ORIGINAL RESEARCH
Quality of nursing care: patient environment in a medium-complexity public hospital
Fabiane Gorni BorsatoI; Marli Terezinha de Oliveira VannuchiII; Maria do Carmo Fernandez Lourenço HaddadIII
INurse. Master in Nursing. Responsible for the Nursing Quality Control
Service at the Hospital Dr. Anísio Figueiredo. Londrina, Paraná, Brazil.
E-mail: fgborsato@gmail.com
IINurse. PhD in Public Health. Pofessor of the Master in Nursing at the
State University of Londrina. Parana Brazil. E-mail: vannuchi@sercomtel.com.br
III
Nurse. PhD in Fundamental Nursing. Professor of the Master in Nursing at
the State University of Londrina. Parana Brazil. E-mail: haddad@sercomtel.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2016.6222
ABSTRACT
Objective: to compare the findings of two earlier assessments of nursing care quality conducted by patient environment observation at a medium-complexity public hospital in north Paraná. Method: from June to December, 2011, this retrospective, quantitative study collected secondary data from two reports provided by the Office of Nursing Quality Control at an adult inpatient unit. Results: hygiene and comfort, physical safety and use of equipment were observed to improve, while compliance with device identification routines and pressure ulcer prevention deteriorated. It was possible to analyze the process and the structure involved in care and the associated risk factors. Conclusion: despite the positive results, there is clearly still a need to implement educational strategies to continue to improve nursing care processes.
Keywords: Quality control; nursing assessment; patient safety; health care quality assurance.
INTRODUCTION
In face with the changes that have occurred with globalization and technological development, the health area has suffered great impact and has realized the need to redesign its work processes to ensure the effectiveness of its services1. Quality assurance has become a key requirement for economic survival in response to increased consumer demand and also ethical and legal demands and as customers' social right2.
These changes in the modern world have brought the beneficial combination of processes, technologies and human relationships, from the therapeutic point of view. On the other hand, it started to be required from the manager an efficient plan of action for the management of this new and complex system, to maintain the quality combined with the minimization of risks to the customer3. From there, the focus of analysis has influenced an organizational culture based on changes of attitudes and behaviors2.
For nursing, the management of quality of care has always been a focus of concern, determined historically, dating from the time of Florence Nightingale. Currently, with the incorporation of advances in this category and its development as a profession, nursing has even more turned its gaze to guarantee the quality of care as a customer right2. In this context, it started to introduce in its management processes, assessment methodologies of structural components, processes and results, making it possible to gather information about the quality of care, compare them to previously established standards and use them as basis for the implementation of continuous improvement measures2,4,5.
It must also be taken into account that the management of quality in health goes beyond the pursuit of excellence of services and customer satisfaction, reaching the possibility of identifying potential risk factors to the customer, amenable to treatment, allowing the incorporation of the culture of patient safety in the care management process2,6.
Whereas much of the nursing care activities take place on site, with the client, without interruption, knowledge about the service quality conditions can be obtained by analyzing the care setting, from the observation of the patient and their environment7. With this methodology, the aspects related to the structure of the place where care is performed and care conditions to the patient in face of the hospital environment can be easily observed, as well as some aspects related to the development of care and its outcomes.
There are few studies that present results of quality programs related to infrastructure and qualification of professionals8. Guided by this, this study aimed to compare the results of the first two evaluations of nursing care quality carried out by observing the patient environment in a medium complexity public hospital.
LITERATURE REVIEW
Quality management began in the industrial context and had, in that means, the proposal of various concepts, methods and techniques to achieve and maintain quality by several scholars. In health area the physician Avedis Donabedian was the most prominent scholar2. This scholar has proposed several theories, and initially presented quality determined by three interdependent aspects, namely scientific knowledge, interpersonal relations and environmental factors. Later, he developed the seven pillars of quality that comprises efficacy, effectiveness, efficiency, optimization, acceptability, legitimacy, equity9.
Donabedian developed his proposal of quality evaluative model guided on the triad structure, processes and results10:
Nursing professionals are an important part of the staff that work in health services and are also engaged in the quality movement, making use of healthcare strategies used and bringing from the academic training the ideals of quality guided in continuous training and satisfaction of users' needs11. Despite this apparent adherence, there is still need for presenting reports on quality management models and their results in nursing services, for better dissemination of proposals and achievement of credibility8.
Considering the model proposed by Donabedian, his transposition to implementation in nursing should be applied through the analysis of the care setting, which enables data collection from the observation of the patient and their environment6. This methodology will identify determinants of quality care related to structure, process of care and outcomes of care provided, culminating in the proposal driven by Avedis Donabedian.
METHODOLOGY
This is a retrospective and quantitative study on the quality of nursing care, verified by analysis of the patient's environment in an adult inpatient unit of a medium complexity public hospital in the north of Parana, with collection of secondary data provided by the Nursing Quality Control in Service (SCQE in Portuguese) of the institution.
The SCQE performs the evaluation of nursing care quality with the use of three instruments adapted from Haddad, one of them called environmental observation script, which allows checking aspects related to physical environment and the patient's condition as regards hygiene and comfort, physical activity, physical safety, nutrition and hydration, oxygenation and ventilation, disposal and use of equipment. Each item belonging to the observation script has guiding sub-items in the evaluation process, for which it is assigned yes, no or not applicable, according to what is observed by the evaluator. Evaluations are carried out every 3 months, in 20% of hospitalized patients, and at the end of a month management reports are issued, composed of simple percentages compounds on the quality of care4.
In this research, secondary data were collected from the management reports of two evaluations conducted by SCQE in an adult inpatient unit of the institution under study, from June to December 2011, which were, evaluation 1 and evaluation 2, occurred with an interval 3 months between them.
Data were tabulated in specific worksheet in Microsoft Excel 2007, by adding the values of the two evaluations in order to compare the data.
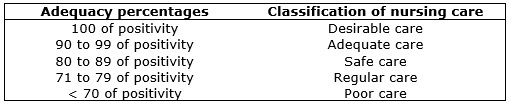
For data analysis, authors a methodology adopted by Haddad (2011) 4, which is the same used by SCQE, composed of the classification indices suggested by Carter apud Saupe, Horr 12. See Figure 1.
FIGURE
1
:
Carter's classification indices according to Sauipe, Horr12,
used in assessing the quality of nursing care of the studied institution.
Londrina-PR, 2011.
The study was approved by the Ethics Research Committee on Human Beings of the State University of Londrina, under the opinion number 238/2011 and CAAE 0220.0.268.000-11.
RESULTS AND DISCUSSION
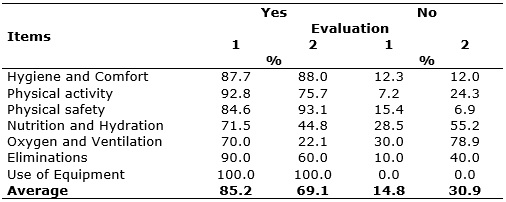
The results showed decline in nursing care quality between the two evaluations performed during the study period in the study unit, through the observation of the patient and their hospital environment. There was a fall of the general rate of positivity from 85.2% to 69.1%, changing from a safe care to a poor one, according to reference standards used in this study, as presented in Table 1.
TABLE 1:
Percentages of two reports provided by the nursing quality control service
of a medium complexity public hospital, concerning the observation of the
hospitalized patient's environment. Paraná, from July to December 2011.
Source: Evaluation reports of nursing care quality provided by the SCQE of
a medium complexity public hospital of in the north, Parana, 2011
Evaluation of hygiene and comfort
The results for hygiene and comfort remained within the safe care range, as shown in Table 1. This means improvements in the implementation of this care by the category that considers it essential to promote physical and mental well-being and consequently, health recovery13. This result was influenced by the change in the profile of patients in the second evaluation, who presented low dependence, i.e., ability to self-care 14. Also, this positive result was determined by advances in primary care identified in this study, such as oral, hair, limbs and bed hygiene, in addition to the correct alignment of bedridden patients.
Body hygiene consists of a set of body care (considered in this research as hair, body, hands and feet hygiene), which is highlighted in discussions on health promotion 15. It pervades the physical well-being, as the effective oral hygiene, with a positive impact on the control of infection, as it allows the reduction of the microbial load of the oral cavity, and hence the reduction in the potential risk for respiratory tract infections. Unfortunately, the oral care is little disseminated in hospitals and needs viable ways to attract the attention of professionals to this hygiene, as the customer does pays attention to this care because of their health conditions 16,17. Another study conducted in a public general hospital in Bahia identified that the institution did not offer this care to bedridden and dependent patients 18.
Evaluation of activity and physical safety
By analyzing the aspects related to the physical activity of hospitalized patient under observation, it was possible to identify a decline from appropriate care to regular care, determined by the decrease in positive percentage, as shown in Table 1. It is noteworthy that decubitus change is an important nursing intervention for pressure ulcer (PU) prevention and that should happens periodically to avoid skin lesions by pressure 18.
Concomitant to the mentioned result, there was the increase in cases of PU. The institution and the national quality management standards consider the incidence indicator of PU as determinant in the analysis of the care process5, and this analysis point is one of the most important in this study.
As for the patient's physical safety, as can be seen in Table 1, there was a transition from safe care to adequate care, with positive index rising from 84.6% to 93.1%, from the first to the second assessment, showing improvements in measures to mitigate and / or eliminate risks to the client during their stay.
In this context, the structural and procedural aspects related to environmental hygiene, which increased from 84.6% to 100% of positivity, were analyzed, showing improvement in the ambience and host; the identification of the bed remained adequate, reflecting the guarantee of safety of the hospitalized patient through an effective communication and information tool of their data, which agrees with research conducted at a university hospital in the north of Parana state in 2008, which showed the reach of 100 % of identified beds in an adult inpatient unit7.
Still, as another factor of customer safety analysis, information on the fall prevention were established by proper maintenance of patient positioning in armchair, showing appropriate care and the increase in the rate of patients who were in beds with high side rails (from regular to adequate). This reflected adjustments in preventing falls, which consists of potentially determinant of worsening of health condition of the patient or, even, of causing other morbidity conditions19.
The causes of falls are multifactorial and may be intrinsic, related to physiological processes of the patient, and extrinsic, when they are linked to structural and context aspects. It is necessary that nursing professionals know the risk factors and adopt preventive measures 20.
As for the structural aspects involved in the analysis of physical safety, there was an increase in the values related to the presence of ring available to the patient, which allows greater agility when calling the nursing staff, and appropriate furniture and equipment in good working conditions, which provide greater adaptation of the environment, free of risks.
This study presented positive results with regard to some aspects of patient safety, however, given the complexity that permeates health care, the potential for adverse events that corresponds to any injury caused to the patient in the period in which they receive health care is increasing, and these can cause temporary or permanent damage21.
Nursing, as ubiquitous professional category, has great responsibility in defining strategies aimed at recovery of the patient's health and, therefore, it is faced with the close relationship between nursing care and the prevention of other diseases, in particular adverse events16 .
The Regional Nursing Council of São Paulo State created in 2010, a booklet titled The 10 steps to patient safety, which establishes, among the measures of nursing care to prevent welfare risks, the prevention of pressure ulcers, the correct and complete identification of the patient and the prevention of falls, all covered in this research22.
Other aspects of the evaluation
This study also showed other results related to various aspects of observation of patients and their hospital environment. There was a considerable decrease in the quality of care from the first to the second evaluation performed during the study period in the items related to nutrition and hydration (71.5% to 44.8%) and eliminations (90.0% to 60.0%) , changing from a regular profile to poor one. This result was impacted by the lack of identification of devices such as venous access, serum catheters, nasogastric and vesical tubes, contrasting the positive results for this aspect of evaluation, obtained in a survey conducted in adult inpatient unit of a university hospital, in 20087. These findings highlight the need for adequacy to the institution's Hospital Infection Control Service recommendations, which requires some types of care, such as the identification of such devices, paying attention to the installation date on the patient in order to ensure the exchange before expiration.
Even with the low quality of identification of venous access and equipment, there was maintenance of the rate related to the absence of post-infiltrative lesions within the safe care range (80 to 89%). These results differ from those presented in research conducted in a university hospital in Porto Alegre, where the occurrence of post-infiltrative lesions reached 24.7% and whose author did not correlate its incidence with the installation time of the venous catheter. However, the incidence of this type of injury, in addition to being caused by some medications, type and location of the catheter, is strongly related to time of stay inside the client, requiring that health professionals adopt measures to improve the care with this device23.
When analyzing the oxygenation and ventilation, there was decrease of the percentage from 70.0% to 22.1% between the evaluations carried out during the study period, and this result is determined by inadequacies in the provision of inhalers in the environment after use and in the time of stay of nebulizers and inhalers in use. It should be emphasized that in 100.0% of cases such devices were expired in both assessments.
Still, in this research, there was a decrease from 90.0% to 60.0% between assessments in the quality of care aimed at eliminations, moving from an adequate care to poor care. This was due to the decrease in percentage on the existence of identification of vesical probes and inadequacies in relation to the filling of the collection bag for beyong two thirds of its capacity.
CONCLUSION
This research enabled analyzing the nursing care performed in the institution under study, based on assessment of the patient's condition and the hospital environment and on everyday aspects of nursing care that are only subject to analysis through the applied methodology.
Even with the positive results presented, it was possible to identify decrease in rates related to compliance with established routines and for the prevention of pressure ulcers, highlighting the need to implement educational strategies with nursing professionals relating to the incorporation of quality care culture associated with patient safety ideals, as well as with regard to adherence to the practice of care with excellence.
It is worth noting that the reports reflect values obtained from data collected once a day, which indicates the possible occurrence of quality changes in the course of the shift and depending on the nursing staff, which is considered a limiting point for the study. However, the research helps to know the care situation as regards observable aspects in the work of the teams, giving credibility and enhancement of results, which are management tool for nursing administration in the search for strategies to improve their services.
REFERENCES
1.Vituri DW, Matsuda LM. Validation of content of quality indicators for evaluation of nursing care. Rev esc enferm USP. 2009; 43: 429-37.
2.Vituri DW, Évora YDM. M. Total Quality Management and hospital nursing: an integrative literature review. Rev Bras enferm. 2015; 68:945-52.
3.Gimenes FRE. The safety of patients in drug administration in an intensive care unit of a general hospital in the countryside of Sao Paulo state: the restorative health approach [PhD thesis]. Ribeirão Preto: University of São Paulo. Ribeirão Preto College of Nursing; 2011.
4.Haddad MCFL, Évora YDM. Implementation of quality program in a public university hospital. Cienc cuid saude. 2012; 11: 78-86.
5.Caldana G, Gabriel CS, Bernardes A, Évora YDM. Performance indicators in hospital nursing service: integrative review. Rev RENE. 2011; 12: 189-97.
6.Gomes AQF. Initiatives for patient safety spread over the Internet by international organizations: an exploratory study [dissertation]. Rio de Janeiro: Oswaldo Cruz Foundation; 2008.
7.Vituri DW, Cacciari P, Gvodz R, Kuwabara CCT, Cardoso MGP. Quality indicators as a strategy to improve quality care in a university hospital. Cienc cuid saude. 2010; 9: 782-90.
8.Rocha ESB, Trevizan MA, Rocha K, Catelhano-Souza M. Quality management in Brazilian nursing: literature review. Rev enferm UERJ. 2013; 21: 812-7
9.Donabedian A. The seven pillars of quality. Archuves of Pathology & Laboratory Medicine. Northefield. 1990; 121: 1743-48.
10.Donabedian A. The quality care. How can it be assessed? JAMA. 1988; 12-260.
11. Pires AS, Souza NVDO, Penna LHG, Tavares KFA, D'oliveira CAFB; Almeida CM. Nursing training: an integrative review. Rev enferm UERJ. 2014: 22:705-11.
12.Saupe R, Horr L. Nursing audit. Rev cien saúde. 1982; 1: 23.
13. Ministry of Health (Br). Constitution of the World Health Organization. Geneva: World Health Organization; 1946.
14.Oliveira DLLC. Nursing and its bets in self-care: emancipatory investments or subjection practices? Rev bras enferm. 2011; 64: 185-88.
15.Bigas M, Guimarães F. Comparative study on the approach of body hygiene in Portugal (2009/10 - 2010/11): a first analysis of textbooks to study the environment. Repositor UM [online]. 2011. Available in: http://hdl.handle.net/1822/17137
16.Benedet AS, Brasil N. The systematization of nursing care and the care needs of hospitalized patients in intensive care unit. Rev eletr gestão & saúde. 2012; 03: 800-15.
17.Lima DC, Saliba NA, Garbin AJI, Fernandes LA, Garbin CAS. The importance of oral health in the perspective of hospitalized patients. Ciênc saúde coletiva. 2011; 16: 1173-80.
18.Passos SSS, Sadigusky D. Nursing care for the dependent hospitalized patient. Rev enferm UERJ; 2011. 19: 598-603.
19.Vitor AF, Araújo TL. Settings for the nursing result of prevention of falls: an integrative review. Rev. eletr. enf. [on-line]. 2011; 13: 313-22. Available in: http://www.fen.ufg.br/revista/v13/n2/v13n2a18.htm
20.Ramos CV, Santos SSC, Barlem ELD, Pelzer MT. Falls in the elderly of two emergency care units of Rio Grande do Sul. Rev. eletr. enf. [on-line]. 2011; 13: 703-13. Available in: http://www.fen.ufg.br/revista/v13/n4/v13n4a15.htm
21.Bezerra ALQ, Queiroz ES, Weber J, Paranaguá TB. Adverse events: performance indicators according to the perception of nurses in a sentinel hospital. Enferm glob. 2012; 27: 198-209.
22. São Paulo Regional Nursing Council. 10 steps to patient safety. Sao Paulo: Regional Nursing Council of São Paulo; 2010.
23.Urbanetto, JS. Prevalence of phebitis in adult patients with peripheral venous catheter. Rev enferm UFSM. 2011; 1: 440-8.