*There was ignored information
RESEARCH ARTICLES
Neonatal mortality: analysis of preventable causes
Maria Aparecida Munhoz GaivaI; Elizabeth FujimoriII; Ana Paula Sayuri SatoIII
I
Ph.D. in Nursing. Associate Professor 3 from the Federal University of Mato Grosso, Nursing Shcool. Cuiabá, Mato Grosso, Brazil. Researcher of the National
Council of Scientific and Technological Development. E-mail: mamgaiva@yahoo.com.br
II
Ph.D. in Nursing. Associate Professor 3 of the Nursing School at the University of São Paulo, Collective Health Nursing Department. São Paulo, Brazil.
Researcher of the National Council of Scientific and Technological Development. E-mail: efujimor@gmail.com
III
Ph.D. in Nursing. Ph.D. Professor form the Public Health School of the University of São Paulo, Epidemiology Department. São Paulo, Brazil. E-mail:
sah@usp.br
Research funded by CNPq, universal edict 14/2012, process nº 471609/2012-9
DOI: http://dx.doi.org/10.12957/reuerj.2015.5794
ABSTRACT
This cross-sectional study to examine neonatal deaths in Cuiabá, Mato Grosso against the List of Causes of Death Preventable by Intervention by National Health System (SUS) Services, was conducted with data from the Information Systems on Live Births (SINASC) and Mortality (SIM) for 2010. Of total deaths, 81.1% were preventable, 47.2% were due to inadequate care for newborns, 21.6% to inadequate care for women during pregnancy and 12.2% to inadequate care during labor. The high percentage of neonatal deaths from inadequate care in the SUS shows unfavorable conditions of antenatal and neonatal care in the municipality, underlining the need for investments in service structure and capacity building for professionals.
Keywords: Neonatal mortality; surveillance; information systems; underlying cause of death.
INTRODUCTION
The infant mortality rate, which includes the neonatal and post-neonatal periods, is one of the best indicators of living conditions and health of a population1.
Over the past three decades, the infant mortality rate has decreased in the country, mainly by reducing post-neonatal mortality (deaths occurring from the 28th day up to one year old). However, neonatal mortality has not shown significant changes and, in 2008, had 68% of deaths in the first year of life1.
The neonatal component that is the deaths occurred in the first 27 days of life, is distributed in early neonatal mortality (deaths occurring in the first 7 days of life) and late (deaths from the 7th to 27th day of life), reflecting socioeconomic and maternal health conditions, and the quality of care provided in prenatal care, childbirth and newborn2.
There is evidence that more than 70% of neonatal deaths occur from preventable causes, especially lack of proper care to pregnant women and the newborn 2-4. Prematurity is highlighted as the main cause of child deaths in the first week of life in all regions of the country and the second cause of death is asphyxia/hypoxia in the North and Northeast regions, and in other regions is dominated by congenital malformations5.
The risk of neonatal death is respectively 44 and 50 times higher among infants with low birthweight (<2,500 g) and preterm (gestational age <37 weeks), as it is 54 to 125 times higher when the Apgar is less than 7 at the first and 5th minutes, respectively6.
Thus, to analyze neonatal deaths according to considered preventable causes of death can enlarge the understanding of pathological events involving the mother and child during pregnancy and childbirth and leading to death2. In this sense, several studies have examined the causes of neonatal and child deaths under the focus of avoidable3,7-10, in order to identify situations that require investments to improve health care11.
Seeking to contribute to the examination of the topic, this study aimed to analyze the neonatal deaths according to the List of Causes of Death Preventable by Interventions in the Area of the Unified Health System (SUS).
LITERATURE REVIEW
Preventable causes of death are those preventable, totally or partially, through effective health services that are accessible in one place and period 12, defining diagnostics on the health care network.
Many causes of neonatal deaths are considered preventable from adequate access and quality care assurance with regard to prenatal, childbirth and puerperium2, especially through early and accurate diagnoses and interventions13.
In recent years, the discussion and the scientific literature about avoidable infant deaths has been important by pointing out both successful actions as the gaps and weaknesses in the organization of services and in the work process of health professionals in care for women and child13.
Several classifications have been used for the analysis of avoidable death, highlighting the Deaths List of Causes of Preventable by Interventions in the SUS Area, built for the Brazilian reality12. For children under five years old, this list ranks: preventable causes (reducible by vaccine prevention activities, by providing specialized care to women during pregnancy, childbirth and newborn care, by appropriate actions of diagnosis and treatment and appropriate actions health promotion, linked to appropriate actions health care); non-defined causes; and other causes (those clearly unavoidable).
In this way, identifying and monitoring the causes of avoidable death in the focus are important steps, as they allow the construction of sensitive indicators to the quality of health care, having research mechanisms to explain the deaths and trigger actions to reduce it14.
Therefore, the analysis of deaths by potentially preventable or reduced causes through interventions under the SUS area subsidizes the management and planning of preventive and care interventions because it provides essential elements to improve the production and health care14.
METHODOLOGY
This is a retrospective cross-sectional study which analyzed mortality data occurred in 2010 in Cuiabá, capital of Mato Grosso (MT), which in that year had a population of 551,350 inhabitants and Human Development Index (HDI) of 0.82115.
Data were obtained from the Live Birth Information System (SINASC) and Mortality Information System (SIM) provided by Surveillance Births and Deaths Management of Municipal Health Secretary of Cuiabá, MT. Databases were related by linkage technique, with the use of the variables declaration number of birth, mother's name and child's birth date.
In 2010, there were 9,349 live births (LB) and 81 neonatal deaths recorded in information systems. Information was obtained on SINAC referring to 74 newborns, resulting in linking 91.4%, with loss of five newborn deaths that were not included in that system and deleting two who were not mothers living in Cuiabá. Thus, data were analyzed in 74 infants who died in the neonatal period, 56 died in the early neonatal period and 18 in late neonatal period.
The cause of death was obtained in SIM, which has reference to the International Classification of Diseases, 10th Revision (ICD-10).
For data analysis, as a reference the Deaths List of Causes of Preventable by Interventions in the SUS Area for children under five years old was used 12.
To calculate the neonatal mortality rate (NMR), the number of child deaths 0-27 completed days of life was divided by the total number of live births in 2010 and multiplied the result by one thousand. It proceeded in the same way to calculate the early neonatal mortality rates (ENMR) and late (LNMR), when it was used in the numerator the number of child deaths 0-6 completed days of life and the number of deaths of children 7 to 27 completed days of life, respectively.
The original databases, stored in Tabwin, were transformed into Microsoft Excel 2007 spreadsheets and analyzed using descriptive statistics with distribution of absolute and relative frequencies.
The research project was approved by the Research Ethics Committee (CEP) of the University Hospital Júlio Muller (HUJM of the Federal University of Mato Grosso), according to the Protocol 968 / CEP-HUJM / 2010.
RESULTS AND DISCUSSION
The neonatal mortality rate of mothers living in the city of Cuiabá in 2010 was 7.9 per thousand LB, being 6.0 per thousand LB in the early neonatal period, with a high concentration of deaths in the first 24 hours of life (29.7 %, n=22) and 1.9 per thousand LB in late neonatal period.
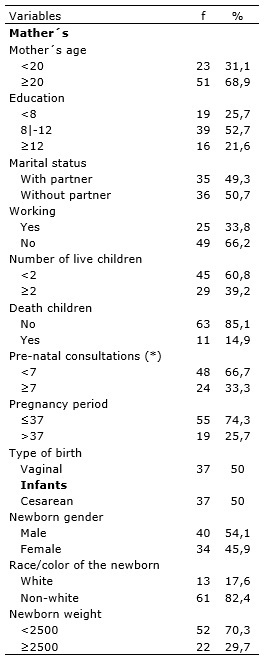
About a third of mothers were adolescents (<20 years old), half had between 8 and 11 years of study, two-thirds did not work and had less than seven prenatal visits. Greater proportion of infants who died in the neonatal period were male (54.1%) non-white (82.4%) were born preterm (74.3%) and underweight (70.3%) as shown in Table 1.
TABLE 1: Distribution of mother´s characteristics, pregnancy, childbirth and newborns who died in Cuiabá (MT), Brazil, 2010.
*There was ignored information
In 2010, the neonatal mortality rate in Cuiabá (7.9 deaths per thousand LB) was below the coefficients found in 2009 in the country (10.1 deaths per thousand LB) in the State of Mato Grosso (10.3 deaths per thousand LB) and Cuiabá (10.2 deaths per thousand LB)5,16. However, despite this decline, the index is far from being adequate, as in developed countries like the United States and Canada, the coefficients in 2009 were below 4 (3.9 deaths and 2.9 deaths per thousand LB, respectively), and even in countries of South America, such as Chile (3.8 deaths per thousand LB)17. Nevertheless, the coefficient found in Cuiabá is below the agreed at the Municipal Health Plan 2010-2013, which proposed reducing the neonatal mortality rate in the municipality at 5% per year, from 10.3 in 2008 to 8.6 deaths per thousand LB by December 201318.
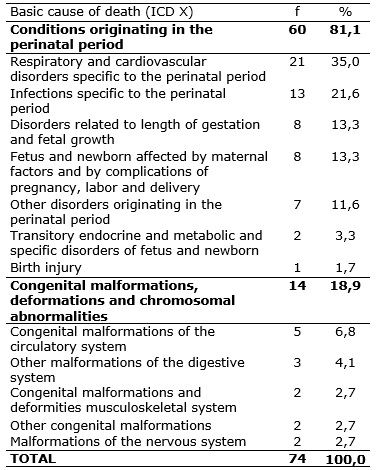
As basic causes of neonatal deaths there are disorders originating in the perinatal period (n=60), highlightingRespiratory and cardiovascular disorders specific to the perinatal period, having about a third of deaths (35%), followed by deaths from specific perinatal infection (21.6%). Also as causes of death there were the Disorders related to length of gestation and fetal growth (13.3%), especially very low birth weight and extreme immaturity, and Fetus and newborn affected by maternal factors and by complications of pregnancy, labor and delivery (13.3%), as shown in Table 2.
TABLE 2: Distribution of basic cause of death- Cuiabá (MT), Brazil, 2010.
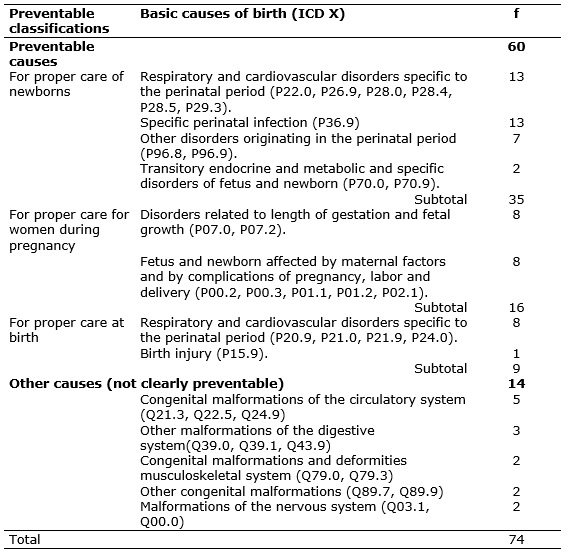
The disorders originating in the perinatal period have been the leading cause of neonatal death in the country5,19.20. In Cuiabá, among these disorders, respiratory and cardiovascular disorders and infections specific to the perinatal period accounted together for 35.2% of deaths preventable by proper care of newborns, according to Table 3. This high percentage differs from what occurred in Brazil from 1997 to 2006 when deaths from perinatal causes such as intrauterine hypoxia, birth asphyxia and neonatal aspiration decreased, probably due to increased access to care during labor and advances in care in the immediate postpartum period, especially for access to intensive neonatal care and the use of surfactant in SUS hospitals 7.
TABLE 3: Distribution of preventable situations according to the basic cause of death. Cuiabá (MT), Brazil, 2010.
Mortality analysis of neonates less than 32 weeks and weighing 1,500 g also identified the respiratory distress syndrome as the leading cause of death and noted that the drop in NMR coincided with the implementation of specific equipment and resources in neonatal units and use of surfactant and antenatal corticosteroids21.
In Cuiabá, from the total number of deaths analyzed, 81.1% were preventable interventions under the SUS area, highlighting those for adequate attention to the newborn (47.3%), similar to results obtained in other studies8,20,22. In addition, 21.6% were preventable by proper care for women during pregnancy and 12.2% for adequate care for women in childbirth, according to Table 3.
Among the causes of preventable deaths by providing specialized care to newborns, there are highlightedthe respiratory and cardiovascular disorders (hialiana membrane disease and respiratory failure) and the specific infection of the perinatal period (septicemia). For proper care for women during pregnancy, as preventable causes of death there were the Disorders related to length of gestation and fetal growth (prematurity and low birth weight); and among the preventable deaths by adequate care during labor, the respiratory and cardiovascular disorders (birth asphyxia and meconium aspiration), as shown in Table 3.
Thus, despite the NMR in Cuiaba be less than in the State and the capital in the previous year, the result is worrying because more than 80% of neonatal deaths resulted from preventable causes. This index confirms study findings developed in Recife, also capital of the state, where 78.4% of neonatal deaths from 1999 to 2009 were preventable3. High rates of preventable deaths were also observed in a cohort of children of Pelotas, Brazil, where 79.2% of deaths in the first year of life were preventable, and most of them (63.4%) were neonatal deaths4. Another study, also conducted in Pelotas, showed that from 266 infant deaths that occurred from 2005 to 2008, 72.9% were preventable19.
Compared to another study conducted in Cuiabá in 20079, there was an increase of almost 10% in preventable deaths by providing specialized care to newborns (from 38% to 47.3%) and decreased 10.4% in deaths preventable by proper care for women during pregnancy, maintenance of deaths that could be avoided by adequate care during labor.
These results differ from what happened in the country from 1997 to 2006, when there was decrease of 42.5% in the percentage of preventable deaths by providing specialized care to newborns, reducing 27.7% of deaths preventable by adequate care to childbirth and 28.6% of preventable deaths by providing specialized care to women during pregnancy7.
Considering that the access to prenatal care has expanded, it is strange the increase in the percentage of preventable deaths by providing specialized care to women during pregnancy. A study that analyzed the deaths occurred during a decade in Recife, found that of 2,267 preventable deaths, 41% would be for adequate care during pregnancy3. In Pelotas, the infant deaths that occurred between 2004 and 2008, 63.1% could have been avoided by proper care to women during pregnancy4, and in Londrina, PR, 32.8%22. However, as in Cuiabá, in Natal, RN, was identified lower percentage (22.6%) of preventable deaths by providing specialized care to women during pregnancy13.
The increase in prenatal coverage rate in recent years in Cuiabá, may explain in part the decrease in the number of preventable deaths by providing specialized care to women during pregnancy, but the high percentage (66.7%) of pregnant women is worrying with less than 7 prenatal visits found among mothers of infants who died in the neonatal period. This result is a warning to health services because prenatal care is recognized for its positive impact on neonate survival23,24, not restricted to access to consultations, but also with regard to quality of care provided24,25 , prenatal being a favorable period for the implementation of actions to prevent and combat neonatal mortality4,25.
Although low birth weight and preterm birth are the result of complex determinants, such as environmental conditions and antenatal maternal health, the occurrence of these events is also linked to the quality of pre-natal care2,6,13. Currently, these are the causes of most relevant neonatal mortality, and in this study, nearly three-quarters of neonatal deaths (70.3%) occurred in infants of low birth weight (less than 2,500g), similarly to the observed in other capital of the State (74.4%)3. This result also highlights the need to invest in improving prenatal care quality, especially as the prevalence of underweight births has been stable in the country since early 1990, averaging 8% of total live births26.
Current data from the World Health Organization classifies Brazil as the tenth country in the world with the highest number of preterm births, with a prevalence of 9.2%27. Moreover, in recent years, its occurrence was in more than half of neonatal deaths, especially in children born with extremely low birth weight 28.
Regarding the deaths preventable by proper care for women in childbirth, the percentage found in Cuiabá (12.2%) is similar to the 13.3% observed in Brazil in 20067 and 15.5% recorded in 16 cities in the state of Mato Grosso do Sul, from 2000 to 200211.
The pattern of preventable neonatal deaths found in this study suggests the existence of problems related to maternal and child care and indicates the need for investments in the structure of services and the training of professionals to meet the woman in pregnant and childbirth and the newborn, priority in the immediate postpartum period.
Knowing the causes of death, especially those preventable by proper care is therefore essential to assess the performance of services and monitor the quality of care provided by the healthsystem7,13,14.
It is important that in this study we worked with data from a Brazilian state capital of referring to one year, so the results should be interpreted in the regional context. However, it is important to show that the analysis of deaths by preventable criteria is an important tool to assess the quality of health care. In addition, the classification of causes of death can be considered as a first step to a better understanding of the determinants of neonatal mortality in the context of preventing them14.
CONCLUSION
The high percentage of preventable neonatal deaths through appropriate care under the SUS area indicates that there is in the city of Cuiabá, unfavorable conditions of care for pregnant women and newborns to reinforce the need for investments in the structure of services and training of professional, to improve the quality of care provided to women in prenatal care services and the newborn, especially the care provided immediately after birth.
One limitation of this study refers to the fact that it is of secondary data analysis, which depends on the reliability and completeness of filling out records. The use of linkage technique databases, however, proved to be useful and feasible to be used by local managers to face the neonatal mortality.
Finally, there is the importance of information systems and analysis of preventable deaths according to criteria such as tools to evaluate and monitor the quality of health care.
REFERENCES
1.Victora CG, Aquino EML, Leal MC, Monteiro CA, Barros FC, Szwarcwald CL. Maternal and child health in Brazil: progress and challenges. Lancet. 2011; 377:1863-76.
2.Ministério da Saúde (Br). Secretaria de Vigilância em Saúde. Manual de vigilância do óbito infantil e fetal e do Comitê de Prevenção do Óbito Infantil e Fetal. Brasília (DF): Ministério da Saúde; 2009.
3.Rocha R, Oliveira C, Silva DKF, Bonfim C. Mortalidade neonatal e evitabilidade: uma análise do perfil epidemiológico Rev enferm UERJ. 2011; 19:114-20.
4.Gorgot LRMR, Santos I, Valle N, Matisajevich A, Barros AJD, Albernaz E. Óbitos evitáveis até 48 meses de idade entre as crianças da coorte de nascimentos de Pelotas de 2004. Rev Saude Publica. 2011; 45:334-42.
5.Ministério da Saúde (Br). Saúde Brasil 2011: uma análise da situação de saúde e a vigilância da saúde da mulher. Secretaria de Vigilância em Saúde. Brasília (DF): Ministério da Saúde; 2012. [citado em 19 out 2014]. Disponível em: http://portalsaude.saude.gov.br/portalsaude/arquivos/pdf/2013/Fev/21/saudebrasil2011_parte1_cap1.pdf
6.Maran E, Uchimura TT. Mortalidade neonatal: fatores de risco em um município no sul do Brasil. Revista Eletrônica de Enfermagem. [Internet]. 2008. [citado em 16 out 2014]. Disponível em: http://www.fen.ufg.br/revista/v10/n1/v10n1a03.htm
7.Malta DC, Duarte EC, Escalante JJC, Almeida MF, Sardinha LMV, Macário EM et al. Mortes evitáveis em menores de um ano, Brasil, 1997 a 2006: contribuições para a avaliação de desempenho do Sistema Único de Saúde. Cad Saúde Pública. 2010; 26:481-91.
8.Jobim R, Aerts D. Mortalidade infantil evitável e fatores associados em Porto Alegre, Rio Grande do Sul, Brasil, 2000-2003. Cad Saúde Pública. 2008; 24:179-87.
9.Lourenço EC, Bruken GS, Luppi CG. Mortalidade infantil neonatal: estudo das causas evitáveis em Cuiabá, Mato Grosso, 2007. Epidemiol Serv Saúde. 2013; 22:697-706.
10.Jodas DA, Scochi MJ, Vicente JB, Colucci AG. Análise dos óbitos evitáveis de menores de cinco anos no município de Maringá-Pr. Esc Anna Nery. 2013; 17:263-70.
11.Gastaud ALGS, Honer MR, Cunha RV. Mortalidade infantil e evitabilidadae em Mato Grosso do Sul, Brasil, 2000 a 2002. Cad Saúde Pública. 2008; 24:1631-40.
12.Malta DC, Duarte EC, Almeida MF, Dias MAS, Moraes Neto OL, Moura et al. Lista de causas de mortes evitáveis por intervenções do Sistema Único de Saúde do Brasil. Epidemiol Serv Saúde. 2007; 16:233-44.
13.Brandão ICA, Godeiro ALS, Monteiro AI. Assistência de enfermagem no pré-natal e evitabilidade de óbitos neonatais. Rev enferm UERJ. 2012; 20:596-602.
14.Malta DC, Duarte EC. Causas de mortes evitáveis por ações efetivas dos serviços de saúde: uma revisão da literatura. Ciênc saúde coletiva. 2007; 12:765-76.
15.Mato Grosso (Br). Secretaria de Estado Planejamento e Coordenação Geral [Internet]. Mato Grosso em números. [citado em 18 out 2014] Disponível em: http://www.seplan.mt.gov.br/sitios/indicador/mtemnumeros2010/pdf/aspectossociais.pdf
16.Cuiabá (MT). Secretaria Municipal de Saúde de Cuiabá. Indicadores de mortalidade de Cuiabá e referencial comparativo – 1997/2009. Cuiabá (MT): Secretaria Municipal de Saúde; 2010.
17.Rajaratnam JK, Marcus JR, Flaxman AD, Wang H, Levin-Rector A, Dwyer L et al. Neonatal, post neonatal, childhood, and under-5 mortality for 187 countries, 1970–2010: a systematic analysis of progress towards Millennium Development Goal 4. The Lancet. [Internet]. 2010. [cited in 2014 Aug 16]. Available in: http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(10)60703-9/abstract
18.Cuiabá (MT). Secretaria Municipal de Saúde de Cuiabá. Plano municipal de saúde 2010-2013. Cuiabá (MT): Secretaria Municipal de Saúde; 2010.
19.Silva VLS, Santos IS, Medronha NS, Matijasecich A. Mortalidade infantil na cidade de Pelotas, Estado do Rio Grande do Sul, Brasil, no período de 2005-2008: uso da investigação de óbitos na análise das causas evitáveis. Epidemiol Serv Saúde. 2012; 21:256-74.
20.Ferrari RAP, Bertolozzi MR, Dalmas JC, Girotto E. Determining factors for neonatal mortality in a city in the Southern Region of Brazil. Rev esc enferm USP. [Internet]. 2013. [cited in 2014 Jun 22]. Available in: http://www.scielo.br/pdf/reeusp/v47n3/en_0080-6234-reeusp-47-3-00531.pdf
21.Barría-Pailaquilén RM, Mendoza-Maldonado Y, Urrutia-Toro Y, Castro-Mora C, Santander-Manríquez G.Trends in infant mortality rate and mortality for neonates born at less than 32 weeks and with very low birth weight. Rev Latino-Am Enfermagem. 2011; 19:977-84.
22.Santos HG, Andrade SM, Silva AMR, Mathias TAF, Ferrari LL, Mesas AE. Mortes infantis evitáveis por intervenções do Sistema Único de Saúde: comparação de duas cortes de nascimentos. Ciênc saúde coletiva. 2014; 19: 907-16.
23.Kassar SB, Melo ANC, Coutinho SB, Lima MC, Lira PIC. Determinants of neonatal death with emphasis on health care during pregnancy, childbirth and reproductive history. J Pediatr. 2013; 89:269-77.
24.Nascimento RM, Leite AJM Almeida NMGS, Almeida PC, Silva CF. Determinantes da mortalidade neonatal: estudo caso-controle em Fortaleza, Ceará, Brasil. Cad Saúde Pública. 2012; 28:559-72
25.Borba GG, Neves ET, Arrué AM, Silveira A, Zamberlan KC. Fatores associados à morbimortalidade neonatal: um estudo de revisão. Saúde (Santa Maria). 2014; 40:09-16.
26.Silva AAM, Silva LM, Barbieri MA, Bettiol H, Carvalho LM, Ribeiro VS, Goldani MZ. The epidemiologic paradoxo flow birth weight in Brazil. Rev Saude Publica. 2010; 44: 767-75.
27.World Health Organization. Born too soon: the global action report on preterm birth. Geneva (Swi): WHO; 2012.
28.Almeida MF, Alencar GP, Schoeps D, Novaes HMD, Campbell O, Rodrigues LC. Sobrevida e fatores de risco para mortalidade neonatal em uma coorte de nascidos vivos de muito baixo peso ao nascer, na Região Sul do Município de São Paulo, Brasil. Cad Saúde Pública. 2011; 27:1088-98.