RESEARCH ARTICLES
Systematization of nursing care: difficulties highlighted by the grounded theory
Ana Lúcia de MedeirosI, Sérgio Ribeiro dos SantosII, Rômulo Wanderley de Lima CabralIII
I Nurse Midwife. Master of Nursing, Professor of the Department of Women's Health Nursing, Faculty of Santa Emilia Rodat. João Pessoa, Paraíba, Brazil. E-mail: aninhapits@gmail.com
II Nurse. PhD in Sociology. Associate Professor, Department of Clinical Nursing and the Graduate Program in Nursing, Federal University of Paraíba. João Pessoa, Paraíba, Brazil. E-mail: srsantos207@gmail.com
III Nurses Midwife. Master in Public Health. Professor, Department of Nursing and Women's Health Program Graduate Obstetric Nursing College of Santa Emilia Rodat. João Pessoa, Paraíba, Brazil. E-mail: romulopits@gmail.com
ABSTRACT
Many problems are encountered in the implementation of the Systematization of Nursing (SAE), reflecting on the quality of care provided. The study aims to investigate the factors that hinder the operation of SAE in the obstetrics service. This is a qualitative study from the perspective of Grounded Theory, held in 2011, through open interviews with 13 nurses from a public hospital of the city of João Pessoa, Paraíba. Data analysis showed that factors hinder the operation of SAE and ways to better adherence and success through the application of the nursing process. Nurses expressed the knowledge dimension of SAE experienced in practice and their expectations of the socio-organizational context in which they exist. We conclude that the difficulties faced by nurses in the operation of SAE are diverse, highlighting: the small number of professionals, work overload and lack of operation of the process by the nurse.
Keywords: Nurse, nursing process; nursing care, working conditions.
INTRODUCTION
In the health scenario, the nurse practice is based nursing care supported on a theoretical and scientific sustained Care System in Nursing (ASN) and implemented through the nursing process. This is considered a method of decision making that promotes humane care, results oriented, encourages nurses to continually examine their actions, seeking to maximize service and minimize errors. It also helps to ensure that interventions are developed for the individual and not the disease1.
The application of SAE promotes improved quality of care, allowing the use of a scientific method that supports it. As part of customer service, directs and organizes the work, enables auditing, favors visibility and effective participation in professional care and in decision making, providing an individualized work on the needs of each client2.
However, since the beginning of its implementation in health services, some difficulties were noted. Among these are: those related to factors inherent in its structure, as its complexity and lack of uniformity in establishing each of its steps, related to the teaching-learning process, in that the undergraduate teaching and post-graduation courses has favored the acquisition of skills necessary for the development of this process, the difficulties within the healthcare practice, for example, the insecurity of professionals to carry out the activities inherent to the process and the number of nurses in most health services are inadequate for their proper development3.
Faced with these difficulties, many nurses have left to systematize their assistance and identify the nursing diagnoses. With that, they start to fragment care and customer problems, failing to see it as a whole and often, taking care that bear no relation to the problems encountered. Therefore, it is assumed that the non-application of the nursing process, an integral form, causes a nursing care inadequate, not individualized and not systematized customer.
In this context, the difficulties in operationalizing the SAE are described by nursing students, nurses and teachers in several researches, hence the relevance of this study so that we can think of overcoming them in everyday practice of nursing care.
Beginning with this issue, the following question arose: what factors hinder the implementation of the NCS by nurses in the obstetrics service? Therefore, this study aimed to investigate the factors that hinder the operation of SAE at obstetrical service of a public hospital.
THEORETICAL-METHODOLOGICAL REFERENCES
Nursing as a discipline, focuses on the science and art of caring human being. In recent years it has progressively consolidated its known and do care to humans as an integral being, seeking to give meaning to their existence. In this context, means that care is essential in different situations of human life, be it in health promotion, disease prevention, in the course of diseases and their complications, disabilities or in the process of dying.
Considering this scenario, the SAE is an essential tool in planning and executing such care, with a method used by nurses to collect data, plan, implement and evaluate care, ie, identifies the situations of health and illness and care needs nursing and subsidizes the promotion interventions, prevention, recovery and rehabilitation of the individual, family and community5. Soon, reveals the importance of this methodology in the care of humans, where there is a meeting of real health problems be careful intervention caregiver, requiring judgment, skill and expertise in decision making of nurses, ensuring that way, the quality and safety of care provided.
Its implementation as a process of practical work appropriate to community needs and how to care model to be applied in all areas of health care by nurses is effectively improves the quality of nursing care. Thus, the Federal Board of Nursing established the Resolution No 272/026,, repealed by Resolution No 358/097, which provides for the systematization of nursing care in health institutions in Brazil.
Therefore, the SAE is a form of work organization that aims, through its structuring, ensuring the best quality of care to the client and ensure that nursing interventions are developed for each client. Looking emphasize the individual's assessment focused not only on the disease, providing agility in finding the diagnosis or treatment of health problems and real potential8.
This is a descriptive study with a qualitative approach in the perspective of Grounded Theory. The survey was conducted from January to April 2011 at a public hospital in the city of João Pessoa, Paraíba, Brazil. The subjects of the research collaborators were thirteen nurses who work at the site where the research was conducted.
Before starting the process of data collection, the research project was submitted to the Ethics Committee in Research of the Lauro Wanderley University Hospital of the Federal University of Paraíba (UFPB), which approved the opinion of the rapporteur and the Certificate issued in 083 / 2010, authorizing the search. As for the ethical position, norteamo us by the criteria established in the Guidelines and Standards of Research Involving Human Subjects9.
Collection and processing of data
For data collection techniques were used participant observation and semi-structured interview, with guiding questions inherent in the proposed objective research. The subject of this quantitative benchmark was determined by theoretical saturation. Thus, not restricted the number of participants, so that this number was set according to the content and consistency of data from the depositions. Thus, as these data were being collected, were analyzed concurrently aiming at theoretical saturation, enabling the emergence of possible sample groups.
In this theoretical and methodological framework, to verify the data saturation, ie when no other information adds or modifies existing ones, begins the systematic and deeper analysis of all data from different samples. Therefore, the saturation of the sample was achieved after completion of the 13th interview.
So that one could understand the meaning of the data obtained through interviews and observations, we proceeded to his analysis, coding them, categorizing them and identifying the phenomenon. Data analysis was done in three steps interdependent, namely: open coding, axial, and selective coding.
The open coding was done manually by reading the interviews. For each fragment of the interview were assigned words or expressions, forming the preliminary code. In the next phase, set itself a conceptual or abstract name for each grouping of data, code by code, which had some resemblance to each other or even distinct characteristics.
Continuing with the analysis of the data passed to the stage of axial coding, in which the data were grouped into new forms, establishing connections between categories, seeking to expand and densify the emerging phenomenon.
Continuing the analytical process, it moved to the stage of selective coding where categories were worked in depth and density consistency. This refinement is a process of integration between the categories and subcategories defined, unveiling the results of the studied phenomenon. When this stage of the work has been achieved, we sought to inter-relate the representative categories to translate concretely the theoretical sensitivity to understand the meaning of the experience of nurses as a whole. From there, we tried to develop a theoretical model of this experience.
The phenomenon was examined in the light of the paradigm of analysis of Strauss and Corbin, as a way of grouping the categories and facilitate data analysis. Therefore, we tried to understand what were the causal conditions that developed in the phenomenon, the context and the strategies that were being conducted. It also sought to identify the consequences that determine the occurrence.
RESULTS AND DISCUSSION
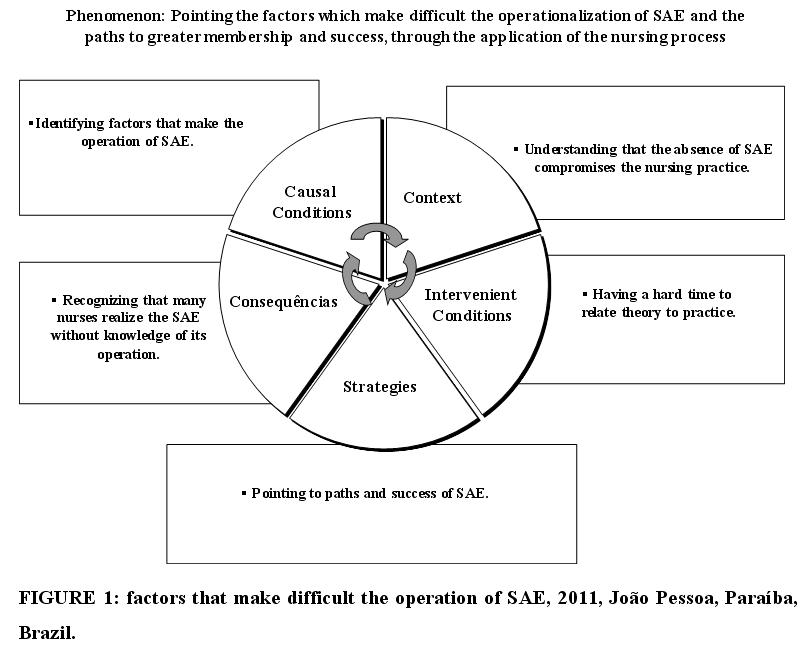
Data analysis of the phenomenon resulted in the factors that hinder the operation of SAE and the paths to greater compliance and success through the application of the nursing process.
This phenomenon provides an understanding of the transformation of tacit knowledge into explicit knowledge of the practice of everyday work experienced by nurses, within a context that has its peculiarities. Therefore, the presentation of results in this study was to enable an understanding of the experiences of these professionals, from the identification of the phenomenon analyzed using the standard paradigm of Strauss and Corbin, as shown in Figure 1, which plots the phenomenon analyzed .
Highlighting the causal conditions
Category: Identifying factors that hinder the operation of SAE
In this category the nurses pointed out the main factors that affect the operation of SAE, impairing its performance. And so, expect to arise proposed solutions that contribute to their development in order to improve the methodology of nursing work.
The difficulties faced by nurses for deployment of SAE are diverse, according pointed this category, highlighting the following: the small number of nurses, lack of credibility of the nursing technicians and front of the SAE workload of nurses as express the statements:
[...] First the insufficient number of nurses [...] is another thing that hinders the workload of nurses, because often we have to deploy to meet our responsibilities and respond by all in the industry. (Alfazema)
[...] Another factor is the lack of credibility of the nursing staff, since most do not believe in SAE or view the nursing prescription as something important to the customer. (Azaléa)
The workload of nurses, coupled with the reduced number of nursing professionals in health institutions, has interfered directly in the application of the nursing process. These professionals perform many tasks not always linked to their professional area, away from the fact that assistance, leading to excessive workload. Consequently, the execution of the nursing process is no longer priority.
Regarding the credibility of SAE, one realizes the devaluation of the practice by some nurses, specifically by some technicians. These, in most cases, perform the care of mechanically, limiting its assistance to a routine procedure, failing to observe what was prescribed by the nurse, giving priority to medical prescription. Thus, the devaluation of nursing prescription undermines the credibility of the practice of integrative action as SAE care.
These difficulties are similar to those found in some research on the subject, where the overhead of nurses related to bureaucratic activities has hindered their professional as well as the disbelief and rejection of the nursing technicians front of SAE12,13.
Emphasizing the context
Category: Understanding that the absence of SAE undertakes nursing practice
Failure to use the SAE can bring many consequences. The main problem is compromising the quality of care provided, reflecting the lack of customer needs. According demonstrates that category, nurses understand that the absence of SAE compromises assistance both in the obstetrics service as in other workplaces, as stated in his speech:
[...] Without performing the nursing process, we have difficulties, we do not know the direction to follow. [...] Not all hospitals have implemented the SAE. This adversely affects the quality of care provided. (Violeta)
The consequences of not using the SAE are: disorganization of the service generated by different forms of professional conduct in care; experienced the conflict between the desire to provide a direct client care and administrative activities; devaluation of nurses in a hospital setting; wear human resources evidenced by the lack of planning, resulting in decreased productivity and quality of care, the loss of time caused by the lack of planning and priority setting.14.
Although SAE is not implemented in many health services in Brazil is operationalized or partially, nurses recognize their importance and the need to structure the services for their proper functioning. In this context, the deployment of SAE, care shall be executed individually and needs of each client are met in the best way possible, contributing to its recovery and continuity of care.
Thus, by putting into practice the models of the nursing process, nurses promote skilled care to patients in a minimum time and maximum efficiency15.
Highlighting intervening conditions
Category: Having difficulty to relate theory to practice
A discourse analysis of nurses provides insight into how they see the relationship between theory and practice. In the perception of some nurses, it is difficult to relate theory to practice, when it comes to SAE. Many of them have difficulty to operationalize it by considering theoretical activity, which is just on paper, far from reality. In this respect, the nurses show that there is a weakness in the way of implementation of the NAS, due to the emergence of many problems. These difficulties need to be understood in order to create strategies that can help in overcoming it, so that nurses are able to develop a planned and organized assistance. The reports express that situation well:
[...] Cannot make this relationship between theory and practice, find it all very theoretical.
[...] Only studied the SAE at the University. When we got to the service, not put into practice because in many services, there is no SAE. (Orquídea)
The lack of relationship between theory and practice in nursing exists as a result of the formation process of these professionals is usually done within a theoretical framework poorly suited for nursing practice. Consequently, the academic model that prevails in the preparation of nurses is still the technical-rational that describes a scientific perspective of nursing as a hierarchical knowledge, theoretical and academic status16.
Therefore, teachers must commit to promote situations that create a meaningful learning that stimulates critical thinking and reflective of the students, making them understand that they are active subjects in the process of teaching and learning.
Developing strategies for action
The vision of nurses to their lived experience in practice is focused on the SAE as a way to build an integrated knowledge (explicit or tacit). Facing the possibility of improving the operation of SAE, the study presents the following category that represents the action strategies used by nurses:
Category: Pointing paths to greater compliance and success of SAE
To achieve effective implementation of SAE or to overcome difficulties, some studies indicate paths that possibly will lead to success. Therefore, for the success of SAE, there must be a partnership with continuing education in order to overcome the difficulties of real professionals.
The maternity nurses studied showed some ways that facilitate the effectiveness of SAE, ensuring adherence and success in nursing practice, among them are: in-service training for nursing staff, political administrators of services, use of instruments that address the phases of the nursing process and wider dissemination of SAE to improve the credibility and value of nursing prescriptions. This proposal can be seen in the following statements:
[...] For better adhesion of SAE at obstetrical service, we need direction and coordination of nursing skills and make training for nurses and nursing technicians. [...] We need forms that include patient history, physical examination, nursing diagnoses and nursing prescriptions in the medical record. (Íris)
[...] When we apply the nursing process in the day-to-day, we are showing its importance. But it must appear to most SAE events in nursing and are stimulated research on this topic. (Tulipa)
For an effective implementation of the NCS, there must be a commitment of the nursing leadership with the proposal. He shall hold meetings and prepare an action plan, including staff awareness of the importance of this methodology. It should also promote further research on the topic with the involvement of the whole team, and collectively build the means to enable the execution of the process.
The lack of tools that can facilitate the registration process by nurses has been identified as a factor that hinders the deployment of SAE. Features that favor the record and organize the data, such as computer technology or the development of specific instruments for data collection, can bring advantages such as standardization of information, agility in decision making, improving care, increasing productivity and professional satisfaction, possibility of better production from adequate documentation for lawful purposes and research17.
The SAE must be recognized by all professional nursing as a working methodology that aims to promote a systematic customer care. Therefore, it is of fundamental importance to the collective construction of this process. Thus, to understand its importance and the full realization of its stages, it is necessary that all nursing staff involved in the work process.
The recognition of SAE on the part of other health professionals will only be possible through the dissemination of benefits arising from their use, both for the nurse and for the customers and also to the health institution. Its use is considered important because it systematizes nursing actions, is essential to have a good tour. Also, it provides recognition of the profession, prompting the nurse to occupy its space within the healthcare team.
Thus, it is concluded that the SAE promotes individualized assistance, visibility and autonomy for nurses, as well as provides subsidies for the development of technical and scientific knowledge, which characterizes nursing as a discipline and science, whose own specific knowledge5.
Identifying the consequences of the phenomenon
Category: Recognizing that many nurses perform SAE without knowledge of its functioning
While SAE has been implemented in Brazil since the 1970s, only received legal support from the Federal Board of Nursing in 2002, through Resolution No 2726, then, by Resolution No. 3587. However, many studies show that these resolutions were not sufficient to guide its implementation, since many difficulties are still encountered in the realization of this methodology care.
The nurses in the obstetrics service recognize that many nurses perform the requirements of SAE only by COREN and the institution where they work, not recognizing the benefits it can bring to the customer, for the institution and especially for nursing. This fact is evidenced in the following report:
[...] Even though the SAE deployed in the service, I observe that many nurses are performing just because the demand is COFEN or the institution, without giving the real importance it requires. (Hortência)
In the current context, the implementation of the NCS becomes a necessity, as it can provide definition, differentiation and enhancement of the profession and nursing professionals. Moreover, it is a resource that provides nurses to apply and demonstrate their scientific, technical and human resources in the care of cliente18. But only after the requirement COFEN, it was established that the SAE should be applied to all health services.
Due to the requirement of regulatory agencies and nursing administrators of health institutions, many nurses realize the SAE in everyday practice, even without commitment to this methodology. In this direction, the disengagement can be related to lack of theoretical knowledge that subsidizes the nursing process or the operation of the process itself, with all its component phases.
It should be remembered that the SAE is for nursing professionals, institution customers and an important technical and scientific instrument capable of ensuring the quality and continuity of nursing care and cost containment, and a guarantee for legal purposes. Therefore, drawn by nurses, allows the full humanized care, appreciation of the nurse and his entire team3.
CONCLUSION
The study showed that among the many factors that have hindered the operation of SAE in obstetrics clinic, appointed by nurses, deserves the lack of credibility of the nursing technicians front of the SAE, the workload of nurses, the unwillingness of managers deploy the SAE and the ignorance of the functioning of the process by nursing professionals.
The integration of the categories emerged from the study showed that nurses expressed interest in seeking alternatives to address the difficulties, tracing their paths to greater compliance in order to implement it in all phases of the nursing process to the needs of customers were met.
Although we have sought all rigors in analysis and procedures used in this study, it is important that highlighted some aspects concerning its limitations. Firstly, the method used in this research - Grounded Theory - despite allowing a full check of the identified categories and deep, characterized by being limited to the situation studied in the service, not allowing the full generalization of their results and conclusions for other services. And secondly, that although the categories surveyed are significant according to the theoretical framework presented, does not exhaust the possibilities of the subject under study. Thus, some could also be worked in order to verify the difficulties to operationalize the point SAE and strategic changes in the service.
REFERENCES
1. Barreto M, Petra S. The process of introduction and implementation of the systematization of the nursing assistance at a hospitalization unit belonging to a private institution: a case study. Online braz j nurs [online]. 2007 [Access 2010 Dec 10]. 6(3) Available:
http://www.objnursing.uff.br/index.php/nursing/article/view/j.1676-4285.2007.1050/244.
2. Costa NB, Kitchenman SRS, Nunes AS, Santiago MMA. Sistematização da assistência de enfermagem: vantagens, dificuldades e características das publicações. In: Anais do 61º Congresso Brasileiro de Enfermagem; 2009 dez 7-10; Fortaleza, Brasil. Fortaleza (CE): Associação Brasileira de Enfermagem; 2009.
3. Carvalho EC, Bachion MM, Dalri MCB, Jesus CAC. Obstacles for the implantation of the nursing process in Brazil. Rev enferm UFPE on line [online]. 2007 [Access2010 Aug 15]; 1:95-9. Available:
http://www.ufpe.br/revistaenfermagem/index.php/revista/article/view/17-8781-1-/pdf_172
4. Guedes HM, Nunes DP, Nakatani AYK, Bachion MM. Identificação de diagnósticos de enfermagem do domínio atividade/repouso em idosos admitidos em hospital. Rev enferm UERJ. 2010; 18:513-18.
5. Truppel TC, Meier MJ, Calixto RC, Peruzzo SA, Crozeta K. Sistematização da assistência de enfermagem em unidade de terapia intensiva. Rev Bras Enferm. 2009; 62:221-7.
6. Conselho Federal de Enfermagem (COFEN). Resolução nº 272, de 27 de agosto de 2002. Dispõe sobre a sistematização da assistência de enfermagem nas instituições de saúde. Rio de Janeiro: COFEN; 2002.
7. Conselho Federal de Enfermagem (COFEN). Resolução nº 358, de 15 de outubro de 2009. Dispõe sobre sistematização da assistência de enfermagem e a implementação do processo de enfermagem em ambientes, públicos ou privados, em que ocorre o cuidado profissional de enfermagem. Rio de Janeiro: COFEN; 2009.
8. Silva DCN, Ribeiro AA, Fabrício SCC. Produção do conhecimento sobre sistematização da assistência de enfermagem a idosos. Rev enferm UERJ. 2007; 15:406-0.
9. Ministério da Saúde (Br). Conselho Nacional de Saúde. Resolução 196, de 10 de outubro de 1996: diretrizes e normas regulamentadoras de pesquisa envolvendo seres humanos. Brasília (DF); 1996.
10. Dantas CC. Teoria fundamentada nos dados - aspectos conceituais e operacionais: metodologia possível de ser aplicada na pesquisa em enfermagem. Rev Latino-Am Enfermagem. 2009; 17:573-9.
11. Strauss A, Corbin J. Pesquisa qualitativa: técnica e procedimentos para o desenvolvimento da teoria fundamentada. 2ª ed. Porto Alegre: Artmed; 2008.
12. França FVC, Kawaguchi IAL, Silva EP, Abrão GA, Uemura H, Alfonso LM, et al. Implementação do diagnóstico de enfermagem na Unidade de Terapia Intensiva e os dificultadores para enfermagem: relato de experiência. Rev Eletr Enferm [online]. 2007 [Access 2011 Aug 12]; 9(2):537-46. Available: http://www.fen.ufg.br/revista/v9/n2/v9n2a20.htm
13. Uchôa MG, Lemes MMDD. A visão dos enfermeiros que trabalham em unidade hospitalar pública sobre a Sistematização da Assistência de Enfermagem [online]. Goiânia: Núcleo de Estudos e Pesquisas em Saúde e Sociedade (NEPSS); 2008 [Access 2011 Apr 14]. Available:
http://www.ucg.br/ucg/insti tutos/nepss/monografi a/monografi a_01.pdf
14. Andrade JS, Vieira MJ. Prática assistencial de enfermagem: problemas, perspectivas e necessidade de sistematização. Rev Bras Enferm. 2005; 58:261-5.
15. Amante LN, Rossetto AP, Schneider DG. Sistematização da Assistência de Enfermagem em Unidade de Terapia Intensiva sustentada pela Teoria de Wanda Horta. Rev Esc Enferm USP [online]. 2009 [Access 2011 Dec 18]; 43(1):54-64. Available: <http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0080-62342009000100007&lng=en&nrm=iso>.
16. Santos SR, Nóbrega MML. A busca da interação teoria e prática no sistema de informação em enfermagem: enfoque na teoria fundamentada nos dados. Rev Latino-Am Enfermagem. 2004; 12:460-8.
17. Évora YDM, Dalri MCB. O uso do computador como ferramenta para a implantação do processo de enfermagem. Rev Bras Enferm. 2005; 55:709-13.
18. Pivotto F, Lunardi Filho WD, Lunardi VL. Prescrição de enfermagem: dos motivos da não realização às possíveis estratégias de implementação. Cogitare enferm. 2004; 9:60-70.
Received: 24.07.2012
Approved: 26.01.2013