RESEARCH ARTICLES
Profiling health and disease in oldest-old primary health care users
Letice de Freitas PereiraI; Maria Helena LenardtII; Tatiane MichelIII; Nathalia Hammerschmidt Kolb Carneiro IV; Leandra de Fátima BentoV
INurse at the Colombo City Administration, Paraná, Brazil. E-mail: letice_freitas@hotmail.com
IINurse. Ph.D in Philosophy of Nursing.Senior Professor at the Graduate Program in Nursing of the Universidade Federal do Paraná.
curitiba.helena@gmail.com
IIINurse.Ph.D in Nursing. Member of the Multiprofessional Research Team on the Elderly.Curitiba, Paraná, Brazil. E-mail: tatiane.michel@uol.com.br
IVNurse.Ph.D. candidate with the Graduate Program in Nursing of the Universidade Federal do Paraná.Holds a scholarship withReuni.Member of the
Multiprofessional Research Team on the Elderly.Curitiba, Paraná, Brazil. E-mail: nathalia.kolb@gmail.com
VNurse at the Curitiba City Administration. Expert in Nursing Services Managementand Public Management in Health.MBA in HumanResources Management.
Curitiba, Paraná, Brazil. E-mail: leandradefatimabento@hotmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2015.5069
ABSTRACT
This quantitative, descriptive, transversal study aimed to profile the health and disease status of older-old primary health care users. Study participants were 100 older adults 80 or more years old, selected on inclusion and exclusion criteria during the sample period from February to April 2011. Data were collected by adapted, semi-structured questionnaire, and analyzed using descriptive statistics. The results revealed a profile consisting of sedentary oldest-old, with chronic diseases and comorbidities, who report healthy living habits, assess their health as fair, use various drugs, and whose main leisure activities are television and household chores. The findings reveal a need to encourage activities that foster socialization, since sharing experience can provide better self-care, prevent sedentary lifestyle, and intensify control of diseases and medicines.
Keywords: Aged, 80 and over; geriatric nursing; longevity; health center
INTRODUCTION
Demographic changes are a world phenomenon and have generated discussion on both elderly-related public policies and health services and care. Increase in the elderly population has brought about social challenges, such as heavier load of diseases, disabilities, and higher demand for hospital health care 1.Every year new ranks of elderly join the Brazilian population. Those aged 80 or older make upover 12% of the elderly population2. The Brazilian state of Paraná is outstanding for the highest ranks of people in their 100's (933)3, and is home now for 147,193elderly over 80, of which 27,630 are concentrated in the city of Curitiba4.
Population longevity seriously affects several sectors, such as the social, health, and economic areas.The search for longevity and extended health quality and wellbeingturns out to be one of the most relevant values in all human history5. However, health problems affecting the older elderly are still under investigated by health services and researchers. Therefore, littleisknownaboutthem.
Thus, it becomes relevant to assess the specific characteristics and health-disease conditions of older elderly. Data assessment and analysis provide local-specific subsidies for the development of new research as well as it allows nursing professionals to act in health promotion and prevention of diseases and disabilities and to help higher life quality of the long-lived.
In view of those considerations, this study aimed at drawing the health-disease profile of the older elderly on primary health care.
LITERATURE REVIEW
The scarse studies concerned with that age group enhance cognitive decline, presence of comorbities, functional dependence, and depression as outstanding problems. In addition to their inter relation, such health conditions turn out to be relevant mortality predictors6. Other authors7 draw attention both to a deficit in knowledge concerning the health of the elderlyon the basis of the lack of scientific production on that age group and to the need of scientific attention to that theme. Likewise, little is known about the health-disease profile of long-lived elderly on primary health care. National statistics institutes bring out just the data on the group aged 60 or over, and frequently, information on older groups are not specific.
The age segment for older elderly showsspecific morphophysiological, psychological, and socioeconomic characteristicsapart even from those found among younger elderly. Therefore, there is outstanding heterogeneity among the elderly and meaningful differences betweenthe younger ones (60-79 years) and those aged 80 or older8.
METHODOLOGIES
This is a quantitative descriptive cross sectional study, conducted both at a Primary Healthcare Unit (PHU) and at the residence of the elderly users at the municipality of Curitiba, Paraná, Brazil. The PHU reaches 19 thousand inhabitants and about 1,600 registered elderly.About 23 elderly receive some kind of treatment at that uniton a daily basis. The elderly population aged 80 years or older with registration with PHU programs comprised 109 subjects in January, 2011.
The following inclusion criteria were used for the selection of the participants in this study: to be 80 years or older; to be registered at the selected PHU; and to be above cut-off points on the Brief Exam for Mental State Assessment (MEEM) 9: 13 points for the illiterate; 18 points for low and average schooling levels; and 26 points for those with high schooling levels.Exclusion criteria in this research reached the elderly with strong communication impedimentsand lacking a family caregiver who couldfacilitate the address to the questionnaire.
Out of the long-lived elderly registered at the PHU, six resided no longer in the neighborhood, two did not accept to take part in the study, and one was deceased. Therefore, the sample was comprised of 100 long-lived elderly on the basis of inclusion and exclusion criteria within the sample period from February to April, 2011. Out of those, five showed communication impediments, and nine showed cognitive alterationstraced down by means of the MEEM, which prevented them from answering the questionnaire. In those cases, the family caregiver was invited to join. Inclusion criteria for that caregiver were as follows to be a familycaregiver to the elderly either showing communication impediments or with a MEEM score below cut-off point levels; to reside with the long-lived elderly; to be 18 years or older.
Data collection was made on both primary and secondary sources and was conducted over two moments: first, with an investigation intomedical records and phone contact with potential long-lived elderly; second, application of both the MEEM and the questionnaire.
Medical records of those elderly aged 80 or older were investigated for collection of identification data (name, age, address, and phone number). Then, phone calls were made to check on the elderly's willingness and availability to be research subjects. Of the total 100 long-lived elderly, 42% answered the questionnaire at the PHU and 58% at their residences.
To identify health-disease profile characteristics, a semi structured questionnaire10 was adapted for use in this study, with questions related to the participants' health state, medication taken, services used, background information on falls, hospitalization, living habits, and adoption of assistive technologies.
Collected data was transcribed on version 6.04 of Excel e Epi Infosheets, analyzed by means of descriptive statistics, and presented by means of tables. Ethical volunteer and free consent standards were observed, in accordance to Resolution 196/9611. Project was approved by the Ethics Committee of the Health Sciences Sector, according to the opinion registered under number 0107.0.091.091-10.
RESULTS AND DISCUSSION
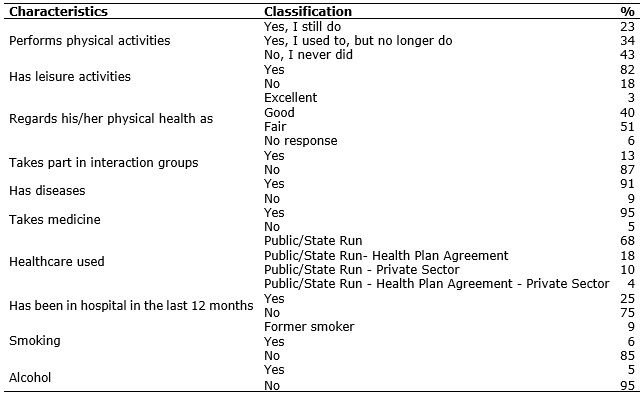
Considering the health-disease profile of those 100 long-lived elderly on primary health care at the PHU participating in this study,43% never exercised; 34%no longer do; and 23%still do. Out of the latter, 16%are into walking, 3%into stretching,3%into working out and1%into riding a bike for the sake of exercising. See Table 1.
Table 1: Health-Disease and Living Habits of Older Elderly: Level Profile (%). Curitiba - PR, 2011. (N=100)
Results showed that most older elderly were sedentary (77%), although 34% of them had already taken to exercising at one point or another in their previous course of life. Therefore, sedentary living levels are found to be high in the sample under analysis, especially in view of studies conducted with 129 long-lived elderly residing in São Geraldo, in the state of Minas Gerais (MG)12, which revealed a figure of 31% for sedentary older elderly.
Long-lived elderly women in particular are likely to decrease their physical activity levels as they grow older12. Sedentary levels among the long-lived elderly can be partially explained on the basis of the very physiological ageing process which, as time goes by, results in the decrease of muscle mass, loss of bone mass, muscle atrophy, all of which are hindrances accounting for the decrease in physical activities.
Physical activities can help the elderly in their independence for longer, and can bring down risks of their falling down.Therefore, physical activities must be a priority also onolder age levels, considering possible benefits attained.13,14.
Most leisure activities by long-lived elderly were as follows:watching television(29%), followed by house chores (19%) and hand work (15%). Travelling stands out among least frequent activities, pointed out by just 3%of the participants.
Active living improves mental health and frequently promotes social contacts13. However, most leisure activities reported were conducted by most long-lived elderly in their own residences, and, therefore that favors sedentary living and social isolation even further. A similar finding was registered in a study with 271 womenresiding in Uberaba (MG), all of which in their 80's.Seventy nine point three per cent (79.3%) reported watching television, and 59.5% reported listening to the radio, 70.4% of which are happy with their leisure activities.15.
It must be enhanced that just 12%of the long-lived elderly in this study took part in interaction groups such as those of senior citizens and volunteers, and, 1%in therapy groups for hyper tension. Low group participant levels among the elderly were equally found in other studies, as in the research developed with 197 elderly of both sexes in Belo Horizonte (MG), in which the long-lived were in the lowest participant level ranks. 16.Higher dependence and comorbities16, limited access, and lack of information on the activities meant for them17account for their limited participation.Active ageing requires support and active participation of the elderly in economic development, formal and informal work, and volunteer activities, according to their personal needs, preferences, and skills.13. Besides, the year 2012 was held as the European Year for Active Ageing and Solidarity among Generations, and whose central aim was "to affect, to disseminate good practices, and to encourage political authorities and interested parties to facilitate active ageing"18:9. This way, European Union governments are expected to develop actions to promote social inclusion of the elderly in a more active way.Suchinitiativescan stand out as examplestoBrazil.
To the majority (51%) of the long-lived elderly participating in this study, their health was found fair (51%); 40% found it good , and just 3%held it as excellent, according to Table 1.Self-health evaluation has been used as an indicator to well-being in research with the elderly, and is regarded as a predictor to morbidity, disability, and inactivity. Those factors can contribute to the worst self-evaluation in health among the population aged 80 or older; however, few pieces of research have focused on that age segment.
On a poll in the municipality of Campinas (SP) with 1,432 long-lived elderly, 64.5% evaluated their health as good, 24.6% as excellent or very good, and just 10%found it poor19.Thosefindingsconstrastwiththeresults in thisresearch.
The number of older elderly evaluating their health as good was expressive. However, all of them reported at least one chronic disease. Out of the 100 participants, just 9% denied any type of disease whereas 91% admitted to one or more, and reported up to nine comorbities. Reported diseases were spread over outstanding ranks as blood hypertension (67%),osteomuscular complications(39%), followed by diabetes mellitus (27%) and cardiovascular conditions(20%).
Self-perception about health can be compromised in cases of diseases that do not frequently show strong manifestation and that can be more silent as hypertension. Still, the reported conditions turn out to be chronic, which can get the elderly to be used to signals and symptoms, since medication minimizes symptomatology.
Those elderly aged 80 or older show the highest frequency of chronic diseases on a clinic basis. Results of this investigation come together with those findings in nation-wide studies. Emphasis is given to the research conducted with 2,136 elderly residing in São Paulo (SP), who likewise reported on hypertension (53.3%) and rheumatic diseases (38,3%) as the most outstanding with that population20.
Most long-lived elderly (95%) reported on the use of one or more medications according to Table 1. On average they use 2.6 pieces of medication (minimum=1and maximum=11), ranked as anti-hypertensive (83%), diuretic (26%), platelet antiaggregant(18%), anti-lipid (18%) andpain relievers (17%).
Polypharmacyhas been associated to advanced age in many studies 12,21. Those pieces of research enhance that the elderly show higher frequency of chronic-degenerative diseases, whose control and prevention of sequels require regular use of medication. One of those studies21, which aimed at characterizing the use of medication by 667 elderlyresiding in Belo Horizonte (MG), showed significant statistics on the use of medication among those aged 80 or older.
Simultaneous use of several medications by the long-lived implies attention by professionals about inadequate use, which can cause serious health damage. Iatrogenic effects at advanced age can occur on account of medicinal interactions, unpredictable reactions, and falls associated to the use of psychotropics13. Incidence of adverse reactions caused by the administration of medications proportionately increases with age2. The long-lived elderly frequently display several factors which can predisposethem to adverse effects in pharmacological therapies. Thus, both sound and controlled drug use among the long-lived, and the observance of professional guidance to the elderly and their families must be enhanced.
As for the use of health services, this research revealed that 68% of the long-lived elderly resort to public/state-run healthcare and 25% had been in hospital in the past 12 months, according to Table 1. Those data are similar to those found among 271 women aged 80 yearsor older, residing in the urban area in Uberaba (MG), in which 50% reported priority use ofpublic health care and 31.1% had been in hospital in the past 12 months15. Thus, preparation of both health centers and professionals to cope with the demands generated by population ageingis enhanced in view of the priority use of public/state-run health care by the elderly as well as of a prospectiveranking for the Brazilian populationas the sixth with the highest number ofelderly by202513,.
Concerning living habits, 85% of the participants reported non-smoking habits; 9%have quit smoking for over 20 years; and 6%still smoke.Out of these, 2%have smoked for over 30 years and 4% have smoked for less than 30 yearsAlcohol consumption was reported by 5% of the older elderly.
Participants in this study reported on healthy living habits. Another study involving subjects with that age group confirms those allegations20. However, it is ignored what the older elderly make of healthy habits and it can be understood that real meaning ascribed ties in with cultural issuesEthnographic research might provide sounder address to that issue.
As for assistivemobility technologies, most part(73%) of the long-lived do not make use of them; 21%have canes, 5%are wheeledand 1% is in bed. Out of the 100 elderly participating, 31% have fallen down in the past 12 months. Still 69% of them reported wearing glasses, 15% of them just for reading, and85% do not make use of hearing apparatuses. See Table 2.
TABLE 2:
Assistive Technologies and Oral Conditions of Older Elderly: Level Profile (%). Curitiba - PR, 2011. (N=100)
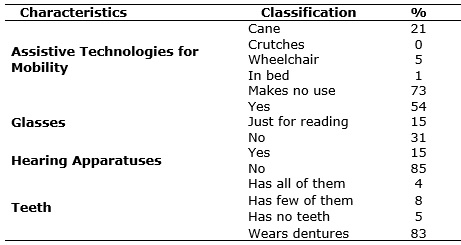
This research showed that most older elderly use neither mobility nor hearing aids. However, the need for that assistive technology was identified with several of them. A study developed with 137 residents in Rio Grande do Sulto evaluate living, health and support conditions of older elderly revealed that 27.7% use canes and 27.7% lean against the furniture as a means to aid mobility22.
It is understood that the use of assistivemobility apparatuses can make a difference for ensuring independence and self-reliance among the elderly. The use of assistive technologies can improve the elderly's capability in their daily activities in the most independent way possibleDeficiency compensation is highly recommendable for active ageing13, and it can involve several aids, adaptations, and technologies, such as canes, walkers, glasses, hearing apparatuses, handrails, among others.
Studies used in a literature review showed the low use of hearing aidsby the elderly aged 80 years or older. They underline that hearing loss associated with ageing is a high prevalence phenomenon with the elderly population, which can cause a series of difficulties in oral communication, as well as very frequently interfere with family and social interaction23.
Edentulism is frequent among the older elderly, and in this study 83% of the long-lived reported to wear dentures and just 4% to have all teeth (Table 2). These results are similar to those found in a bibliographic review24, which revealed that most part of the older elderly have less than half of their teeth; quite a few of them wear dentures, and none was reported to have preserved all their teeth.
Studies show that feeble oral health is associated to malnutrition and, therefore, to higher risk of developing non-contagious diseases and worse quality of living13,25. One of those pieces of research25 demonstrated that the older the less frequent the use of odontologic services.
As for the dietarycharacteristics reported by the long-lived, most claimed to have healthy diets with fruit intake (68%), green vegetables (77%), milk and dairy (74%),white and red meat (62%), e 1%reported special diet on a gastronomic basis according to Table 3.
TABLE 3:
Dietary Intake by Older Elderly: Level Profile (%). Curitiba - PR, 2011. (N=100)
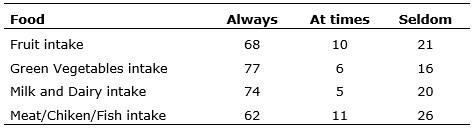
(*)One older elderly has a special gastronomic diet
One of the factors related to healthy ageing is good life-long nutrition. Adequate nutritional conditions increase chances for nearing maximum life cycle 13,26. In a quantitative study conducted with 14 long-lived elderly in Australia, participants found it essential to a good health condition to keep a balanced diet and reported a good diet is rich in fruit and green vegetables with reduction of meat27.This study revealed most long-lived elderly reported having a diet containing fruit, green vegetables, milk, and meat. However, as that is a self-report, dietary-related issues affecting the long-lived elderly can be better exploited in ethnographic studies.
CONCLUSION
Participants' profile in this study displays long-lived elderly who claim good living habits with low alcohol and smoking intake levels and a healthy diet. On the other hand, they are sedentary and lack activities that promote socialization and active ageing, as they do not participate in interaction groups and report television and house chores as their primary leisure means.
To nursing, socialization of the long-lived by means of interaction groups aims at developing the collective feeling of solidarity, anchored in the exchange of the care experience. Cooperation spirit developed along with more intense integration enhances enthusiasm about life and a drive for further and better self-care.
It can be inferred that sheer healthy habits claimed by the long-lived do not suffice to avoid incidence and aggravation of diseases, since they have at least one chronic disease, with emphasis on systemic blood hypertension and osteomuscular conditions. Still, polypharmacyhas frequent bearing in the results of national research with that age group and it provides warning to professionals regarding the benefits of medication.
In the present study, a few long-lived claimed not to have diseases, despite making use of medication. That unveils the need for attentive regard by the nursing professionalabout the several dimensions in care guidance. It is as central to focus professional attention on clinic problems as it is to account for cultural issues prompting actions developed in face of the long-lived family belonging, as the habit of self-medication.
One of the ways to bring down shortcomings among the long-lived is to facilitate their access to each and every proper apparatus and technology. Many of the elderly did not make use of them on account of difficulties in acquisition, among which slowness and high cost stand out. Likewise, edentulism cannot be accepted as a normal and natural phenomenon in ageing, but instead as a result of lack of preventive health policies forthe adult populationfor dental preservation up to advanced age.
Limitations to this study derive from the scarce scientific production on the long-lived age group as well as from the limited sample, which made inference over a few variables more difficult to make. Other quantitative studies with meaningful samples can develop the findings further and research which use qualitative approach can shed light onto subjective issues involving health and disease of the long-lived elderly.
REFERENCES
1.Veras R. Envelhecimento populacional contemporâneo: demandas, desafios e inovações. Rev Saude Publica. 2009;43:548-54.
2.Ministério da Saúde (Br). Secretaria de Atenção à Saúde, Departamento de Atenção Básica. Envelhecimento e saúde da pessoa idosa. Brasília (DF): Editora MS; 2010.
3.Instituto Brasileiro de Geografia e Estatística .Censo Demográfico 2010. Características da População e dos Domicílios: Resultados do Universo [site de internet]. Brasil(DF): IBGE; 2010. [citado em 08 mai 2015]. Disponível em: http://www.ibge.gov.br/estadosat/temas.php?sigla=pr&tema=resultuniverso_censo2010
4.Ministério da Saúde (Br). Tecnologia da informação a serviço do SUS – DATASUS. Projeções intercensitárias [site de internet]. Brasilia(DF): DATASUS; 2012. [citado em08 mai 2015]. Disponível em: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?ibge/cnv/poppr.def
5.Francisco CM. Estudo dos fatores preditores de envelhecimento sem incapacidade funcional entre idosos em velhice avançada no município de São Paulo [dissertação de mestrado]. São Paulo: Universidade de São Paulo; 2006.
6.Rosset I, Pedrazzi EC, Roriz-Cruz M, Morais EP, Rodrigues RAP. Tendências dos estudos com idosos mais velhos na comunidade: uma revisão sistemática (inter) nacional. Rev esc enferm USP. 2011;45:264-71
7.Menezes TM, Lopes RLM. Produção do conhecimento sobre idoso longevo: 1998-2008. Revenferm UERJ. 2009;17:569-74.
8.Marafon LP, Cruz IBM, Schwanke CHA, Moriguchi EHM. Preditores cardiovasculares da mortalidade em idosos longevos. Cad SaúdePública. 2003;19:799-807.
9.Bertolucci PH, Brucki SM, Campacci SR, Juliano Y. The Mini-Mental State Examination in a general population: impact of educational status. Arq Neuro-Psiquiatr. 1994;52:1-7.
10.Instituto Brasileirode Geografia e Estatística (Br). Censo demográfico 2000. Questionário da Amostra CD 1.02.[sitede internet]. Brasil(DF): IBGE; 2000. [citadoem 10 nov 2010]. Disponível em: http://www.ibge.gov.br/home/estatistica/populacao/censo2000/migracao/censo2000_migracao.pdf
11.Conselho Nacional de Saúde (Br). Resolução nº 196, de 10 de outubro de 1996. Aprova as Diretrizes e Normas Regulamentadoras de Pesquisas envolvendo Seres Humanos. [site de internet]. Brasília: Ministério da Saúde, 1996. [citado em 10 nov 2014]. Disponível em: http://dtr2004.saude.gov.br/susdeaz/legislacao/arquivo/Resolucao_196_de_10_10_1996.pdf
12.Nogueira SL, Ribeiro RCL, Rosado LEFPL, Franceschini SCC, Ribeiro AQ, Pereira ET. Fatores determinantes da capacidade funcional em idosos longevos. Rev Bras Fisioter. 2010;14:322-9.
13.Organização Mundialda Saúde. Envelhecimento ativo: uma política de saúde. Brasília (DF): Organização Pan Americana de Saúde; 2005.
14.Honório GJS, Martins HEL, Basso JF, Alvarez AM, Meirelles BS, Santos SMA. Estratégias de promoção da saúde dos idosos no Brasil: um estudo bibliométrico. Rev enferm UERJ. 2013;21:121-6.
15.Soares MBO, Tavares DMS, Dias FA, Diniz MA, Machado ARM. Características sociodemográficas, econômicas e de saúde de idosas octogenárias. Cienc Cuid Saúde. 2009;8:452-9.
16.Borges PLC, Bretas RP, Azevedo SF, Barbosa JMM. Perfil dos idosos frequentadores de grupos de convivência em Belo Horizonte, Minas Gerais, Brasil. Cad Saúde Pública. 2008; 24(12):2798-808.
17.Peregrino AAF, Schutz V, Marta CB, Pereira ACA, Silva GP, Nogueira LC. Buscando a inserção dos idosos nas ações de promoção social e de saúde. Rev enferm UERJ. 2012; 20:513-8.
18.European Union. Active ageing and solidarity between generations : a statistical portrait of the European Union 2012. Bélgica: Eurostat; 2011.
19.Borim FSA, Barros MBA, Neri AL. Autoavaliação da saúde em idosos: pesquisa de base populacional no município de Campinas, São Paulo, Brasil. Cad Saúde Pública. 2012;28:769-80.
20.Ferreira JVC. Os muito idosos no município de São Paulo [dissertação de mestrado]. São Paulo: Universidade de São Paulo; 2006. 1001p.
21.Ribeiro AQ, Rozenfeld S, Klein CH, Cesar CC, Acurcio FA. Inquérito sobre uso de medicamentos por idosos aposentados, Belo Horizonte, MG. Rev Saude Publica. 2008;42:24-32.
22.Morais EP. Envelhecimento no meio rural: condições de vida, saúde e apoio dos idosos mais velhos de Encruzilhada do Sul - RS [tese de doutorado]. Ribeirão Preto (SP): Universidade de São Paulo; 2007.
23.Veras RP, Mattos LC. Audiologia do envelhecimento: revisão da literatura e perspectivas atuais. Rev Bras Otorrinolaringol. 2007;73:128-34.
24.Ferrari MAC. Idosos muito idosos: reflexões e tendências. O Mundo da Saúde. 2002;26:467-71.
25.Matos DL, Giatti L, Lima-Costa MF. Fatores sociodemográficos associadosao uso de serviços odontológicos entre idosos brasileiros: umestudobaseadona Pesquisa Nacional por Amostra de Domicílios. Cad Saúde Pública. 2004;20:1290-7.
26.Campos MAG, Predoso ERP, Lamounier JA, Calosimo EA, Abrantes MM. Estado Nutricional e fatores associados em idosos. RevAssocMed Bras. 2006;52:214-21.
27.Orb A. Aspectos de salud em adultos mayores de 80 anos de edad que vivenindependientementeenlacomunidad: uma perspectiva australiana. Rev Latino-Am Enfermagem. 2004;12:589-96.