive and behavioral depression symptoms in children and adolescents aged 7-17 years old. This instrument was constructed from an adaptation of Beck Depression Inventory, used for adults.
The original inventory consists of 27 items and has been used in epidemiological, international and Brazilian studies. The CDI consists of 20 items; each item has three alternative responses, and the correction varies on a scale of 0 (no symptom), 1 point (mild symptoms) and 2 points (worsening symptoms). The cut off point is 17 so that children and adolescents with equal scores or more than 17 points should receive greater attention because this result indicates depressive symptoms10.
Thus, the CDI is a self-report inventory to identify changes: affectivity (lowered mood, loneliness and irritability); cognitive (negative self-image, self-blame, negative expectations in decision); motivational (reclusion, avoidance, suicidal idea); vegetative and self-evaluative (disturbance of sleep and appetite); psychomotor and other interpersonal conduits11.
The socio-demographic questionnaire includes the variables: education, age, gender, socio-cultural context, interpersonal relationships and extracurricular activity.
The application of instruments was conducted in July and August 2012, collectively, in the classroom with the students, after signing the informed consent by parents. The study project was approved by the Research Ethics Committee of the Federal University of Santa Maria/RS, under the advice embodied in 37284.
For data analysis, the descriptive statistics, chi-square test and Fisher's exact were used with the help of software - Statistical Package for Social Sciences (SPSS) Version 13 for Windows.
RESULTS AND DISCUSSION
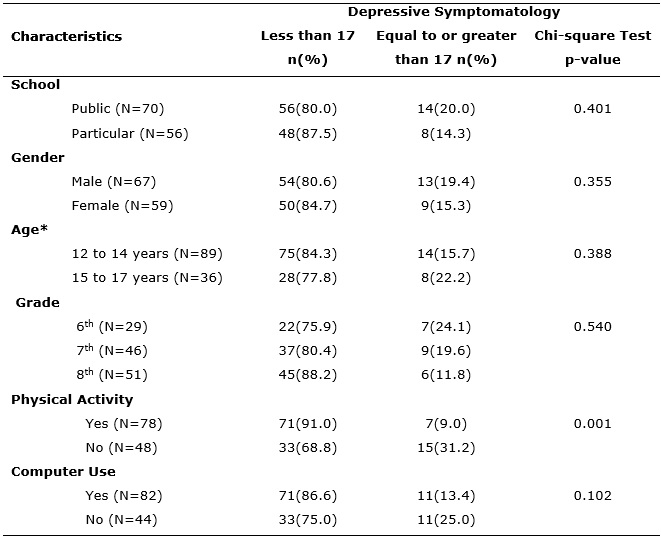
Of the 126 surveyed students, 70 (55.6%) from the public school and 56 (44.4%) from a particular institution. Of the total, 59 (46.9%) are female and 67 (53.1%) male. The girls (61.4%) are more numerous in public schools while the particular schools were dominated by boys (57.1%). When analyzed the school's nature in which respondents are bound, related to suggestive symptoms of depression (score above or equal to 17), it is evident that they occur in greater numbers in public schools, accounting for 20%, while in particular are 14.3%. This may be related to characteristics such as low socioeconomic status, social disadvantage and family stress, which are social determinants that negatively influence the health of children and adolescents12.
As for education, 51 (40.5%) attend the 8th grade, and 59.5% are in the 6th or 7th grades. The age group of adolescents is between 12 and 17 years old, and 71.2% are between 12 and 14 years old and 28.8% from 15 to 17 years old. Concerning age group, it is identified that the predictive symptoms of depression are more significant in adolescents between 15 and 17 years old. Also, it is observed that students who have scores greater than or equal to 17 are at a higher percentage in the 6th grade of elementary school, decreasing in 7th and 8th grades. See Table 1.
TABLE 1:
Participants distribution, according to socio-demographic data and presence
or absence of depressive symptoms. Palmeira das Missões, RS,
Brazil, 2012.
(*)One respondent did not answer
In a study of the prevalence of depressive symptoms, which used the CDI with 519 students aged 7-13 years old, identified that 13.7% of them had depressive symptoms, indicating that a significant number of children and adolescents probably had depression13.
The results of the CDI show that 22 (17.5%) adolescents have a score equal to or above the cut off point 17, which is indicative of depressive symptoms. Table 1 shows the analysis results of the presence or absence of depressive symptoms, relating to the socio-demographic data. It is evident that the students of the research, with an indicative of depressive symptoms, had the highest percentage of students related to public school, boys and those aged from 15 to 17 years old.
When depressive manifestations are related to physical activity, it appears predominance among those who do not perform activity - 31.2% - those with indicative of depressive symptoms. Also, with the chi-square test, a significant relationship is found (p<0.001) between the practice of physical activity variables and absence of predictive symptoms of depression. It is important to emphasize that people who practice physical exercise are less likely to develop depressive symptoms because this activity increases serotonin levels in the brain. This effect was found for all forms of regular exercise. The depletion of serotonin leads to irritability and anger while its supplementation can relieve anxiety and increase feelings of well-being3. Concerning the frequent use of the computer, it appears that it does not have significant influence over the probable depressive symptoms.
The inventory of childhood depression has 20 questions, and each one has three choices for symptoms in the last two weeks. Thus, the responses of the subject to this inventory containing three options – the absence of predictive symptoms of depression, mild symptoms and worsening - on each item, are distributed in Table 2.
TABLE 2:
Frequency of symptoms of depression on each of the questions of the
Inventory of Child Depression. Palmeira das Missões, RS, Brazil,
2012.
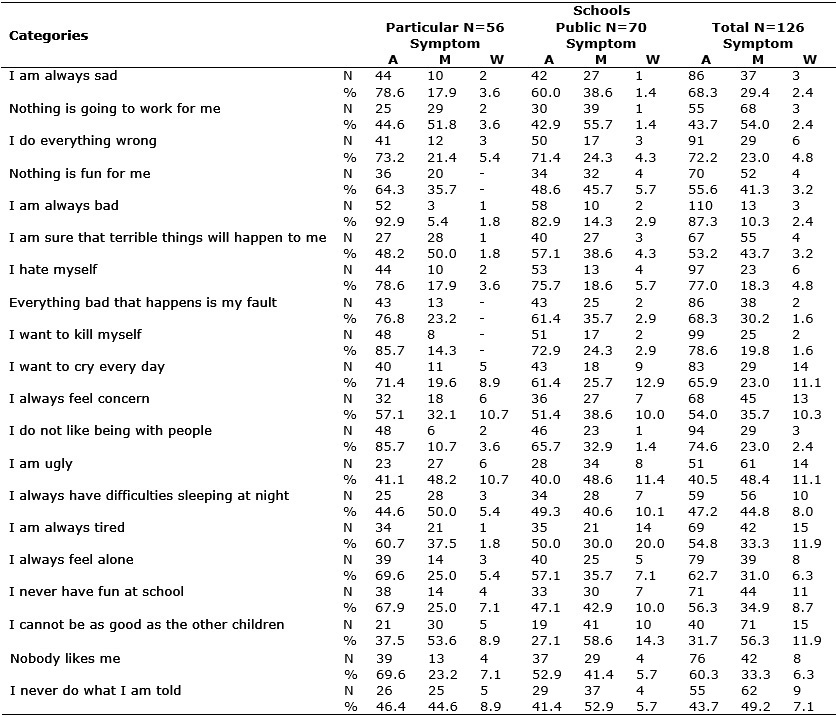
A: absence; M: Mild; W: worsening
Predictive depression symptoms presented by the investigated group are in agreement with the employee manual contents in the diagnosis of mental disorders, which highlight as depressive symptoms - depressed mood, most of the day, decreased interest in daily activities, sleep and appetite changes, lack of energy, changes in motor activity, feelings of worthlessness, difficulty concentrating and thoughts and/or suicide attempts14.
It is noticed that in the total of predominant subjects responses concerning the presence of the predictive symptom of depression worsening was – I am always tired, I cannot be as good as the other children, I want to cry every day, I always feel concern, and I am ugly -, ranging between 10 and 12% of students. It is worth noting that the prevalence of public school students was identified in all categories.
Still, making a parallel between the schools, it appears that when performed the sum of the percentage of students who have mild or worsening indicative of depression, there is a value greater than 50% in both institutions in the categories Nothing is going to work for me, I am ugly, I always have difficulties sleeping at night, I cannot be as good as the other children and I never do what I am told. The category I am sure that terrible things will happen to me reached 50% of private school students. See Table 2.
The categories I am always sad,Nothing is going to work for me, I am always bad,Everything bad that happens is my fault,I want to kill myself, and I do not like being with people are predictive symptoms of depression, however, were less evident in the studied population. However, it should be pointed out that the categoriesNothing is going to work for me, I am ugly,I cannot be as good as the other children, and I never do what I am told, stand out as mild symptoms, and were identified by more than 48% of research subjects.
Depressed mood, loss of interest or pleasure, sadness, depreciation and antisocial behavior are the key symptoms of depression3. These characteristics were not the most marked in the questionnaire by the adolescents in the study, which may be associated with the fact that they are inserted in the school environment.
From this perspective, we must highlight the importance of social relationships between people, especially between members of related groups. The event feeling rejected by colleagues and friends was significant, indicating that can be considered a predictor of depressive symptoms. Also, the adolescent's dissatisfaction with the received family support may influence the emergence of such events.
It is agreed on the importance of the social group during the development of children and especially adolescents. Experts recommend immediate intervention with students with probable depressive symptoms. Thus, it is possible to prevent the scores increasing along and also reduce symptoms already submitted15.
The less the adolescent likes to go to school, the greater the possibility of developing depressive symptoms, which is found in this study in the category I detest, where 50% of respondents have predictive symptoms of depression. See Figure 1.
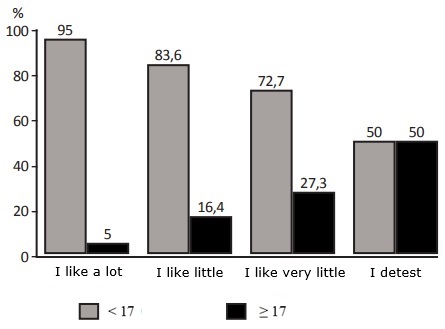
FIGURE 1:
Symptoms of depression, cut off point 17, according to student satisfaction
to go to school. Palmeira das Missões, RS, Brazil, 2012.
In this line, the study shows that the influence of the school on adolescents is positive and may constitute a preventive factor in the emergence of depressive symptoms15. The school has a significant role in socialization and the development of cognitive skills of this age group, favoring the understanding of the social world. It is necessary to develop pedagogical practices of pleasure, making students feel comfortable going and being at school16.
Regarding the action of the school and the professionals who were working on it, it highlights its importance in identifying symptoms indicating depression and the development of psychosocial and pedagogical actions, curricular and extracurricular, aimed at the prevention of this disease and the formation of citizens able to socially interact17.18. Also, the educational system has the function to reduce the stigmas related to prejudices and taboos18, including depression, as commonly understood that this pathology is not part of everyday life of children and adolescents.
In addition to the school, it is understood that the professionals in the primary health care must also insert adolescents into their care programs. Thus, it is considered that in the health agenda and planning of care actions, is contemplated that portion of the population, which has particularities and various health risks18. Therefore, it is up to school with other social sectors to rescue capabilities of the individual, strengthening and encouraging decisions that contribute to the physical and mental health of this population stratum19.
CONCLUSION
As depression often occurs among children and adolescents, it is important to conduct studies that seek to identify early predictors of depression symptoms. Also, there is the effectiveness of measures for the promotion of mental health and prevention of disease, also in the educational system.
The results of this study allow verifying the presence of predictive symptoms of mild depression and its worsening in a significant number of adolescents. Most students with predictive symptoms of depression studies in public school, are male and aged from 15 to 17 years old. Also, among those who do not perform physical activities, was indicative of depressive symptoms.
The study has some limitations because the CDI is a tool that helps to identify children and adolescents with depressive symptoms and ask for an adolescent to select the best alternative that describes their feelings in the past two weeks is a complex task. Thus, there is the importance of parents, educators and health professionals, particularly nurses, to be attentive to the manifestations of children and adolescents, contributing to the early diagnosis of symptoms indicating depression.
It is important to develop programs to promote health and disease prevention and especially for interventions in the mental health area, with children and adolescents. We must build care strategies and well-being for those who have suggestive symptoms of depression. Reinforces the presence of the nurse in this context, can contribute to the health of this population group.
REFERENCES
1.Nakamura E, Santos JQ. Child depression: an anthropological approach. Public Health Magazine 2007; 41:53-60.
2.Ministry of Health (Br). Ways to a Children and Youth Mental Health Policy. Brasília – DF, 2005.
3.Sadock BJ, Sadock VA. Psychiatry compendium: behavioral sciences and clinical psychiatry. 9Th edition. Porto Alegre: Artmed; 2007.
4.Lacerda ALT, Quarantini LC, Miranda-Scippa AMA, Del Porto JA. Depression: from the neuron to the social functioning. Porto Alegre: Artmed; 2009.
5.Barbosa GA, Lucena A. Child depression. Infant: Neuropsychiatry Infant Adolescent Magazine 1995; 3: 23-30.
6.Delfini PSS, Reis OA. Coordination between public health services in care focused on children and youth mental health. Cad. Public Health 2012; 28: 357-66.
7.Cruvinel M, Boruchovitch E. Child depression: a contribution to educational practice. School and Educational Psychology 2003; 7: 77-84.
8.Mendes AV, Loureiro SR, Crippa JAS. Maternal depression and mental health of students. Clinical psychiatry Magazine 2008; 35: 178-86.
9.Brazil. Law n. 8.069, 13th July 1990. It provides about the Statute of Children and Adolescent and gives other measures. Brasília; 1990.
10.Gouveia VV, Barbosa GA, Almeida HJF, Gaião AA. Children Depression Inventory – CDI: adaption study with students of João Pessoa. Brazilian psychiatry journal 1995; 44: 345-9.
11.Pereira DAP, Amaral VLAR. Depression rating scale for children: a validation study. Psychology Studies Magazine 2004; 21: 5-23.
12.Assis SG, Avanci JQ, Oliveira RVC. Socio-economic inequalities and children mental health. Public Health Magazine 2009; 43: 92-100.
13.Fonseca MHG, Ferreira RA, Fonseca SG. Prevalence of depressive symptoms in students. Pediatrics 2005; 27: 223-32
14.American Psychiatric Association. DSM-IV TR: Diagnostic and statistical manual of mental disorders. 4th edition. Porto Alegre: Artmed; 2002.
15.Abaid JLW, Dell'aglio DD, Koller SH. Predictors of depressive symptoms in children and adolescents institutionalized. Univ. Psychol. 2010; 9: 199-212.
16.Martins SVM, Tavares HM. The family and the school: challenges for education in the contemporary world. Catholic Magazine 2010; 2: 256-63.
17.Monteiro FR, Coutinho MPL, Araújo LF. Depressive symptomatology in high school adolescents: a study of social representations. Psychology, Science and Profession 2007; 27: 224-35.
18.Costa RF, Queiroz MVO, Zeitoune RCG. Adolescent care: nursing contributions. Nursing Magazine UERJ 2012; 20:197-202.
19.Ribeiro KCS, Nascimento ES, Coutinho MPL. Social representation of depression on a public educational institution. Psychology, Science and Profession 2010; 30: 448-63.