
RESEARCH ARTICLES
School, emotional and behavioral performance of children infected by HIV: preliminary study
Ana Cristina Magazoni BraghetoI; Ana Maria Pimenta CarvalhoII
IPsychology. Doctorate in Science Degree from the University of São Paulo. Ribeirão Preto Nursing College. Department of Psychiatric Nursing. Ribeirão Preto, São Paulo, Brazil.E-mail: crisbragheto@yahoo.com.br
IIPsychology. Post-doctorate in Centre of Addiction and Mental Health. Doctorate in PsychologySchool and Human Development from the University of São Paulo. Professor Lecturer of the University of São Paulo. Ribeirão PretoNursingCollege. Professor of the Department of Psychiatric Nursing. Ribeirão Preto, São Paulo, Brazil. E-mail: anacar@eerp.usp.br
ABSTRACT
The study aimed to evaluate the school performance and the cognitive and emotional development of children with HIV and non-infected children. Participants were children and adolescents between 7 and 12 years old. where 15 children were infected with HIV/AIDS and 15 children without chronic diseases and their respective caregivers answered to the instruments School Performance Test (SPT), Children’s Strengths and Difficulties Questionnaire (SDQ) and Human Figure Drawing Test (HFDT). Results showed that there are differences regarding the cognitive development. Those with HIV/AIDS were more compromised.In the behavioral assessment, the two groups differed only in the domain relationship with colleagues. Regarding the school performance, results were lower than expected for both groups. The findings suggest the development of care strategies for HIV children, over all, highlight aspects to be investigated in other studies.
Keywords: HIV; children; child development; psychology.
INTRODUCTION
There were about 370.000 children infected with HIV (Human Immunodeficiency Virus), especially in underdeveloped countries, such as Africa, until 2009. Under the global plan, the goal would be to work to reduce that number to 90% by the end of 20151.declined in the past two yearsThese children, in particular, face common problems, aim by the literature of the area: they live with an infection that still has no cure; are exposed to prejudice and discrimination; hospitalized in moments of complications (which increase with advanced stages of the disease or in those cases without satisfactory engagement); are required to take at least twice a day medicines of unpleasant taste, which cannot be delayed or not taken and even feel the side effects, often without the clear understanding of the need, since in most cases, the diagnosis is not revealed2.
This set of conditions is presented as an obstacle to the goal development of the child threatening, in particular, their mental health.
This work aims to evaluate though children, parents and caregivers of HIV infected children, which are the social skills, school performance and cognitive and emotional development.
THEORETICAL REFERENTIAL
HIV infection is a chronic condition with repercussions on the physical and psychological development of children and adolescents with HIV, especially those infected by mother-to-child transmission. With the advent of ant-retroviral therapy and access to treatment, studies have shown improvements in the quality of life of HIV positive children so that psychosocial needs have new meaning and relevance3, 4.
Before the advent of the combined anti-retroviral therapy, the mortality rate in children with HIV was high, in addition to the frequent occurrence of psychomotor development and neurocognitive deficits due to the action of HIV on the central nervous system5. In addition, a study of Brazilian children showed that neurological déficits were associated with other symptoms: headaches, learning difficulties, paresthesia and dysphagia6.
Studies conducted in developed countries indicate that HIV positive children have a higher risk of having psychological adjustment problems depending on the variety of stressors, such as: maintaining the secret of diagnosis, routine changes and presence of multigenerational losses. Difficulties in dealing with the daily need to take medicines, feelings of anger, frustration, loneliness and low self-esteem were also identified in some studies7.
The socioeconomic factors that permeate the conditions, under which children with HIV live, are in precarious situations for the development, such as: financial difficulties, lack of education, lack of environmental stimulus and parental cares. The co-occurrence of risks increases the likelihood of the child to development problems8.
These factors may influence the treatment adherence, use of treatment services, in family relationships and revelation of the disease. Also they can influence the development of the child with regard to emotional aspects.
Considering the importance of this condition for development, being physical, cognitive, social, economic, emotional and/or liked to interpersonal relationship and the relative absence of studies in the country on this subject, the hypothesis is that HIV infected children have lower results in evaluations concerning their mental health.
In children, mental health indices are inferred from the assessment of school performance, behavior displayed in relations with other people from their surrounding and cognitive and emotional development9. The knowledge about the cognitive and emotional development of children infected with HIV can assist health professionals involved in this population assistance.
METHODOLOGY
This is a cross-sectional, quantitative study, conducted in the special unit of infectious diseases therapy of a teaching hospital of São Paulo and in an institution that serves children from 0 to 12 years old in the same location. Convenience sample was used and under the conditions laid down by the researcher10.
The number if subjects was set on the basis of studies that use the comparison group strategy, considering also the difficulties in approaching them within a given time limit, the number of children available at the time of data collection where the research was conducted and the possibility of statistical treatment of data, through non-parametric techniques.
15 children were selected and their caregivers and/or parents, HIV infected and 15 children and their caregivers and/or parents, without chronic disease for the control group. The children ages ranged from 7 to 12 years old, six boys and nine girls infected by HIV, students from the first to sixth grade of elementary school. The control group was treated in gender, age, social class and grades with the group of children with HIV.
In both groups, the distribution of participants in the social classes was: eight in class C, six in the class D and one in class B2.
Among caregivers who participated in this research, was chosen the person who lives with the child and provided care every day. In the group of children with HIV, were interviewed three aunts, seven grandmothers and five mothers. The age ranged from 32 to 58 years old.
As for education, eight were illiterate, four had elementary school incomplete and three of them have high school incomplete. The group of children without chronic diseases, 13 mothers and two grandmothers were interviewed. The age range was 25 to 47 years old. As for education, 11 had elementary school incomplete, three of them high school incomplete and one with a degree level.
In the group of children with HIV, the inclusion criteria to participate in the research were children aged 7 to 12 years old, without distinction of sex, who have been infected by HIV through mother-to-child transmission, with a follow-up in the unit and with use of anti-retroviral therapy.
Exclusion criteria to participate in the group of HIV infected children were: children who were not in school that would prevent the assessment; home shelter children, for which there is not a responsible caregiver that could participate in the research; children residing outside the region of Riberão Preto and children with disabilities, such as cerebral paralysis.
In the group of children without chronic disease were excluded those who have any other chronic disease. Family and caregivers, as well as nursing assistant of the institution were interviewed to obtain information about the child, to exclude any kind of chronic illness (asthma, diabetes, cancer, among others), because this group would only be children without this type of illness.
For the data collection, the following instruments were used: - Children’s Strengths and Difficulties Questionnaire (SDQ)11, 12: brief instrument, used for tracking of mental health problems in children and young people from 4 to 16 years old. It is consisted of 25 items (subdivided in attention deficit/hyperactivity, anxiety or depression, behave problems, relationship problems with colleagues and pro-social behavior) to be answered by parents and/or caregivers, focusing on the child´s behavior, their emotions and relationships with other people.
School Performance Test (SPT)13: provides standards for classification of the child´s performance on tasks of reading, writing and arithmetic. The performance of the child is classified into three levels: lower, middle and upper in the three subtests and in the total classification of the test according the norm of the grades.
- Human Figure Drawing Test (HFDT)14: evaluates the cognitive and emotional development of the child. It is asked the child to draw a person, and then another person of the opposite sex. The assessment is based on the characteristics of the drawing (e.g. if it has head, eyes, pupils, ears, etc.) proposed by Koppitz in the 60, which are assigned 0 to 1 points to items proposed.
- Brazil criterion: it does the socioeconomic characterization of the families in which children live. It was applied to parents and caregivers of the child15.
Children with HIV and their responsible were addressed during the outpatient consultations, and on this occasion we present the research proposal and we invite them to participate. After acceptance, we arranged a day and place for the interview and the assessments, searching for places where they could feel comfortable to discuss the study, without interruptions. The average time of application of instruments in children was 100 minutes and 60 minutes for caregivers. The children without chronic disease were addressed in the institution itself, as well as their responsible.
A análise dos dados foi feita mediante o cômputo dos escores de cada criança nos domínios avaliados e segundo as instruções de uso de cada instrumento.
The scores of the two groups – research group (children with HIV) and control group (children without chronic disease) were compared using non-parametric tests, Mann-Whitney U Test and Fisher Exact Test16, with alpha equal to 0,05. For the assessment on HFDT, it was checked by naive evaluators about the child being affected with HIV or not.
In compliance with the laws governing research on human beings17, the Project was submitted to the Research Ethics Committee of the Hospital where the collection of data would be held, having been approved in accordance with the process of the Clinic Hospital of Ribeirão Preto (HCRP) no 12745/2006.
RESULTS AND DISCUSION
The detailed results of each domain show the non-differentiation between the two groups, with the exception of the domain problems with colleagues, as shown in Table 1.
TABELA 1: SDQ Domains- Children’s Strengths and Difficulties Questionnaire. Scores of children according to the scales evaluated by the instrument – emotional Symptoms, behavioral problems, problem with colleagues and hyperactivity. Ribeirão Preto, São Paulo, 2007
(*) Mann-Whitney U Test
Here are the results for the evaluation of school performance.
The distribution of children in different levels of performance was similar. The comparison of the distribution of the two groups, through Fisher Exact Test – p = 0,2885 shows that there is no statistically differences between them.
The assessment through the Human Figure Drawing Test, initially proceeded to the examination of the evaluators´ agreement and there were the following results: 92% among the judges, to the evolutionary indicators and 89% for the emotional indicators. The results of the two groups in the assessment of evolutionary and emotional indices through the Human Figure Drawing Test (HFDT), are shown in table 2.
TABELA 2: Medium, minimum and maximum values and p values concerning to the scores obtained by the children of the two groups in the Human Figure Drawing Test. Ribeirão Preto, São Paulo, 2007.
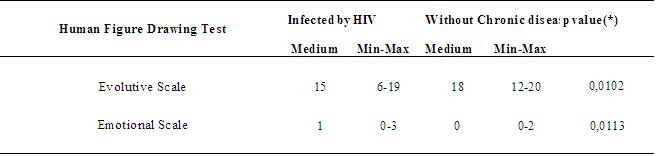
(*) Mann-Whitney U Test.
It was found that the differences between the two groups reached statistical significance. It was used the Mann-Whitney U Test for comparison of the two groups as to the raw scores obtained in the test, according to the table 2.
Problems with colleagues were the only category of differentiation between the groups in the evaluation through the SDQ.
As regards with social skills, caregivers of children with HIV say they participate in activities in groups, having the opportunity to enjoy socializing experiences with family and peers. However, some of them show their concerns relating to the restriction of activities that could facilitate the acquisition of opportunities infections or result in physical damage to the child.5. It is noticed in these behaviors, excessive care and protection in the child, reducing opportunities for relationship leading children, under this condition, to have in the perception of their caregivers, fewer problems. In addition, one might think that their routines, which include out-patient consultations, school absences and hospitalizations, making more difficult the creation of b links with colleagues, avoiding the emergence of problems in this relationship. There is also the issue of closing to new relations and exchange of experiences that child with HIV face, due to the stigma brought by them and their caregivers. The study reports that a substantial portion (40-50%) of the American population still believed that could be contaminated with HIV, kissing someone with the virus, as well as most of the interviewed believe that drinking water in the same glass and using public restrooms can also be forms of contagion. These conceptions seem to join the closing of those infected by HIV for relationships18, 19.
In the hyperactivity, emotional symptoms and behavior problems, the results of this study show the difficulties of the two groups, both of children with HIV, such as children without chronic disease. A possible explanatory hypothesis for these findings is that the children of both groups come from lower socioeconomic class, have fewer resources, which may leave their caregivers under stressful condition in relation to concerns about the maintenance of the house and children setting them to a more negative perception of them.
Children´s mental disorders such as: hyperactivity, emotional symptoms and behavior problems are the most common and are important because result in suffering to young people, children and those with whom they live, because they interfere in psychosocial and educational development, and can generate problems and interpersonal relationships in adult life20.
As for the pro-social behavior, also no differences were found between the two groups. This suggests the presence of resources that promote the social development of children.
On school performance, there was no difference between the groups evaluated, and in both, most of the children performed less than expected. However, another part of the group showed lower performance. This refers to the conditions of public schools. Evaluations conducted by the Evaluation System of Academic Achievement in the State of São Paulo (Saresp) show that the state elementary schools in the city of Ribeirão Preto, had below national average, schools in which children participated in this research, both infected with HIV as those without chronic diseases are inserted21.
In cognitive plan, however, is not the same, corroborating the findings of literature suggesting that deficits for children with HIV22.
In the emotional development of children, it was found that the group with HIV showed more prejudiced. It is necessary to point out that the differences are caused by four children who exhibited lower results in this evaluation. Most of them (n= 11 - 73,3%), showed good result from the emotional point of view. The two groups generally exhibited good result on this point, which differed from the evaluation of their caregivers. This suggests emotional potential preserved, constituting personal protection factor to development. However, we must consider that the instruments used are different and the data the generate come from different sources – children and caregivers.
CONCLUSION
In spite of the limitation of the study, use of self-report instruments, small sample size and selection for convenience, it was found some indicatives of the need for attention to children with HIV who, in this study, showed lower performance in cognitive and emotional maturity.
The findings of this research provide subsidies on the development and care of children infected by HIV, psychosocial aspects, which is still little in national literature and open issues for future studies. It also brings specific information about the cognitive and emotional development of these children to health care professionals.
REFERENCES
1.UNAIDS. AIDS epidemic update: fevereiro 2012 [Internet]. 2012 [cited 2012 fev 27]. Available from: http://www.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2011/20110609_JC2137_Global-Plan-Elimination-HIV-Children_en.pdf~
2.Moreira MCN, Cunha CC. Repensando as práticas e dilemas no cotidiano de atenção à saúde de crianças e jovens vivendo com HIV/AIDS. Divulg Saúde Debate. 2003;(29):73-92.
3.Ledlie SW. The psychosocial issues of children with perinatally acquired HIV disease becoming adolescents: a growing challenge for providers. AIDS Patient Care STDs. 2001;15:231-6.
4.Mialky E, Vagnoni J, Rutstein R. School-age children with perinatally acquired HIV infection: medical and psychosocial issues in a Philadelphia cohort. AIDS Patient Care STDs. 2001;15:575-9.
5.Seidl EMF, Rossi WS, Viana KF, Meneses AKF, Meirelles E. Crianças e adolescentes vivendo com HIV/ AIDS e suas famílias: aspectos psicossociais e enfrentamento. Psicol Teor Pesqui. 2005;21:279-88.
6.Araújo APQC. Neurologic findings in Brazilian children with human immunodeficiency virus infection. Pediatr AIDS HIV Infect. 1994;5:33-4.
7.Khoury M, Kovacs A. Pediatric HIV infection. Clin Obstet Gynecol. 2001;44:243-75.
8.Pedromônico MRM. Instrumentos de triagem e vigilância do desenvolvimento da criança de 0 a 6 anos. In: Mendes EG, Almeida MA. Temas em educação especial. São Carlos: Editora UFSCar; 2004. p. 325-30.
9.Masten AS, Coatsworth JD. The development of compentece in favorable naunfavorabel environments: lessons from research on successful children. American Psychologist. 1998; 53: 205-20.
10.Cozby PC. Métodos de pesquisa em ciência do comportamento. São Paulo: Atlas; 2003.
11.Cury CR, Golfeto JH.Strengths and difficulties questionnaire (SDQ): a study ofschool children in Ribeirão Preto. Rev Bras Psiquiatr. 2003;25:139-45.
12.Goodman, R. The extended version of the strengths and difficulties questionnaire as a guide to child psychiatric caseness and consequent burden. J Child Psychol Psychiatr Allied Discipl. 1999;40:791-9.
13.Stein LM. Teste de desempenho escolar-TDE. São Paulo: Casa do Psicólogo; 1994.
14.Hutz CS, Antoniazzi AS. O desenvolvimento do desenho da figura humana em crianças de 5 a 15 anos de idade: normal para avaliação. Psicol Reflex Crít. 1995;8:3-18.
15.Associação Brasileira de Empresas de Pesquisa. Critério de classificação econômica Brasil [Internet]. 2003 [citado em15 maio 2008]. Disponível em: http://www.abep.org/codigosguias/ABEP_CCEB_2003.pdf
16.Siegel S. Estatística não paramétrica. São Paulo: McGraw-Hill do Brasil; 1975.
17.Ministério da Saúde (Br). Diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Brasília (DF): Ministério da Saúde; 2002.
18.Pedromônico MRM, Venske S, Duarte CS, Succi RM. Problemas de comportamento em filhos de mães portadoras de HIV. Folha Méd. 2000; 119 (2): 29-35.
19.Siegel K, Lekas HM. AIDS as a chronic illness: psychosocial implications. AIDS. 2002;16:69-76.
20.Fleitlich BW, Goodman R. Implantação e implementação de serviços de saúde mental comunitários para crianças e adolescentes. Rev Bras Psiquiatr. 2002;24:2.
21.Sistema de Avaliação de Rendimento Escolar do Estado de São Paulo (Saresp) [Internet]. 2009 [citado 2010 set 20]. Disponível em: http://saresp.fde.sp.gov.br/2009/
22.Steele RG, Nelson TD, Cole BP. Psychosocial functioning of children with AIDS and HIV infection: review of the literature from a socioecological framework. J Dev Behav Pediatr. 2007;28:58-69.
Received: 15.05.2012
Approved: 15.01.2013