RESEARCH ARTICLES
Acute coronary syndrome: risk in youth
Leticia Pereira de SouzaI; Renata RigonII; Maria Antonieta MoraesIII; Silvia GoldmeierIV; Lúcia PellandaV
I
Specialist in Cardiology. Multidisciplinary Integrated Residence in Health: Cardiology, Institute of Cardiology, Cardiology University Foundation. Porto
Alegre, Rio Grande do Sul, Brazil. E-mail: leticiapds@yahoo.com.br
II
Specialist in Cardiology. Lato-Sensu Graduate Program: Nursing in Cardiology, Institute of Cardiology, Cardiology University Foundation. Porto Alegre, Rio
Grande do Sul, Brazil. E-mail: re_rigon@yahoo.com.br
III
PhD in Health Sciences: Cardiology. Professor of Lato Sensu Graduation: Nursing in Cardiology, Institute of Cardiology, Cardiology University Foundation.
Porto Alegre, Rio Grande do Sul, Brazil. E-mail: antonieta_moraes@uol.com.br
IV
PhD in Health Sciences: Cardiology. Professor of Lato Sensu Graduation: Nursing in Cardiology, Institute of Cardiology, Cardiology University Foundation.
Porto Alegre, Rio Grande do Sul, Brazil. E-mail: pesquisa.sgold@gmail.com
V
Cardiologist. PhD in Health Sciences: Cardiology. Coordinator of Graduate Program in Health Sciences: Cardiology, Cardiology University Foundation. Porto
Alegre, Rio Grande do Sul, Brazil. E-mail: lupellanda@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2015.5934
ABSTRACT
This cross-sectional study to determine risk for acute coronary syndrome in young adults examined patients of both sexes aged 20-50 years admitted to a cardiology hospital in Rio Grande do Sul State between September 2010 and June 2012 with diagnoses of acute coronary syndrome. The cardiovascular risk factors analyzed were: age, family history, smoking, body mass index, physical activity, blood pressure, glucose, triglycerides, total cholesterol and high density lipoproteins. The results comprised 96 patients, mean age 43±7.4 years, 52(54.2%) of them male, and 57(59.4%) with acute myocardial infarction with ST-segment elevation. The most prevalent risk factors were positive family history 53(55.2%) and smoking 49(51%). A multidisciplinary approach should be introduced to modify lifestyle and prevent new events.
Keywords: Acute coronary syndrome; risk factors; young adults; primary prevention.
INTRODUCTION
In recent years, cardiovascular diseases (CVD) have occurred, prematurely, in adults less than 45 years-old1. The concern in the medical, social, psychological, and economic area has been linked to the prevalence of current society diseases boosted by unhealthy lifestyle. The diagnosis among young individuals is not as well characterized as in older subjects2. The committed vessels are often only what can be related to genetic and family history aspects of the disease3.
About 5% to 10% of acute myocardial infarctions occur in adulthood-young age4-6, comprised between 20 and 40 years, but with better prognostics 5,6. Setting this risk profile, we may invest in primary prevention, reducing rehabilitation expenditures. Therefore, the aim of this study was to determine the risks in young-adult patients with early acute coronary syndrome, who are hospitalized in a cardiology-reference, in the State of Rio Grande do Sul (RS).
THEORETICAL REFERENTIAL
The risk factors (RF) that have been singled out as responsible for the higher prevalence of CVD in this population are: tobaccoism, hypercholesterolemia (modifiable) and positive family history (not modifiable)5-8.
Exposure to RF typically begins in childhood and is then consolidated in youth9-11. Cholesterol deposition in coronary arteries since childhood, this provides for an increase in the extent of injuries in more advanced ages12 and it is through food culture started in childhood that we may decrease the advance in the progression of lesions.
Studies report that individuals, who consume greater amounts of foods containing saturated fats, have a higher incidence of coronary atherosclerosis than those who do not consume. In the long run the saturated fats raise cholesterol levels and cause damage to the coronary arteries13,14.
Another aspect of great importance refers to the prevalence of obesity in our culture. Two factors, such as the high consumption of processed foods and insufficient practice of physical activity leverage the emergency of CVD in the future. It is recommended to carry out at least 30 minutes a day of mild or moderate intensity activity on five or more days of the week, or the practice of at least, 20 minutes a day of vigorous intensity physical activity three or more days of the week. Reversing lifestyles, considered detrimental to quality of life, becomes a must for public policies and health practices whose orientation is focused on prevention15,16.
The prevalence of dyslipidemias in children and adolescents has been growing over the last years proven by the elevation in plasma levels of low-density lipoprotein (LDL), a decisive factor in developing atherosclerosis17.
Data obtained in RS, in 2008, showed 3228 deaths by circulatory system diseases. Of these, six deaths were 20 to 29 year-old; 31 between 30 to 39 years and 150 between 10 to 49 years18.
Studies in several countries have shown concern with adults who suffer an early ischemic event19-21.
In order to enable planning with preventive and effective actions, it is necessary to know the particularities of the RF related to CVD in the target population.
METHODOLOGY
Cross-sectional study, developed from September 2010 to June 2012, which included young-adult patients with diagnosis of acute coronary syndrome (ACS), hospitalized in a cardiology reference institution of Rio Grande do Sul,
Patients of both genders, aged between 20 and 50 years, diagnosed with ACS of whatever origin were included in the study. The exclusion criteria were patients who have communication barriers and neurological degenerative diseases, clinical instability or did not accept to participate in the study.
A questionnaire with the variables: gender, age, positive family history (FH+), systemic arterial hypertension (SAH), hypercholesterolemia, hypertriglyceridemia, High Density Lipoproteins (HDL), tobaccoism, sedentarism, overweight/obesity and diabetes mellitus (DM) were used in our study.
ACS was considered through the medical diagnosis of unstable angina (IA), acute myocardial infarction (AMI) with ST-segment elevation (W/STSE), AMI with no STSE, through electrocardiogram (ECG) and by the result of altered cardiac enzymes (CK total for women > 81 U/L, and for men > 129 U/L; CK MB> 10 U/L; Troponin T > 100 pg/ml)22. FH+ was considered when first-grade close relatives (father, mother, or brother) had developed some early coronary disease23. Hypertension was considered when blood pressure value reached ≥ 140/90 mmHg24. Diabetes Mellitus was characterized with a previous medical diagnosis, or when the patient stated use of oral hypoglycemic agents and/or insulin, or still, when two consecutive fasting blood glucose tests ≥ 126 mg/dl occur, or one ≥ 200 mg/dl24. Total cholesterol was considered when plasma values reached ≥ 240 mg/dl, altered HDL with values ≤ 35 mg/dl25 and high triglycerides ≥ 150 mg/dl25.
Tobaccoism referred to patients who smoked any quantity of cigarettes a day24. Overweight meant a body mass index (BMI) ≥ 25 Kg/m²; and obesity BMI ≥ 26 29.9 Kg/m². Sedentarism has been evaluated by the international physical activity questionnaire (IPAQ-8) - short version, validated in Brazil, and proposed by the World Health Organization (WHO). It contains questions on intensity and duration of physical activity during a normal week, both in occupational activities as well as in locomotion, leisure and sports, classifying patients in: very active, active, irregularly active or sedentary 27.
To calculate the sample, a 50% prevalence of disease was set in patients with acute coronary syndrome, with 5% error margin and 90% confidence interval, resulting in an estimation of 96 patients.
The analyses were conducted using the Statistical Package for Social Sciences (SPSS) 19.0. Categorical variables were described in absolute and relative frequencies (%). Continuous variables were expressed as mean values and standard deviation or median and 25% and 75% percentiles, as followed or non-normal distribution.
We used the Chi-square test in order to assess association between gender and qualitative variables and for quantitative variables; the comparison among genders was done through T-test or Mann-Whitney nonparametric test. P < 0.05 values were accepted as significant.
The project was approved by the Committee of Ethics in Research of the Cardiology Institute/ Cardiology University Foundation, under No. 4516/10. The subjects who have agreed to participate in the study signed a Free and Clarified Consent Form (FCCF).
RESULTS AND DISCUSSION
The predominant gender was male - 52 (54.2%), with a mean age of 43 ± 7.4 years. The more prevalent RF were family history (+) 53 (55.2%), tobaccoism - 49 (51%), overweight/obesity - 70 (71.8%). In relation to biochemical tests, 17 (17.7%) were hypercholesterolemic, 44 (45.8%), with HDL ≤ 35 mg/dl and 41 (42.7%) were with triglycerides (TG) ≥ 150 mg/dl. Increased blood glucose was found in 35 (36.5%) subjects of the sample and hypertension in 24 (25%).
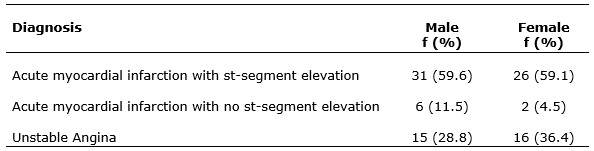
The prevalence of AMI W/STSE was 57 (59.4%), 31 (32.3%) showed unstable angina and 8 (8.3%) AMI with no/STSE. AMI W/STSE was found in 57 (59.6%) of male and 57 (59.1%) of female as recorded in Table 1.
TABLE 1: Prevalence of Acute Coronary Syndrome according to gender of patients. Porto Alegre – RS, 2012. (N=96)
International physical activity questionnaire (IPAQ) level is ranked as very active with 14 (14.6%), active with 35 (35.4%), irregularly active with 35 (36.5%) and sedentary representing 13.5%. These data are shown in Figure 1.
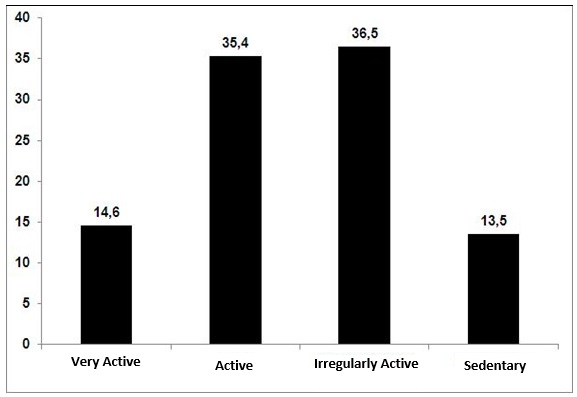
FIGURE 1: Percentage distribution of physical activity classified according to IPAQ. Porto Alegre – RS, 2012. (N=96)
DISCUSSION
This study was developed to identify risk profile in patients with early ACS, who are hospitalized a reference cardiology university hospital in RS, in order to demonstrate that cardiovascular risk factors and CVD are found not just in the more advanced life phase,.
The demographic characteristics of the patients with ACS in our study demonstrated a predominance of males with a mean age of 43 years. These findings corroborate the records described in the literature whose prevalence of CHD (Coronary Heart Disease) occurs most often in young males becoming similar among genders around 80 years28.
The risk factors found in our sample with ACS showed the presence of positive family CHD history, followed by tobaccoism and overweight. In an Italian study conducted with people of the same age group, the findings identified that the majority of individuals had a positive family history and tobaccoism 29.
World Health Organization has been warning that even though tobaccoism has decreased in developed countries it is on the rise of about 3% per year in developing countries. In research conducted by the Risk Factor Monitoring System in Brazil showed that Porto Alegre (RS) and Rio Branco (Acre) are the Brazilian capitals with the highest percentage of smokers: 21.2% of total population30.
The results of this study showed high proportion of patients with overweight and obesity. Similar data have been recorded in different national and international scenarios26. The consensus of secondary prevention for CHD of the American Heart Association and American College Cardiology consider obesity as a major risk factor for cardiovascular disease33. Studies refer to a higher recurrence of heart attack and death among individuals with high body mass index34,35 and that hypertension is cited as being one of the main risk factors for ACS36. In the sample of this research, most patients revealed normal BP levels, a result similar to a study with adults whose age was less than 46 years19,21. This fact is attributed to the large number of patients using antihypertensive drugs for a long time. In addition, these results demonstrate not be indicative of normal blood pressure values in this age group. The prevention of hypertension in early stage, through the practice of physical activity and diet with low sodium, favors the normal BP levels.
Among the individuals here investigated, the results showed that there was a large proportion of sedentary people. This finding showed a value three times higher than a São Paulo origin study, in which 6% of the study population were sedentary and that 90% of these performed some physical activity recommended as protective factor for CVD26. It is worth noting that there's a difference between physical activity and physical exercise. The first is defined as any body movement, produced by the skeletal muscles that results in energy expenditure greater than rest levels, and exercise means a planned, structured, and repetitive physical activity, whose ultimate or intermediary goal is to increase or maintain the health/physical fitness fitness 37. Therefore, one can infer that the patients in this study may be considered active from the point of view of physical activity, but sedentary people regarding the conceptualization of physical exercise.
Altered glucose values were detected in 34.3% of the patients and the type II DM in 13.3%. Such a difference is explained by the use of insulin; some patients received insulin, according to their capillary blood glucose, which may have masked the laboratory tests. Similarly, the mean lipid profile of the patients showed ideal values, justified by the fact that most patients are using cholesterol-reducing drugs.
Although the critical stage of atherosclerosis occurs mostly in middle age, atherosclerotic lesions already start during childhood. In addition, some risk factors cardiovascular (CV), such as hypercholesterolemia, hypertension, tobaccoism and obesity, may have an association with the development of atherosclerosis in adolescents or young adults38. Early detection of modifiable CV risk factors in this population may have an impact in a more advanced age. It is necessary to act with non-pharmacological measures and invest in prevention, with a healthy diet and physical exercise. The literature 29,31 still reference the importance of lipid profile, as a beacon for primary prevention.
However, health professionals, including the nurses, in their practice of caring/educating/researching must be committed as for the provision of information leading this population to reflection, for the awareness of it being adopted in their lifestyle.
CONCLUSION
This research provides data search subsidies for a prospective study with a larger number of subjects. The main risk factors for early acute coronary syndrome among the subjects were family history, tobaccoism and overweight. Of these, the modifiable risk factors may be reduced substantially if there is an investment in promotion and prevention of diseases and cardiovascular lesions responsible for increased morbidity and mortality. One of the ways to act in prevention is to encourage healthy live practices in family culture, strengthening individual conduct in the future.
Among the limitations of this study, it is highlighted that other risk factors, responsible for the development of ACS, as the presence of stress, alcohol use and eating habits were not analyzed, justifying the absence of their association with ACS.
REFERENCES
1.Weinberger I, Rotenberg Z, Fuchs J, Sagy A, Friedmann J, Agmon J. Myocardial infarction in young adults under 30 years: risk factors and clinical course. Clin Cardiol. 1987; 10: 9-15.
2. Maroszyńska-Dmoch EM , Wożakowska-Kapłon B. Coronary artery disease in young adults: clinical and angiographic characterization. A single centre study. Kardiol Pol. 2015; 14:1-17.
3.Chouhan L, Hajar HA, Pompisiello JC. Comparison of thrombolytic therapy for acute myocardial infarction in patients aged <35 and >55 years. Am J Cardiol. 1993; 71: 157-9.
4.Pasricha A, Batchelor W. When young hearts are broken: profiles of premature myocardial infarction. Am Heart J. 2002; 143: 4-6.
5.Doughty M, Mehta R, Bruckman D, Das S, Karavite D, Tsai T, et al. Acute myocardial infarction in the young - the University of Michigan experience. Am Heart J. 2002; 143: 56-62.
6.Cantarelli MJC, Castello Jr HJ, Gonçalves R, Gioppato S, Navarro E, Guimarães JBF et al. Intervenção coronária percutânea em pacientes jovens. Rev Bras Cardiol Invasiva. 2014; 22: 353-8.
7.Avezum A, Makdisse M, Spencer F, Gore JM, Fox KA, Montalescot G, et al. Impact of age on management and outcome of acute coronary syndrome: observations from the Global Registry of Acute Coronary Events (GRACE). Am Heart J. 2005; 149: 67-73.
8.Borba CS, Lemos IGS, Hayasida NMA. Epidemiologia e fatores de risco cardiovasculares em jovens adultos: revisão de literatura. Revista Saúde e Desenvolvimento Humano. 2015; 31: 51-60.
9.Myers L, Coughlin SS, Webber LS, Srinivasan SR, Berenson GS. Prediction of adult cardiovascular multifactorial risk status from childhood risk factor levels. The Bogalusa Heart Study. Am J Epidemiol. 1995; 142: 918-24.
10.Strong JP, Malcom GT, McMahan CA, Tracy RE, Newman WP, Herderick EE, et al. Prevalence and extent of atherosclerosis in adolescents and young adults: implications for prevention from the Pathobiological Determinants of Atherosclerosis in Youth Study. JAMA. 1999; 281: 727-35.
11.Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, Eberlein KA, et al. Blood pressure, stroke, and coronary heart disease. Part 2, Short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet. 1990; 335: 827-38.
12.Theroux P, Fuster V. Acute coronary syndromes: unstable angina and non-Q-wave myocardial infarction. Circulation. 1998; 97: 1195-206.
13.Keys A. The diet and 15-year death rate in the seven countries study. Am J Epidemiol. 1986; 124: 903-15.
14.Krauss RM, Eckel RH, Howard B. AHA dietary guidelines: revision 2000: a statement for healthcare professionals from the Nutrition Committee of the American Heart Association. Circulation. 2000; 102: 2284-99.
15.Santos I, Soares CS, Berardinelli LMM. Promovendo o autocuidado de clientes com obesidade e coronariopatia: aplicação do diagrama de pender. Rev enferm UERJ. 2013; 21: 301-6.
16.Santos LR, Brito ECC, Neto JCGL, Alves LEP, Alves LRA, de Freitas RWJF. Análise do sedentarismo em estudantes universitários. Rev enferm UERJ. 2014; 22: 416-21.
17.Leite AHP, Dantas TS, Rolim LADMM, Silva NQ, Morato CBA. Perfil lipídico em adultos jovens e fatores de risco associados a doenças cardiovasculares REBES.2015; 5 (2): 15-20.
18.Ministério da Saúde (Br). DataSUS [site de Internet]. Sistema de Informações sobre Mortalidade-SIM. [citado em 15 jan 2015]. Disponível em: http://portal.saude.gov.br/portal/-saude/profissional/visualizar_texto.cfm?idtxt=32116&janela=1.
19.Tungsubutra W, Tresukosol D, Buddhari W, Boonsom W , Sanguanwang S, Srichaiveth B. Acute coronary syndrome in young adults: The Thai ACS Registry. J Med Assoc Thai. 2007; 90: 81-90.
20.Aguiar C. Síndrome coronária aguda no jovem: essencialmente uma complicação aterotrombótica evitável. Rev Port Cardiol. 2010; 29: 957-60.
21.Teixeira M, Sá I, Mendes JS, Martins L. Síndrome coronária aguda no jovem. Rev Port Cardiol. 2010; 29: 947-55.
22.Keller T, Zeller T, Ojeda F, Tzikas S, Lillpopp L, Sinning C, et al. Serial changes in highly sensitive troponin I assay and early diagnosis of myocardial infarction. JAMA. 2011; 306: 2684-93.
23.Gus I, Fischmann A, Medina C. Prevalência dos Fatores de Risco da Doença Arterial Coronariana no Estado do Rio Grande do Sul. Arq Bras Cardiol. 2002; 78: 478-83.
24.Sociedade Brasileira de Cardiologia, Sociedade Brasileira de Hipertensão, Sociedade Brasileira de Nefrologia. VI Diretriz Brasileira de Hipertensão. São Paulo: SBC; 2010.
25.V Diretriz brasileira de dislipidemias e prevenção da aterosclerose. Sociedade Brasileira de Cardiologia. Arq Bras Cardiol. 2013; 101(4 Supl.1): 1-22.
26.Viebig R, Valero M, Araújo F, Yamada A, Mansur A. Perfil de saúde cardiovascular de uma população adulta da região metropolitana de São Paulo. Arq Bras Cardiol. 2006; 86: 353-60.
27.Marshall A, Baumann A. The internacional physical activity questionnaire summary report of the reliability and validity studies. Geneva (Swi): IPAQ Excecutive Commite, World Heath Organization; 2001.
28.Schwartz JB, Zipes DP. CaBraunwald E, Bonow RO, Libby P, Zipes DP, editors. Braunwald's heart disease: a textbook of cardiovascular medicine. Philadelphia (USA): Elsevier Saunders; 2005.
29.Caimi G, Valenti A, Lo Presti R. Acute myocardial infarction in young adults: evaluation of the haemorheological pattern at the initial stage, after 3 and 12 months. Ann Ist Super Sanita. 2007; 43: 139-43.
30.Ministério da Saúde (Br). Vigitel Brasil 2006: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Brasília (DF): Ministério da Saúde; 2007.
31.Rosengren A, Wallentin L, Simoons M, Gitt A, Behar S, Battler A, et al. Cardiovascular risk factors and clinical presentation in acute coronary syndromes. Heart. 2005; 91: 1141-7.
32.DeVon H, Ryan C, Ochs A, Shapiro M. Symptoms across the continuum of acute coronary syndromes: differences between women and men. Am J Crit Care. 2008; 17: 14-24.
33.Smith SCJr, Blair SN, Bonow RO, Brass LM, Cerqueira MD, Dracup K, et al. AHA/ACC Scientific Statement: AHA/ACC guidelines for preventing heart attack and death in patients with atherosclerotic cardiovascular disease: 2001 update. Circulation. 2001; 104: 1577-9.
34.Rana JS, Mukamal KJ, Morgan JP, Muller JE, Mittleman MA. Obesity and the risk of death after acute myocardial infarction. Am Heart J. 2004; 147: 841-6.
35.Kaplan RC, Heckbert SR, Furberg CD, Psaty BM. Predictors of subsequent coronary events, stroke, and death among survivors of first hospitalized myocardial infarction. J Clin Epidemiol. 2002; 55: 654-64.
36.Conti R, Solimene M, Luz P, Benjó A, Neto P, Ramires J. Comparação entre homens e mulheres jovens com infarto agudo do miocárdio. Arq Bras Cardiol. 2002; 79: 510-7.
37.Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985; 100: 126-31.
38.Jee-Aee Im, Ji-Won Lee, Jae-Yong Shim, Hye-Ree Lee, Duk-Chul Lee.Association between Brachial-Ankle Pulse Wave Velocity and Cardiovascular Risk Factors in Healthy Adolescents The Journal of Pediatrics. 2014 ; 150: 247–51.