RESEARCH ARTICLES
Knowledge of the companions/caregivers of people victimized by cerebral vascular accident in the hospital context
Natália Pimentel Gomes SouzaI; Samia Jardelle Costa de Freitas ManivaII; Consuelo Helena Aires de FreitasIII
INurse. Student from the Academic Master Course in Clinical Care and Health Procedures at the State University of Ceará. Member of the Research Group Adult’s and Family’s Health. Fortaleza, Ceará, Brazil. E-mail: nataliapimentel88@yahoo.com.br
IINurse. Master in Clinical Care and Health Procedures at the State University of Ceará. Member of the Research Group Adult’s and Family’s Health. Fortaleza, Ceará, Brazil. E-mail: samia.jardelle@gmail.com
IIIPHD in Nursing. Professor from the Nursing Department at the State University of Ceará. Head of the Research Group Adult’s and Family’s Health. Fortaleza, Ceará, Brazil. E-mail: consueloaires@yahoo.com.br
ABSTRACT
This study aimed at seeking the knowledge about the care procedures of companions/caregivers of patients hospitalized for cerebral vascular accident. It is characterized as descriptive study, conducted with 14 patients and their respective caregivers in a public hospital at the municipality of Fortaleza. The data were collected between April and May 2011, through the techniques of semi-structured interview and simple observation, being that they were subjected to statistical and thematic analysis. The patients held a high degree of dependence and severe disabilities. The caregivers were women and their speeches have highlighted the founded difficulties for performing the care, among them, there is the lack of knowledge. We conclude that the caregivers are not prepared to assume their role in caring of such patients. Therefore, one should invest in preparing this clientele still within the hospital environment, thereby permeating other levels of health care.
Keywords: Cerebral vascular accident; caregivers; nursing care; nursing.
INTRODUCTION
Currently, cerebral vascular accident (CVA or stroke) is one of the main causes of death in the adult population1. Nevertheless, mortality is only one of the public health consequences arising from the stroke’s impact. Another equally important is the sequel and, consequently, unproductiveness, loss of quality of life and premature retirement of the individual2.
In cases of hospital discharge, many of the people victimized by CVA remain requiring special care due to the residual disabilities. Accordingly, in most cases, the family, as informal caregiver assumes the responsibility for conducting the homecare procedures. Nevertheless, to ensure the continuity of care, prevention of complications and reducing readmissions, it becomes essential having the preparation of family caregivers in the hospital scope, even in the face of monitoring implemented by the family health strategy (FHS) at home, with sights to assure the improvement in the quality of life of patients.
The study aimed at investigating the knowledge of companions/caregivers about the care for patients hospitalized because of stroke occurrence.
THEORETICAL BENCHMARK
In Brazil, the CVA is between the first and the third cause of mortality, depending on the year and State of the federation. According to estimates, approximately 85% of cases are sorted as of ischemic origin and 15% are hemorrhagic3.
The mortality rate of the disease in Ceará State was 44,8/100.000 inhabitants, in 2005; the diseases of the circulatory system accounted for 25,4% of all hospitalizations in the Brazilian Unified Health System (known as SUS) of individuals older than 65 years4.
As observed, the incidence of CVA has been growing due to the increase in life expectancy and changes in lifestyle. A study5 proves that the incidence of CVA is higher after the age of 65 years, given that there is an increased risk with the passing of time. This population aging, associated with risk factors for cerebrovascular diseases such as arterial hypertension, diabetes mellitus, smoking, alcohol consumption, obesity and dyslipidemia, explains, partly, the high incidence of CVA6.
Nonetheless, the mortality is not the only the public health consequences arising from the stroke’s impact. Another equally important is the sequel and, consequently, unproductiveness, loss of quality of life and premature retirement of the individual3.
Furthermore, the high number of hospitalizations for CVA generates a significant increase in hospitalization costs. In light of this, it becomes indispensable having the partnership of hospital institutions and of the patient's family for planning the hospital discharge as soon as possible, in order to reduce the hospital stay and increase the supply of hospital beds. In this context, the health status of the patient and the adequate preparation of the family are factors intervening in the deinstitutionalization process.
METHODOLOGY
This is a descriptive study, used by researchers when they seek further information from a known situation with sights to analyze the phenomenon by using variables and/or categories7.
The research was conducted in a tertiary hospital of the SUS network, located in the city of Fortaleza(capital of the Ceará State), possessor of 10 admission units destined for adult patients, totaling 300 hospital beds. The surveyed sectors were two wards, one neurological and other clinical, with capacities for 22 and 24 beds, respectively. The service has a multidisciplinary team comprised of physicians, nurses, nursing assistants and nursing technicians, physiotherapists, nutritionists, social workers, pharmacists and other health care professionals.
The study has included 14 patients with CVA and their respective caregivers, between April and May 2011, selected through the method of intended sampling. We have established the following criteria for inclusion in the sample: being patient hospitalized with a medical diagnosis of CVA and possessing a caregiver/companion during the hospitalization time. We have elected as an exclusion criterion: the caregiver demonstrate an impaired physical or mental status, in such a manner to prevent the interview conduction.
As to the data collection, we have performed it by using the technique of semi-structured interview, which was comprised of data related to the person victimized by CVA (sociodemographic variables, degree of disability and dependence in relation to activities of the daily life) and questions addressed to caregivers, which were regarding the care provided in the hospital environment towards the patient with CVA. We have measured the degree of dependence of the patient with CVA by means of the Barthel Index; and the degree of disability through the modified Rankin Scale. In a complementary manner to the semi-structured interview, we proceeded to the simple observation, being that the data were recorded in a field diary.
The information set related to patients was organized into a database in the Microsoft Office Excel®, 2010. Next, we proceeded to the statistical analysis, with absolute and percentage frequency, and presentation of data in tables and respective discussion with basis on the relevant literature to the issue at stake.
The collected material resulting from questions addressed to caregivers was organized and analyzed according to the technique of categorical thematic analysis8, in line with the following steps: we have performed the transcription of the interviews in full-text way, followed by the fluctuating reading, thus constituting the corpus of the work. After successive readings and material exploration, we proceeded to the cutout of the text in recording units, which enabled the formation of the following thematic categories: Sociodemographic characterization of patients hospitalized for CVA; The clinical status of people victimized by CVA in the hospital; The know-how of the caregiver in the hospital environment.
The study was derived from the research project of scientific initiation from the State University of Ceará, entitled “The health-disease process in the daily lives of people with arterial hypertension and diabetes mellitus in hospital and home contexts: meanings and beliefs”. The aforementioned project has been developed since August 2010. In line with the ethical and legal precepts related to researches involving human beings, the requirements of the Resolution nº 196/96 of the National Health Council were fulfilled, as well as we have obtained the signature of the Free and Informed Consent Form by the study participants. As required, the research project was approved by the Research Ethics Committee (REC) of the State University of Ceará (UECE), under the opinion nº 05050534-3, also having the obtaining approval in the surveyed institution under the registration number 140601/07.
RESULTS AND DISCUSSION
Sociodemographic characterization of patients hospitalized for CVA
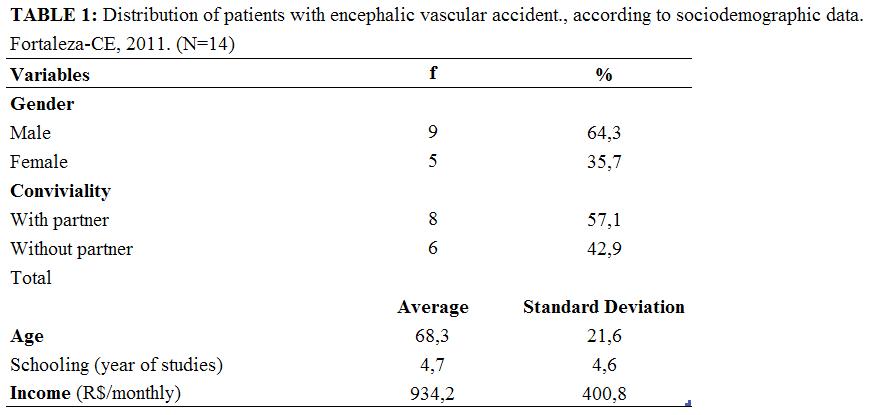
By analyzing the sociodemographic variables of the group of patients with CVA, we have discovered that they were predominantly male, 9 (64,3%) individuals; had coexistence with their partners, 8 (57,1%); average age of 62,3 years; average schooling of 4,7 years of studies; and average income of R$ 934,2/monthly. The variables of schooling and income showed higher concentration in low values, as shown in Table 1.
The low schooling level is indicated by the authors5,6,10 as a detrimental aspect to the understanding of the disease and of the care required in the home environment, thereby favoring the occurrence of new complications arising from the CVA occurrence.
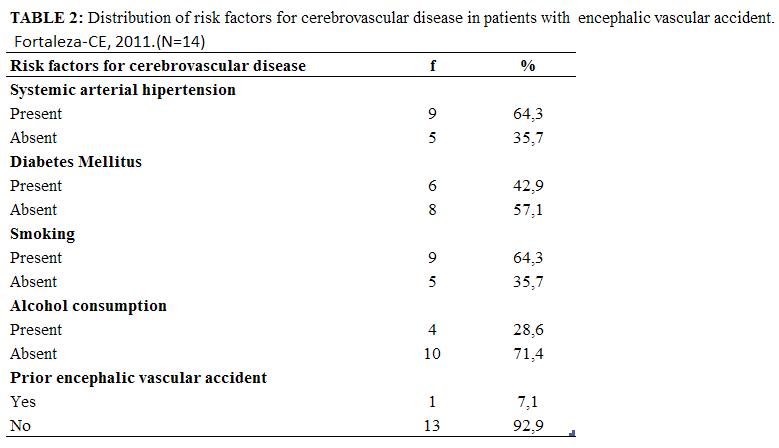
We have identified the occurrence of risk factors for cerebrovascular disease and comorbidity, whose data are shown in Table 2. Accordingly, of the 14 (100%) patients hospitalized with CVA, 9 (64,3%) were hypertensive, 6 (42,9%) diabetic, 9 (64,3%) smokers, 4 (28,6%) consumed alcoholic beverages and 1 (7,1%) showed previous CVA occurrence. According to the evidenced facts, the found risk factors differ from those listed in a particular study, in which the patients with CVA in the city of Fortaleza, Ceará State, have high frequency of arterial hypertension and lower frequency of smoking and alcohol consumption6. Regarding the practice of physical activities, only two patients performed it, in walking modality, prior to the episode of CVA. Depending on the data, the patients hospitalized held comorbidities associated with the CVA occurrence, therefore, need to receive specific guidelines to control risk factors and prevent the manifestation of clinical complications.
Among the patients, 8 (57,2%) lived with daughters and 6 (42,8%) with feminine spouse. As reported, these women would be the responsible for the care of the patient at home. The literature points to the increasingly common management of disabilities generated by CVA in the household context. Thus, the family, as a direct provider of homecare, needs to be prepared for this purpose11. Accordingly, the nursing professional should glimpse the family as a participant in the treatment. Therefore, it becomes necessary to provide support to this institution, not only to care for the patient, but, above all, to confront, understand and share the disease situation. One study has highlighted that the family caregivers, in most cases, are females, daughters or wives and, generally, had no experience in this activity12.
The clinical status of people victimized by CVA in the hospital
We have observed the health status of the patients in relation to the degree of dependency for activities of the daily life. For this purpose, we have used the Barthel Index. We proceeded to the review together with the patient and, when it did not present conditions to respond, the information was requested to the caregiver.
The Barthel Index is a widely used research tool to measure the person's ability to perform 10 activities of the daily life (feeding, bathing, personal hygiene, clothing, bowel control, bladder control, locomotion to the toilet, transferring from bed to chair, gait and stairs). It is a scale that helps to guide the actions of people assigned to follow-up the patient with regard to its progress in the functional capacity. It is also used to assess other neurological disorders. The standard score is 100 (maximum), with scores indicating the degree of dependence. So, the activities are assessed with different degrees, being that we might assign 0, 5, 10 or 15 points13. The initial score above 60 is related to shorter duration of hospital stay and greater likelihood to reintegrate the patient to community life after the hospital discharge14.
The patients of this study had a high degree of dependence, since 9 (64,3%) showed total dependence, with scores ranging from 10 to 20 points. They were patients restricted to the bed due to a relevant motor shortfall (hemiplegia/hemiparesis), fed by nasogastric probe and made use of permanent vesical catheter, as consequence of urinary incontinence. We have observed in 3 cases (28,5%), patients with severe dependence, by presenting scores equal to 40, 45 and 55; and 2 cases (14.3%) of patients with moderate dependence, scoring 65 and 80. Regarding the presence of pressure ulcers, 7 (50%) had an injury in at least one of the body regions: sacral, trochanteric and calcaneus (heels).
The degree of disability of the patients was assessed by the modified Rankin Scale. Of the surveyed subjects, 8 (57,2%) demonstrated severe disability, with score 5, i.e., they were restricted to the hospital bed, with urinary and/or fecal incontinence. Hence, they required care procedures and continuous nursing assistance. The Rankin Scale is mainly used for assessing the global disability, particularly in relation to the physical disability14.
It has proved to be relevant to make the characterization of patients with CVA for being a predictive factor of care to be implemented, both by the nursing staff of the hospital unit and by the caregivers. Thus, we could say that the greater the degree of disability and dependence to perform activities of the daily life, the greater the demand for care to be performed by the caregiver.
The know-how of the caregiver in the hospital environment
The knowledge of caregivers about the illness process was limited to the neurological sequels manifested by patients as a result of the CVA occurrence. It should be evidenced the superficial knowledge that was originated from empirical experiences in the daily management of these patients. None of the respondents showed knowledge about the etiological factors of CVA.
We have realized the association of CVA with arterial hypertension in two patients. In people affected by CVA, the blood pressure control is essential to prevent severe clinical complications, including recurrence of the cerebrovascular disease.
As reported, the caregivers did not receive guidance about the disease during the hospitalization time. The knowledge about the pathophysiology, risk factors, symptoms and behaviors of the general population is an important tool for reducing morbidity and mortality rates from CVA. In a study conducted in the Rio Grande do Sul State, it was found that, in a sample of 483 individuals, the knowledge of CVA was considered inadequate in 97,7% of individuals. As the main factor for the poor performance, the low schooling level was identified15.
Educational actions about CVA and its risk factors directed to family and caregivers should be prioritized by the health care staff, especially by nurses, because they will bring favorable results in the prevention and treatment of disease at stake. In a study of integrative review16 conducted with caregivers of elderly people, it was identified the exhaustion and the helplessness due to the fatigue in daily living activities associated with lack of information for holding the care. The patient care is complex and requires proper planning along with the family members. Thus, we highlight the role of the nursing professional in partnership with the caregiver to allow the homecare systematization, privileging those related to health promotion, prevention of disabilities and the maintenance of the functional capacity of the patient and of the caregiver itself.
As noted, the hospital care performed by the caregivers were inherent to the activities of the daily life; 92% corresponded to patient’s hygiene; 64,3% to nutritional care, including administration of diet by means of a nasogastric probe; 93% to position change (decubitus); 42,8% to the emptying of urine collectors; 42,8% to the administration of oral route medications and 57,2% to aid in relation to the prevention of falls.
It is a task of the caregiver to monitor and assist the person to take care in what he/she cannot do alone. In this context, we should remember: techniques and procedures identified with legally established professions, particularly in relation to the Nursing, are not part of the caregiver’s routine17.
Furthermore, the act of caring does not characterize the caregiver as a health care professional. Thus, the activities under the responsibility of the caregiver should be planned together with the nursing professional and the family itself. Therefore, one must clarify the caregiver about the procedures of its competency, as well as to recognize the danger signs18.
As can be seen, the situation verified in the study is worrisome, because, none of caregivers claimed to have received special training to perform such care, i.e., the care procedures were empirically performed. A similar situation was evidenced in the home environment in another study, also conducted in the city of Fortaleza, Ceará State, in which most caregivers reported implementing the care from knowledge of the daily practice and through the observation of the work of health care professionals during the hospitalization of their relatives. Authors highlight the benefits for the welfare and quality of life of patients with CVA when the caregiver is properly prepared19.
Accordingly, it is essential that the nursing professional seek strategies together with other health care professionals in the specific preparation of the caregiver by identifying the health needs according to each patient's clinical condition.
CONCLUSION
The study patients held a high degree of dependence to perform activities of the daily life and a high degree of disability arising from the CVA sequels. Therefore, they needed a caregiver.
In spite of the small sample size does not allow to generalize the findings, the characterization of patients was helpful and emphasized the urgent need to prepare the family and the caregiver in relation to CVA occurrences, its risk factors and general care procedures with the patient still in hospital environment.
The activities performed by the caregiver of such patients during the hospitalization time were related to activities of the daily life such as hygiene, feeding, position change (decubitus), administration of oral route medications and aid in relation to the prevention of falls. We have observed, in the hospital institution, that the caregivers have performed procedures related to the competency of the nursing staff. This is a situation worthy of attention for the nursing professional. We have investigated the knowledge of caregivers about the disease and it was proved as rudimentary, because of its limitation towards the sequels presented by the patients. As to the care procedures, we have identified the unpreparedness of caregivers, who conducted these shares in an empirical manner.
Given the aforementioned outcomes, we emphasize the importance of health education along with patients and family members/caregivers on the issues – the disease, recognition of signs and symptoms of AVC occurrences, control of risk factors and homecare actions after the hospital discharge. It is relevant to empower the family and the caregiver to the accomplishment of patient care, since it favors the continuity of care and prevents the occurrence of complications.
REFERENCES
1.Giles MF, Rothwell PM. Measuring the prevalence of stroke. Neuroepidemiolpgy. 2008; 30(4):205-6.
2.Araujo DV, Teich V, Passos RBF, Martins SCO. Análise de custo-efetividade da trombólise com alteplase no acidente vascular cerebral. Arq Bras Cardiol. 2010; 95: 12-20.
3.Sociedade Brasileira de Doenças Cerebrovasculares (Br). Primeiro consenso brasileiro para trombólise no acidente vascular cerebral isquêmico agudo. Arq Neuropsiquiatr. 2002; 60: 675-80.
4.Secretaria Estadual de Saúde (CE). Indicadores e dados básicos de saúde. Ceará (CE): SESA; 2007.
5.Fonseca NR, Penna AFG. Perfil do cuidador familiar do paciente com sequela de acidente vascular encefálico.Ciênc Saúde Coletiva. 2008; 13: 1175-80.
6.Cavalcante TF, Moreira RP, Araujo TL, Lopes MVO. Demographic factors and risk indicators of stroke: comparison between inhabitants of Fortaleza municipal district and the national profile. Rev Latino-Am Enfermagem. 2010; 18: 703-8.
7.Lobiondo-Wood G, Haber J. Pesquisa em enfermagem: métodos, avaliação crítica e utilização. Rio de Janeiro: Guanabara Koogan; 2001.
8. Bardin, L. Análise de conteúdo. 5ª ed. Lisboa (Por): Edições 70 Persona; 2010.
9.Ministério da Saúde (Br). Conselho Nacional de Saúde. Comitê Nacional de Ética em Pesquisa em Seres Humanos. Resolução nº 196: diretrizes e normas regulamentadoras de pesquisa envolvendo seres humanos. Brasília (DF): Editora MS; 2010.
10. Souza CB, Abreu RNDC, Brit EM, Moreira TMM, Silva LMS, Vasconcelos SMM. O cuidado domiciliar de idosos acometidos por acidente vascular cerebral: cuidadores familiares. Rev enferm UERJ. 2009;17: 41-5.
11.Machado ALG, Jorge MSB, Freitas CHA. A vivência do cuidador familiar de vítima de acidente vascular encefálico: uma abordagem interacionista. Rev Bras Enferm. 2009; 62: 246-51.
12.Andrade LM, Costa MFM, Caetano JA, Soares E, Beserra EP. A problemática do cuidador familiar do portador de acidente vascular cerebral. Rev esc enferm USP. 2009; 43: 37-43.
13.Moro CHC, Pontes Neto OM. Escalas de avaliação. In: Longo AL, Massaro AR, Moro CHC, Oliveira Filho J, Vedolin L, Friedrich MAG, et al. Programa de aperfeiçoamento continuado no tratamento do acidente vascular cerebral: PACTO AVC. 2009: p. 26-30.
14.Ruzafa JC, Moreno JD. Valoración de la discapacidad física: el Indice de Barthel. Rev Esp Salud Pública. 1997; 71: 127-37.
15.Costa F, Oliveira S, Magalhães P, Costa B, Papini R, Silveira M, et al. Nível de conhecimento da população adulta sobre acidente vascular cerebral (AVC) em Pelotas. J Bras Neurocir. 2008; 19: 31-7.
16.Aguiar ESS, Gomes IP, Fernandes MGM, Silva AO. Representações sociais do cuidar de idosos para cuidadores: revisão integrativa. Rev enferm UERJ. 2011; 19: 485-90.
17.Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Guia prático do cuidador. Brasília (DF): Editora MS; 2008.
18.Marin MJS, Angerami ELS. Caracterização de um grupo de idosas hospitalizadas e seus cuidadores visando o cuidado pós alta hospitalar. Rev esc enferm USP. 2002; 36: 33-41.
19.Machado ALG, Silva MJ, Freitas CHA. Assistência domiciliária em saúde: um olhar crítico sobre a produção científica de enfermagem. Rev Bras Enferm. 2011; 64: 365-9.
Received: 06.06.2012
Approved: 26.01.2013