REVIEW ARTICLES
Clinical validation of diagnoses, interventions and nursing outcomes: narrative literature review
Ana Railka de Souza OliveiraI; Alice Gabrielle de Sousa CostaII; Julyana Gomes FreitasIII; Francisca Elizângela Teixeira LimaIV; Marta Maria Coelho DamascenoV; Thelma Leite de AraujoVI
INurse Student, Graduate Program in Nursing - Phd level. Federal University of Ceará. Ceará, Fortaleza, Brazil. E-mail: railkaufc@yahoo.com.br
IINurse. Student, Graduate Program in Nursing - Phd level. Federal University of Ceará. Ceará, Fortaleza, Brazil. E-mail: alice_gabrielle@yahoo.com.br
IIINurse. Student, Graduate Program in Nursing - Phd level. Federal University of Ceará. Professor for the University of Fortaleza. Ceará, Fortaleza, Brazil. E-mail: julyanapitt@yahoo.com.br.
IVNurse. Phd in Nursing. Professor for the Graduate Program in Nursing. Federal University of Ceará. Ceará, Fortaleza, Brazil. E-mail: felisangela@yahoo.com.br.
VNurse. Phd in Nursing. Professor for the Graduate Program in Nursing. Federal University of Ceará. Ceará, Fortaleza, Brazil. E-mail: martadamasceno@terra.com.br.
VINurse. Phd in Nursing. Student, Graduate Program in Nursing - levels Masters/Phd. Federal University of Ceará. Ceará, Fortaleza, Brazil. E-mail: thelmaaraujo2003@yahoo.com.br.
ABSTRACT
The study aimed to evaluate the clinic validation process of diagnoses, interventions and nursing outcomes. Two articles, six master dissertations and eight PhD theses were selected, fourteen of which corresponded to researches on diagnoses and two were about Nursing Outcomes. The outlines of the studies and analysis are still fragile aspects. Regarding identified methodological references, Fehring’s validation model was the most used. The clinical validation step was predominantly performed by expert nurses. The importance of completing the pilot test, using a gold standard as well as the use of different statistical tests is emphasized. Despite methodological differences the authors emphasized need for further validations with larger and different populations. It is concluded that the clinical validation step is critical, although there is no uniform methodological approach with regard to the studies followed. It is necessary to develop and improve the taxonomies and their components.
Keywords: Validation studies; classification; terminology; nursing
INTRODUCTION
The nursing process is a conceptualized tool, recognized and widely applied in the systematization of human care, therefore enables the nurse to organize and manage the nursing care. The goal is to promote the humanized action, directed at the results, in addition to boosting the professional the constant evaluation of their practice differentiating their actions from those of other professionals. It consists of five inter-related steps: Investigation, Diagnosis, Planning, Implementation and Evaluation1,2.
In the meantime, the nursing classification systems and their taxonomies are fundamental to organize and improve the communication of nursing practices and, therefore, must be clinically useful and applicable3. Therefore, it is believed that there is a broad and necessary space for research on clinical validation in this context.
Thus, arose the following question: What studies have been developed involving clinical validation of taxonomies NANDA- International (NANDA-I),Nursing Intervention Classification (NIC) and the Nursing Outcomes Classification (NOC) in Brazilian Graduate Degree Programs Stricto Sensu?
This study aimed to evaluate the validation process for clinical diagnoses, interventions and nursing outcomes in literature.
THEORETICAL REFERENTIAL
For the use of the nursing process it is necessary that the nurses have their own language and uniform. This uniformity serves several purposes, among them: provides a language for the nurses to communicate what they do; facilitates the evaluation and improvement of nursing care and accelerates the development of knowledge in the profession4.
Thus, for its realization, it requires the use of their own taxonomies, such as the NANDA-I5, to define the nursing diagnosis (ND); the NIC6, for nursing interventions; and the NOC7, for the nursing outcomes.
These classifications, in turn, contain concepts to be studied more depth and validated, which is why the validation process is essential in order to perfect them and legitimate them, with a view to generate an entrepreneur knowledge and the possibility of applying it in the daily life of the professional who produces them8,9. In this context, different types and methods are involved, but little is yet known such as the validation process for the elements of Taxonomy NANDA-I/NIC/NOC (NNN) as it is focused on in Brazilian literature.
It is noteworthy that the clinical validation objective, tests if the list of developed taxonomy components in the concept analysis and validates them by a group of specialists and supports them by clinical data10. An important step to be considered is to clearly describe each diagnostic component, that is being tested, and, if possible, build operational definitions for each component indicating what and how it will be assessed11. Such procedures also apply to the nursing interventions and outcomes.
In addition, it is necessary to summarize essential data as adopted methodological characteristics, found statistical evidence, limitations and recommendations of the authors, to guide the future researchers in the clinical validation process.
METHODOLOGY
It is a literature narrative review study, which consists of the presentation of new information to provide current knowledge on the topic explored or highlight gaps in the body of research, and thus instigating researchers to improve the basis of scientific data12.
To search the publications which occurred in the months of April and May 2011, in two ways: access to the catalogs of dissertations and theses from the Center for Studies and Research of Nursing (CEPEn); and access online the Public Domain Portal, Theses Database Coordination for Improvement of Personnel with Higher Education (CAPES) and Brazilian Digital Library of Theses and Dissertations (BDTD). This focuses on works published from 1990 onwards, which is considered the period in which the production on validation of Taxonomy NNN begsn13, until the year 2011. It was preferred to search information on theses and dissertations in view having more details regarding on the methodological steps covered.
For the completion of the study, the following steps were performed: a survey of all the CEPEn catalogs by the reading of all the titles, descriptors and keywords; consultation in all virtual libraries of the Stricto Sensu graduate programs of Brazil recognized by CAPES. The virtual library search was made by means of the following keywords: validation studies, nursing diagnoses, nursing interventions, nursing outcomes, nursing care and nursing assessment.
This search then yielded 14 publications, whose titles and abstracts were read in full. The inclusion criterion was related to the clinical validation of any component of the NNN Taxonomy. It was observed that the same criterion in the search for articles, having been located two texts. Thus this study examined 16 publications.
Subsequently, a synoptic table was built, which appreciated the following relevant aspects: author; year; type of study; methodological referential; validated taxonomy component; selection criteria from experts, target population and sample calculation, statistical analysis and methodological steps.
The presentation of the results and discussion of the data obtained were made descriptively, by enabling the applicability of the prepared review and provide subsidies to the nurse in decision making regarding the clinical validation course of the NNN taxonomies. The analysis is supported in the literature on the topic13,41.
RESULTS AND DISCUSSION
There were two articles, six dissertations and eight theses analyzed, of which 14 corresponded to work on the diagnostics submitted by NANDA-I and two studies on the nursing outcomes contained in the NOC. Of the total, 11 studies were developed in the post-graduate programs in nursing from the southeast region, three from the northeast region and two from the southern Region. As for the time of the study’s completion, there was a growing trend in the 1990s to 2000. This may have occurred due to the expansion of graduate programs in nursing in the 1990s.
As other research in the area, the nursing taxonomy validation studies in Brazil had their dissemination started in 1992 and constitute a growing trend, possibly due to the concern of researchers with the degree of representativeness of standardized languages and classification systems on patient problems13,14.
The preference for development work on the components of ND is emphasized at the expense of other steps and their respective taxonomies 13,14 .
The literature suggests the importance of clinical validity and clarifies that checking if a diagnosis is clinically valid means assessing if it really represents the behaviors and characteristics of the patient 15. This concept can be adapted to other nursing classification system components.
According to studies, the issue of developing and improving these elements, especially investments in the area of validation, is justified by the fact that it is a necessary tool to substantiate the clinical practice of nurses, to subsidize an improved quality in care16-22.
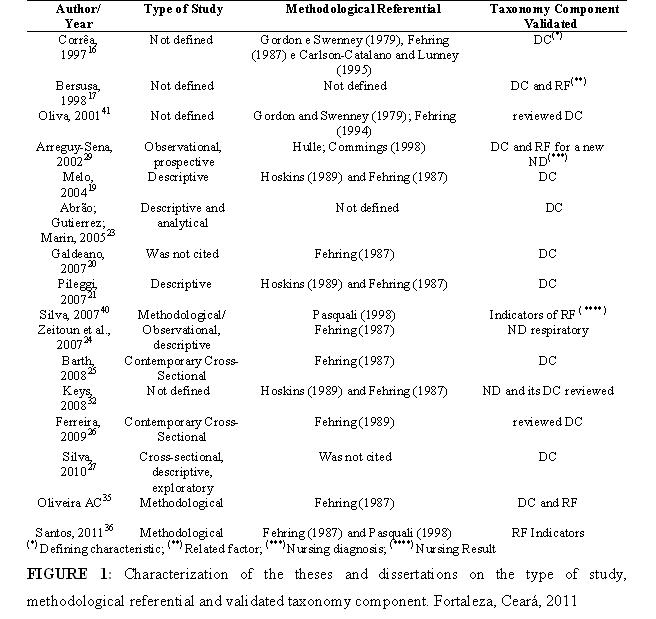
When evaluating the outlines of the studies and data analysis, it is emphasized that these are weak points in several studies, because they are common descriptive studies19.21,27, despite the need for an experimental approach and the use of more consistent technique analyses28. Only one study has developed a cohort type study to assess the presence or absence of defining characteristics (DCs) for the new ND that was being suggested29. As seen in Figure 1.
In clinical research, cohort has as main objectives: to describe the incidence of certain outcomes and to examine associations between the predictors and outcomes. Thus, the researcher defines the sample and measures the predictive variables before the outcome. This design is a powerful strategy to investigate the potential causes of a clinical condition30.
According to the emphasized, the most accurate way of studying a diagnostic test is to conduct a clinical trial, in which subjects are randomly assigned to receive the test or not. However, there may be some practical and ethical barriers to the development of such tests being provided care is taken on possible biases and confounding, observational studies on these issues may be useful31. As for the methodological approach, five studies have used only the validation model of Fehring, which also was adopted in conjunction with other, such as Fehring/Hoskins, Fehring/Goordon, Goordon; and Sweenwy /Fehring/Catalano , Fehring/Pasquali, Lunney, according to the Figure 1. This probably occurred because the Fehring validation model is quite typical for diagnostics. Such reference is considered by many as complex, however, quite reliable since its precepts are respected.
This methodological diversity makes the replication of validation studies difficult14. However, it is noteworthy that, currently, the combined use of these references have been frequent in Brazilian researches on validating taxonomies19,21,32.
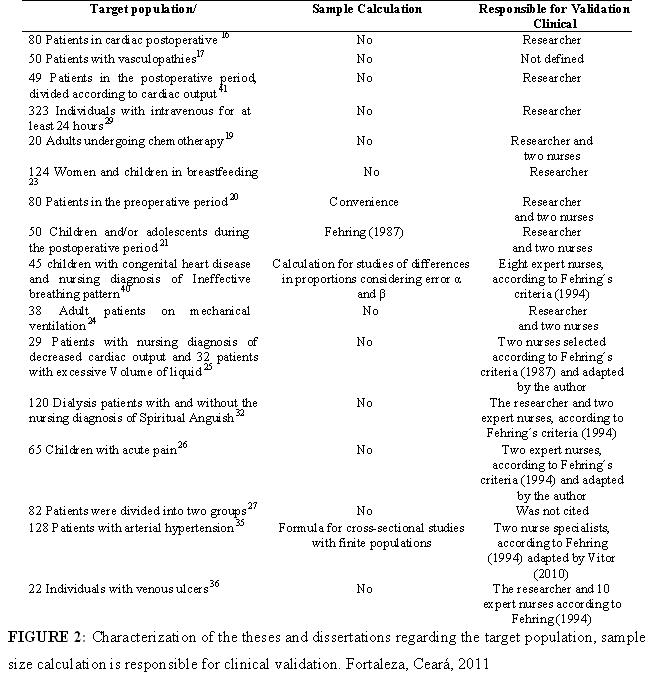
To evaluate who executed the clinical validation step, as observed in Figure 2 that the selection of expert nurses was the least followed. This can become a difficult step to be fulfilled, because in addition to the scarce literature on the definition of experts, there is also the barrier related to training and the professional improvement of nurses. Criteria for selection ofexperts not suitable or not respected may limit studies and interfere with the reliability of the results15.33.
Thus, the scoring system, proposed by Fehring34 for the selection of experts, with views on the diagnostic validation, has been employed. However, in some situations, this system makes it difficult to be met. Faced with this impasse, the researchers only partially adopt such criteria25,26,35,36.
This is due to the fact that in Brazil there is small number of specialist nurses in a given area and also by the small number of those which use ND in clinical practice14.28.
Despite this significant barrier, in the face of the insufficiency ofexperts with a high degree of entitlement, it was observed in three studies the preference for using experts with more experience because their expertise can contribute more significantly to the improvement of the validity studies of NNN taxonomies19-21.
Also it has been difficult to select the population samples in clinical validation studies, because to be able replicate and compare the validation models large samples and standardization of data bases are necessary, as shown in Figure 2. This aspect is a challenge, because it is complicated to differentiate between the subjects that present the diagnosis in study and those who do not, because in many cases the characteristics of both seem to be similar37.
Therefore, the clinical validation has shown distinct sequences of steps in national studies: sometimes the data collection is done directly with the patient in the search for the clinical diagnosis evidence in study, preceded by a bibliographic review of DCs of the aforementioned diagnosis; sometimes the bibliographic search and definition of these are developed prior to the patient’s examination. This sequence has been the most used in recent studies38.
For clinical validation, Fehring11 proposes two possible approaches, according to the nature of the diagnosis to be analyzed. If it relates to a physiological response, direct observation is the most appropriate. If the diagnosis involves a more cognitive or affective response; it is recommended to obtain the information directly from the subject-patient. However, a combination of these two approaches is recommended when the diagnostic indicators cover both objectives as subjective.
In the direct observation approach, first, two nurse specialists evaluate a given number of patients with the predetermined diagnosis which is being tested; second, for each of the patients observed, the two specialists, individually, verify the presence or absence of the diagnosis components, i.e. DCs and related factors (RFs), assigning scores; calculate the reliability coefficient among the specialists for each component11.
In the patient-focused approach, first a sample is obtained with the diagnosis of interest; second, it should confirm whether the allocation of the diagnosis was correct, through the validation performed by a specialist nurse in the area; third, develop a list of DCs and RFs of the diagnosis, which is being tested, and requested the patient to evaluate how these components are indicative of their feelings or behaviors, by assigning a grade11.
For analysis of this step, Hoskins 10 recommends the assessment according to the Ferhing’s proposed model11. And the validation example by a specialist, is the calculation of scores for each indicator (weighted average) to assess the frequency of occurrence in the population and the representativeness in the clinic, and then classifies them as primary, secondary and irrelevant. These steps were also followed for the validation of the nursing outcome indicators39.
In three studies, the completion of a pilot study was also noted to improve the designed instrument19,21,3. The pre-tests and pilot studies are designed to assess feasibility, efficiency, and cost of study methodologies, reproducibility and accuracy of measurements, likely rates of recruitment as well as estimates of outcome and magnitude of effect or association31.
It is also necessary, to choose the clinical gold standard to determine if a patient has or not the disease or outcome in study, as evidenced in Figure 331. Such procedures were common in four studies that used scales or apparatus to demonstrate the presence of ND or the assessment of the patient or even the trial from a third evaluator or the patient16,24,32,35,39,40.
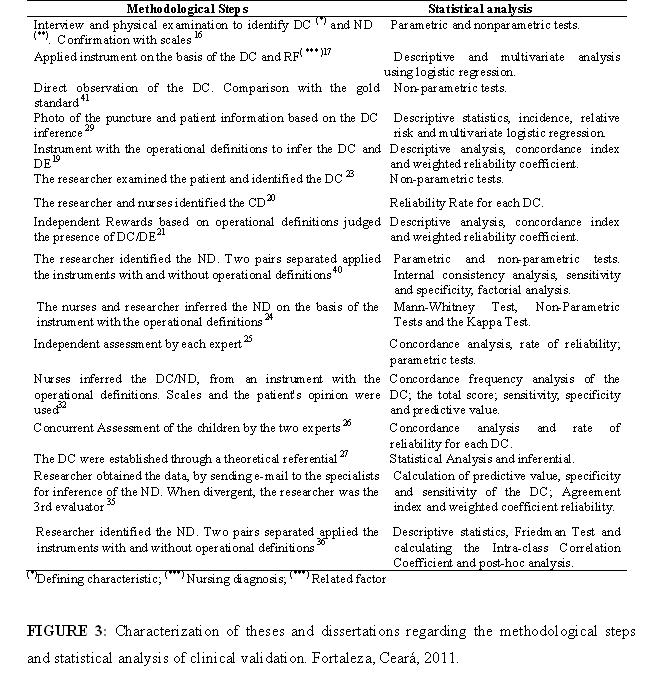
As the statistical approach of the study, it was observed that the evaluation of the percentage or concordance index on the presence or absence of DCs (division between the concordance number for each DC between the two nurse diagnosticians be present and the concordance number were added to the discordance number); Index of total agreement to the ND (sum of all the indices of each DC, by dividing by the total number of DC’S of ND); occurrence frequency of DCs in the studied population (computed by the DCs similar between the two nurse diagnosticians); Weighted reliability coefficient between the observers, according to the formula proposed by Fehring (this formula allows identification of the frequency of each DC, ensuring that a little observed characteristic is considered to be highly evaluated, i.e., it depicts the clinical incidence of the DC corrected by concordance. Such DCs are classified as majors, minors and those which should be highlighted and best studied) and, finally, obtaining the total score calculated by the sum of the coefficients for each DC divided by the number of features, considering the exclusion of some DCs with a score less than 0.50.
The work also employs the Kappa concordance analysis, which measures the degree of inter-observer agreement, beyond what would be expected by the mere knowledge of the “marginal values”, and is important to distinguish between nominal and ordinal variables, because in the latter the Kappa does not capture all the information from the data. In general, measuring the reproducibility, including the variability inter and intra-observer is a good initial step to evaluate a diagnostic test31.
New work has also evaluated the sensitivity, specificity and predictive value of DCs and others have used the multivariate analysis, by means of the logistic regression model. The results of studies on the accuracy of diagnostic tests can be summarized by the sensitivity, specificity, predictive values, the ROC curves and likelihood ratios. Studies on the value of prognostic tests can be summarized by using risk reasons or hazard reasons31.
The nonparametric reliability tests, such as paired t Test, Kruskal-Wallis Test, Mann-Whitney Test, Wilcoxon Test, Chi-square Test and Fisher Test, these studies seek to provide a reliability validation for the results12. The validity can be defined as credibility and is important in the prevention of errors in the diagnosis and also necessary, however, when used alone, does not validate the diagnosis41.
Despite methodological differences, all emphasize the need for new validations with larger populations and different, because the data cannot be generalized16,17,19,21,32,36, and by the need for expert approximation to the patient and population reduction in order to select only individuals already with the ND discussion in35.
As the limitations, the geographical distance between the evaluators and the clinical phase patients is listed; the need to operationally better define the characteristics in a more objective way, offering nurses in care practice the best parameters for the assessment of the elements, in the face of the subjectivity of DC and RF35; reduced number of specialists; biases of observation and evaluation usually present between the evaluator groups; availability to participate in studies; scarce literature results in nursing, which also made it difficult for a broader discussion and comparison between the validation studies36.39.
CONCLUSION
In general, the clinical validation is still seen as a promising factor and essential for research on classification systems as a whole. Various proposals have been identified and some not used any referential methodological for their development, despite the referential proposed by Fehring having been the most adopted in research, in spite of being complex and there is difficulty in identifying and selecting experts. Regarding the type of component, the diagnoses were the most expressive, and major functional and psychosocial domains were the most covered. This may suggest greater concern of researchers with the physical and mental well-being, consistent with the profile of modern society.
However, there is not yet a uniform methodological course in clinical validation studies. Such limitation may complicate the discussion on the reliability of the findings, given that the same indicators are eventually validated for different populations, for example, but by completely different methodological steps. It is understood, however, that NNN validation studies are relatively recent. Therefore, only by conducting more investigations may a methodology be proposed somewhat less methodologically bias.
As noted between the limitations of some authors, to identify the difficulties of previous studies, one will be able to produce a more discerning methodological approach. In this study, was revealed a small number of studies that have failed to portray the current scenario of clinical validation studies developed by the Brazilian scientific community, especially with regard to NIC and NOC Taxonomies, and the unavailability of online works. Furthermore, it was noticed that the studies analyzed in the article category did not present a detailed methodology with a rigorous description of the steps taken.
It emphasizes, therefore, the urgent need to develop new studies on this topic in order to summarize the existing literature productions nationally and internationally. Therefore, it is considered that the classification systems, particularly those represented by NNN Taxonomy need to actually follow the development of the human being and the context around, while trying to cover their needs, achievements and changes.
Given the above, it is concluded that care quality in the direction of human progress includes developing and improving the taxonomies and their components which are increasingly useful, applicable and valid.
REFERENCES
1. Alfaro-Lefèvre R. Aplicação do processo de enfermagem: uma ferramenta para o pensamento crítico. 7ª ed. Porto Alegre (RS): Artmed; 2010.
2. Lira ALBC, Albuquerque JG, Lopes MVO. Perfil dos diagnósticos de enfermagem presentes em pacientes transplantados renais. Rev enferm UERJ. 2007; 15: 13-9.
3. Killeen MB, King IM. Viewpoint: use of king’s conceptual system, nursing informatics, and nursing classification systems for global communication. Int J Nurs Terminol Classif. 2007; 18: 51-7.
4. Johnson M, Bulechek G, Butcher H, Dochterman JM, Maas M, Moorhead S, et al. Ligações entre NANDA, NOC e NIC: diagnósticos, resultados e intervenções de enfermagem. 2ª ed. Porto Alegre (RS): Artmed; 2009.
5. North American Nursing Diagnosis Association- International (NANDA-I). Diagnósticos de enfermagem: definições e classificação 2009-2011. Porto Alegre (RS): Artmed; 2010.
6. Bulechek GM, Butcher HK, Dochterman JM. Classificação das intervenções de enfermagem (NIC). 5ª ed. Rio de Janeiro: Elsevier; 2010.
7. Moorhead S, Johnson M, Maas M. L, Swanson E. Classificação dos resultados de enfermagem (NOC). 4ª ed. Rio de Janeiro: Elsevier, 2010
8. Garcia TR, Nóbrega MML. Processo de enfermagem e os sistemas de classificação dos elementos da prática profissional: instrumentos metodológicos e tecnológicos do cuidar. In: Santos I, Figueiredo NMA, Padilha MICS, organizadores. Enfermagem assistencial no ambiente hospitalar: realidade, questões, soluções. São Paulo: Atheneu; 2004. v. 2, p. 37-63.
9. Napoleão AMA. Estudo da aplicabilidade de intervenções da NIC no atendimento a crianças com o diagnóstico de enfermagem desobstrução das vias aéreas relacionada à presença de via aérea artificial em um centro de terapia intensiva pediátrico [dissertação de mestrado]. Ribeirão Preto (SP): Universidade de São Paulo; 2005.
10. Hoskins LM. Clinical validation, methodologies for nursing diagnoses research. In: Carroll-Johnson RM, editor. Classification of nursing diagnoses. Proceedings of the eighth conference of North American Nursing Diagnosis Association. Philadelphia (USA): JB Lippincott; 1989. p.126-31.
11. Fehring RJ. Methods to validate nursing diagonosis. Heart Lung. 1987; 16:625-9.
12. Polit DF, Beck CT. Fundamentos de pesquisa em enfermagem: avaliação de evidências para a prática de enfermagem. 7ª ed. Porto Alegre (RS): Artmed; 2011.
13. Silva V, Oliveira T, Damasceno M, Araújo T. Languages of the nursing process in the dissertations and theses. A bibliographical study. Online Braz J Nurs. 2006; 55(8). [citado em 25 ago 2011]. Disponível em: http://www.objnursing.uff.br/index.php/nursing/article/view/328/72
14. Chaves ECL, Carvalho EC, Rossi LA. Validação de diagnósticos de enfermagem: tipos, modelos e componentes validados. Rev Eletr Enferm. 2008; 10:513-20.
15. Creason SN. Clinical validation of nursing diagnoses. Int J Nurs Terminol Classif. 2004; 15: 162-9.
16. Corrêa CG. Dor: validação clínica no pós-operatório de cirurgia cardíaca [dissertação de mestrado]. São Paulo: Universidade de São Paulo; 1997
17. Bersusa AAS. Validação do diagnóstico: alteração da perfusão tissular periférica nos pacientes com vasculopatia periférica de membros inferiores. [dissertação de mestrado]. São Paulo: Universidade de São Paulo; 1998.
18. Bachion MM, Araújo LAO, Santana RF. Validação de conteúdo do diagnóstico de enfermagem Mobilidade física prejudicada em idosos: uma contribuição. Acta Paul Enferm. 2002; 15:66-72.
19. Melo AS. Validação dos diagnósticos de enfermagem disfunção sexual e padrões de sexualidade ineficazes [tese de doutorado]. Ribeirão Preto (SP): Universidade de São Paulo; 2004.
20. Galdeano LE. Validação do diagnóstico de enfermagem Conhecimento deficiente em relação à doença arterial coronariana e à revascularização do miocárdio [tese de doutorado]. Ribeirão Preto (SP): Universidade de São Paulo; 2007.
21. Pileggi SO. Validação clínica do diagnóstico de enfermagem Desobstrução ineficaz das vias aéreas de crianças e adolescentes submetidos à correção cirúrgica de cardiopatia congênita [dissertação de mestrado]. Ribeirão Preto (SP): Universidade de São Paulo; 2007.
22. Favretto DO, Carvalho EC. Validação conceitual do diagnóstico de enfermagem comunicação verbal prejudicada. Online Braz J Nurs. 2008; 7(2).
23. Abrão ACFV, Gutierrez MGR, Marin HF. Diagnóstico de enfermagem amamentação ineficaz: estudo de identificação e validação clínica. Acta Paul Enferm 2005; 18:46-55.
24. Zeitoun SS, Barros ALBL, Michel JLM, Bettencourt AR Clinical validation of the signs and symptoms and the nature of the respiratory nursing diagnoses in patients under invasive mechanical ventilation. J Clin Nurs. 2007; 16:1417-26.
25. Barth QCM. Diagnósticos de enfermagem de débito cardíaco diminuído e volume excessivo de líquidos: validação clínica em pacientes com insuficiência cardíaca descompensada [dissertação de mestrado]. Porto Alegre (RS): Universidade Federal do Rio Grande do Sul; 2008.
26. Ferreira AM. Validação do diagnóstico de enfermagem dor aguda em crianças hospitalizadas [dissertação de mestrado]. Porto Alegre (RS): Universidade Federal do Rio Grande do Sul; 2009.
27. Silva RCG. Validação das características definidoras do diagnóstico de enfermagem: perfusão tissular periférica ineficaz em pacientes com doença arterial obstrutiva periférica sintomática [tese de doutorado]. São Paulo: Universidade de São Paulo; 2010.
28. Carvalho EC, Mello AS, Napoleão AA, Bachion MM, Dalr MCB, Canini SRMS. Validação de diagnóstico de enfermagem: reflexão sobre dificuldades enfrentadas pelos pesquisadores. Rev Eletr Enferm. 2008; 10:235-40.
29. Arreguy-Sena C. A trajetória de construção e validação dos diagnósticos de enfermagem: trauma vascular e risco para trauma vascular [tese de doutorado]. Ribeirão Preto (SP): Universidade de São Paulo; 2002.
30. Cummings SR, Newman TB, Hulley SB. Delineando um estudo observacional: estudos de coorte. In: Hulley SB, Cummings SR, Browner WS, Grady D; Hearst N, Newman T. B. Delineando a pesquisa clínica – uma abordagem epidemiológica. 2ª ed. Porto Alegre (RS): Artmed; 2003, p. 113-25.
31. Hulley SB, Cummings SR, Browner WS, Grady DG, Newman TB. Delineando a pesquisa clínica: uma abordagem epidemiológica. 3ª ed. Porto Alegre (RS): Artmed; 2008.
32. Chaves ECL. Revisão do diagnóstico de enfermagem Angústia espiritual [tese de doutorado]. Ribeirão Preto (SP): Universidade de São Paulo; 2008.
33. Galdeano LE, Rossi LA. Validação de conteúdo diagnóstico: critérios para seleção de expertos. Ciênc Cuid Saúde. 2006; 5:60-6.
34. Fehring RJ. The Fehring model. In: Carrol-Johnson RM, Paquette M, editors. Classification of nursing diagnoses: proceedings of the tenth conference. Philadelphia (USA): JB Lippincott; 1994. p. 55-62.
35. Oliveira CJ. Revisão do diagnóstico de enfermagem “Falta de Adesão” em pessoas com hipertensão arterial [tese de doutorado]. Fortaleza (CE): Universidade Federal do Ceará; 2011.
36. Santos FAAS. Construção e investigação da validade de definições conceituais e operacionais do resultado de enfermagem integridade tissular: um estudo com portadores de úlcera venosa [tese de doutorado]. Fortaleza (CE): Universidade Federal do Ceará; 2011.
37. Whitley GG. Process and methodologies for research validation of nursing diagnoses. Nurs Diagn. 1999; 10:5-14.
38. Carvalho EC, Bachion MM, Jesus CAC, Canini SRMS, Napoleão AA, Dalri M.C.B. Análise da produção da pós-graduação brasileira sobre validação de diagnóstico de enfermagem. In: Anais do 8º Simpósio Nacional de Diagnósticos de Enfermagem (SINADEn); 2006 maio 23-26; João Pessoa, Paraíba, Brasil. João Pessoa (PB): Ed UFPB; 2006. p. 1-5.
39. Silva VM. Padrão respiratório ineficaz em crianças portadoras de cardiopatias congênitas: validação de um instrumento de avaliação dos resultados de enfermagem [tese de doutorado]. Fortaleza (CE): Universidade Federal do Ceará; 2007.
40. Oliva APV. Diagnóstico de débito cardíaco diminuindo: validação clínica no pós-operatório de cirurgia cardíaca [dissertação de mestrado]. Ribeirão Preto (SP): Universidade de São Paulo; 2001.
41. Gordon M. Nursing diagnosis: process and application. 3ª ed. St. Louis (USA): Mosby; 1994.
Received: 21.03.2012
Approved: 18.01.2013