RESEARCH ARTICLES
Hospital emergency service patient reception with triage: evaluation of the care process
José Ap. Bellucci JúniorI; Dagmar Willamowius VituriII; Gelena Lucinéia Gomes da Silva VersaIII; Priscila Satie FuruyaIV; Rafhaela Calinca VidorV; Laura Misue MatsudaIV
INurse. Master degree in Nursing. Professor of the State University of Paraná North. Nursing Sector. Bandeirantes, Paraná, Brazil. E-mail: bellucci@uenp.edu.br
IINurse. Master degree in Nursing. Manager Nurse of Hospital Risks of the North Paraná Regional Univeristy Hospital, State University of Londrina.
Londrina, Paraná, Brazil. E-mail: dagmar@uel.br
IIINurse. Master degree in Nursing. Adult Intensive Care Unit- University HospitalUniversitário West Paraná. Cascavel, Paraná, Brazil. E-mail: gelenaenfermagem@yahoo.com.br
IVNurse. Master degree student in Nursing. State University of Maringá. Nursing Department. Maringá, Paraná, Brazil. E-mail: priscila.satiefuruya@gmail.com
VNurse. Santa Rita Hospital of Maringá. Nursing Sector. Maringá, Paraná, Brazil. E-mail: rafhaela_calinca@hotmail.com
VINurse. Ph.D. in Nursing. Professor from the Nursing Department of the State University of Maringá. Nursing Department. Maringá, Paraná, Brazil. E-mail: lmmatsuda@uem.br
DOI: http://dx.doi.org/10.12957/reuerj.2015.4976
ABSTRACT
This quantitative, cross-sectional study, conducted from August to November 2011, evaluated the care process in hospital emergency services that have introduced the Guidelines for Patient Reception with Triage. The sample comprised 314 employees in four emergency services, who had worked there for at least three months. Data were collected using the Patient Reception with Triage Evaluation Questionnaire. It was found that 75.5% of employees rated the care process as weak; 11.8%, as satisfactory; 9.5%, as inadequate, and 3.2%, as good. It was concluded that the services studied need to be reorganized in order to meet the requirements of the Guidelines for Patient Reception with Triage, and thereby improve their care processes. Keywords: Emergency hospital service; user embracement; triage; nursing.
INTRODUCTION
In the health area, the introduction of new technologies, the expansion of the complexity of services and the increasing demand of users for quality of care, have contributed to the evaluation of managers and scholars1.
In general, to evaluate is to give value judgment to a research object2. In health care, the evaluation is defined as the measurement of results obtained from care provided, and should reflect the quality of the structure and care processes3. Therefore, the evaluation is considered an indispensable component because, besides being part of the action planning and management4, it can identify factors that interfere in assistance.
In hospital emergency services (HES), especially in the implementation of new programs/guidelines/technologies, the evaluation of care processes are important5 because they are procedures performed and subsidize the decision making by managers3.
Nowadays in HES, there are many factors involved in the quality of care and are considered as difficult to resolve, such as: overcrowding; fragmented care; conflicts and power asymmetries; exclusion of users at the front door, among others6. These factors are significant barriers for quality because they require high investments, huge efforts of managers and employees, and especially users´ effort to understand the processes that involve health care environment.
Trying to improve the quality of care in HES, the Ministry of Health implemented in 2004, the guideline Embracement with Rating Risk (ACCR) as one of the key instruments to change the care process to users.
That guideline suggests to the user being welcomed and assisted based on predefined risk evaluation criteria that through the Nursing Consultation will allow the classification of each case of aggravation of potential in a color system that means: Red = Emergency; Yellow = Urgency; Green = Less Urgency; Blue = Not Urgency6,7. With the application of Rating Risk, the ACCR, seeks to ensure the users´ humanization of care, accessibility and the most welcoming and less exclusive service.
In Brazil, recent studies reveal that although few HES have implemented the ACCR guideline, it seems to be an effective strategy to managing quality in these services, since positive results in the process of care have already been observed8,9.
Considering HES is interconnected with all sectors of the hospital and that the ACCR is one of the main guidelines to promote quality of care in that place, this study is justified because: there are few publications on the implementation and evaluation of ACCR care process in Brazil and also by the importance of the results that may subsidize actions of managers, focused on its implementation and monitoring in health institutions.
Based on the above, it is asked: Considering the implementation of ACCR guideline in HES, what is the evaluation of employees about the process of care? To answer the question, this study aims to evaluate the process of care in hospital emergency services that have implemented the Embracement with Rating Risk guideline.
LITERATURE REVIEW
In 2004, the Ministry of Health proposed the National Care Humanization Policy and SUS Management (HumanizaSUS), which consists of a ministerial policy that proposes to humanization as a guideline of care and management practices at all levels of the Unified Health System (SUS)10.
In order to provide specific guidelines related to the HES management and quality, in 2004 and 2009, the Ministry of Health implemented the Embracement with evaluation and Rating Risk: an ethical-aesthetic paradigm into healthcare, and Embracement with Rating and Evaluation Risk6 , which had as the main objective to present the reception as an interference strategy in health work processes7.
The importance of the content in the cited documents, is certainly similar with the need to reorganize Brazilian HES, since through the sections above, it is possible to notice that besides emphasizing the importance of the user in the health system, it provides guidance on the process of care organization from the ACCR implementation.
METHODOLOGY
This is a cross-sectional study with quantitative approach, developed from August to November 2011, in four HES, named: HES I; HES II; HES III and HES IV.
HES I is part of a teaching hospital located in the Northwest of Paraná State, which started its activities on 20 January 1989 and implemented the ACCR in December 2010. It currently assists about 47,000 patients/year; it has an area with 31 beds, but accommodates about 90 patients/day; it is a reference in high complexity trauma care; it provides medical assistance and backup service in the main specialties (cardiology, neurology, surgery, orthopedics, among others).
HES II is also part of a teaching hospital located in northern region of Paraná State, which started its activities in 1971 and implemented the ACCR in 2007. By 2007, it assisted about 50,000 users/year. However, due to physical structure reform occurred in 2008 and 2009, it began to assist on average 40,000 patients/year. Currently it has 50 beds, it is a reference in the State to meet the highly complex patients, it is part of the State System of Urgency and Emergency Care Hospital as type III.
The HES III is in a philanthropic hospital in the southern region of São Paulo, which started its activities in 1947 and implemented the ACCR in 2007. Currently it assists about 100,000 patients/year, it has 12 rooms for service; 25 actual beds; and it is a reference in trauma care to 27 cities.
HES IV is part of a public hospital, located in the same city of HES I, it began operations in 2003 and implemented the ACCR in April 2008. It assists an average of 5,400 patients/year, it has 20 effective beds, two rooms observation and ten for procedures, medications, stocks, among others. It works 24 hours a day with reference to the Basic Health Units (UBS) in the city.
The sample consisted of 314 subjects and it was defined through stratified random sampling, proportional allocation, collected from August to November 2011. HES professionals were selected and stratified by professional category, with composition of at least 60% in each category. Having in hand the list of selected names and, upon refusal to participate or when the subject was not found in three attempts, the subsequent name was selected, and so on, until the end of the list.
The inclusion criteria were considered: professionals working directly in HES (nursing, medicine, reception, security, hospital care and social assistance); operating time in HES equal or less than three months and formal acceptance to participate in the study.
Data collection was performed in the workplace, using a self-administered questionnaire, called theEmbracement Assessment Tool with Risk Rating1, which in this study, the questions eight to 14will be analyzed, for the assessment of Care Process dimension, as: Security transmitted by the team to the user (question eight); Non-emergency calls in ACCR (question nine); Knowledge of ACCR protocol by the staff (question ten); Relationship of managers with the staff (question 11); Assistance flowchart clarity for the staff (question 12); Health team training to work in the ACCR (question 13) and; Reassessment of cases waiting for care (question 14).
For data treatment, the spreadsheets of Microsoft Excel for Windows 7.0 was used. Then there was the inferential statistical analysis, applying the EpiInfo 3.5.3 program. In this process, the average of the items was calculated and then, the results were compared with Classification for Dimensions Scores of the Instrument Evaluation1 being: 31.5 to 35.0 = great; 26.2 to 31.4 = satisfactory; 17.5 to 26.1 = precarious and; 7.0 to 17.4 = insufficient. The non-emergency calls item in the ACCR, which was presented in a negative way, it was positive in the data processing phase and those who were marked as Without Opinion or were in white, were computed with the value three (neutral).
As for the ethical aspects, the project of this study was approved by the Permanent Committee on Ethics in Research Involving Human Beings (COPEP) from the State University of Maringa - PR, under Ordinance Number 325/2011.
RESULTS AND DISCUSSION
Among the 314 participants, 114 (36.3%) were male and 200 (63.7%) were female. Regarding the professional category, 28 (8.9%) were Nurses; 150 (47.8%) were Auxiliaries and/or Nursing Technicians; five (1.6%) were Social Assistants; 59 (18.8%) were Doctors; 31 (9.8%) were Administrative Agents; 30 (9.6%) were Operating Agents and; 11 (3.5%) were Security Agents. The acting areas of professionals who answered to the evaluation instrument were: 277 (93.3%) Care; three (1.0%) Education; 15 (5.1%) Care and Education; one (0.3%) Care and Research and one (0.3%) Care, Education and Research.
Regarding their age, participants were from 22 to 67 years old (average of 40.5 ± 10.5 years old) and the operating time at the institution was three months to 35 years (average of 8.6 ± 8.4 years). The average in the operating time in HES was 7.2 ± 7.6 years.
The demographic characteristics data are the reality of Brazilian nursing, where there is a predominance of female professionals and, because it is the emergency room, there is a preponderance of younger professionals11.
The predominance score of nursing category (56.7%), in the composition of the HES team, corresponds to the literature in general, which indicates that nursing plays a fundamental role in the care process of that service and, therefore, it is the larger staff in the health institutions.
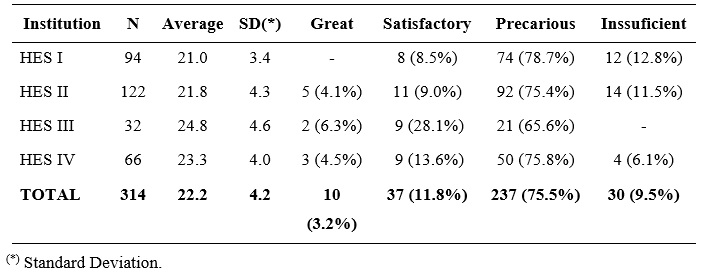
Data from professionals´ evaluation about the Case Process in ACCR are listed in Table 1.
TABLE 1:
Care Process Evaluation in HES. Maringá – PR, 2012.
It is observed that, regardless of the time of implementation of ACCR guideline, all four evaluated HES mostly classified the process of care as precarious. This is worrisome data because the result of the evaluation of the care process shows how the actions of giving and receiving care occurs, reflecting the care provided by health professionals and the way how users search and use the service12. To minimize the problem detected, it is suggested to carry out frequent and ongoing evaluations in order to support future improvement actions with all employees.
It is noteworthy that the high average precarious evaluation (75.5%) among workers of the four HES may have been influenced by the increase demand from external causes, that together with the organizational difficulties (such as lack of qualitative and quantitative human resources; inadequate physical structure; poverty or lack of equipment and materials13, reference system fragility and counter-referral8) certainly harm the process of care in ACCR.
It is observed that the sum of the percentages of records agree and strongly agree (58.97% - item eight) on security transmitted by the team to the user, reflects that most workers agree that the team helps the user feeling secure. See Table 2.
This result possibly is because in the ACCR the user does not leave the service without receiving any type of care. In addition, with the qualified hearing performed, one of the pillars of this guideline, the closest approach between the user and the health team tends to be closer and effective14.
TABLE 2: Items evaluation of Care Process in ACCR, by HES workers. Maringá, PR 2012.
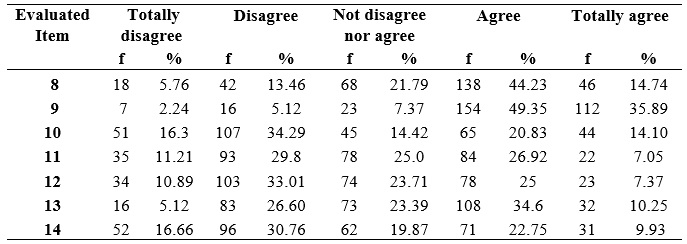
With regard to the Rating of the non-urgent cases, item nine, 85.24% of the participants indicated that they Agree that all patients go through ACCR. This means that even though the evaluation average of the four HES investigated were classified as precarious, the potential for worsening of the case is previously identified by the health team to all patients seeking the service. This finding goes together with patient´s safety, pointed out by workers since the health team approach, on the first contact of the patient with HES, is essential to allow the classification of those who need to be seen first and thus ensure that non-urgent cases can wait for safely care15.
Regarding knowledge of the ACCR's protocol by the team, item ten, more than half of participants (50.59%) disagreed that members of the health team of evaluated HES know the document. This is worrisome because the lack knowledge of some members of the multidisciplinary team, working in HES, about the ACCR´s protocol may involve the failure of its implementation, since decisions are taken through them. Among the decisions referred, there is the determination of care through color, ranking the priority of the case16.
Regarding the Interaction between managers and workers in the ACCR, item 11, 41.01% are disagree. This information shows that while the ACCR promotes reception and rapprochement in the health team, when it comes to acceptance by managers of suggestions for change in the way to operationalize the policy, there is still long way to go. A recent study shows the reception as a guideline that adopts a posture of responsibility for the actions of care and management, which is favored by the confidence and commitment among people who are part of HES care scenario17. In this sense, it is highlighted that the services investigated need more commitment from managers to discuss with the health team, the actions and proposals for improvements in the quality of ACCR.
Recognizing that the clarity of the ACCR care flowchart is of fundamental importance to remove problems in HES care, it is also worrying 43.9% of disagree in relation to the understanding of how to operate the flows in the ACCR (item 12). Currently, it has been observed that in HES seeking to discuss about the flowchart with the health care team, there are clear improvements in the quality of management and care8.
ACCR as an operational guideline should use clinical evaluation to stratify the assistance, based on the prioritization of the most serious cases. Nevertheless, it is necessary to remember that after the risk rating, the user must still wait for medical care in a specific location and must be reevaluated periodically by the nurse. In this sense, high percentage of answers showing the non-occurrence of the revaluation of the users who are waiting for medical care (item 14) were not expected to be found in this study (47.42%).
A study in HES II in 2011, demonstrated that the implementation of ACCR has improved the quality of care because, at the time the revaluation of users waiting for medical care were occurring among other changes18. On the other hand, data from this study indicate that the quality standard achieved at the time of that service guideline implementation was not maintained because, most of the workers of the institution said that the revaluation does not occur regularly. This fact justifies and emphasizes the need for continuing training for professionals involved in ACCR, as showing by the percentage of 44.85% regarding the Health Team Training to work in the ACCR (item 13).
CONCLUSION
Most of workers in this study evaluated the Care Process in ACCR as precarious. The factors that contribute to this result is mainly related to the lack of ACCR´s protocol by all members of the healthcare team of HES; to difficulties in understanding flows in ACCR and; the non-occurrence of revaluation of users who are waiting for medical care.
The results show that the ACCR care process, in the investigated services, needs further increase, especially in public education, with a major number of dissatisfied workers.
It is expected that the results of this research promote discussions and improvements, especially with the work of nurses in the care process in HES using ACCR, because he/she is the professional responsible for the user´s classification and revaluation in these services.
One limitation of this study is the fact that the instrument used is applied only for HES workers and thereby user´s evaluation was excluded. In this way, it is suggested to perform further research aimed at evaluation of the care process in HES using ACCR, from user´s perspective.
REFERENCES
1.Bellucci Júnior JA. Avaliação do acolhimento com classificação de risco em serviço hospitalar de emergência [dissertação de mestrado]. Maringá (PR): Universidade Estadual de Maringá; 2011.
2.Ferreira AS. Competências gerencias para unidades básicas do Sistema Único de Saúde. Ciênc saúde coletiva. 2004; 9: 69-76.
3.Donabedian A. Basic approaches to assessment: structure, process and outcome. In: Donabedian A. Explorations in quality assessment and monitoring. Ann Harbor: Health Administration Press. 1980; 1: 77-125.
4.Bosi MLM, Uchimura KY. Avaliação da qualidade ou avaliação qualitativa do cuidado em saúde? Rev Saude Publica. 2007; 41: 150-3.
5.Dubex LS, Freese E, Reis YAC. Avaliação dos serviços de urgência e emergência da rede hospitalar de referência no Nordeste brasileiro. Cad Saúde Pública. 2010; 26: 1508-18.
6.Ministério da Saúde (Br). Acolhimento e classificação de risco nos serviços de urgência. Brasília (DF): Editora MS; 2009.
7.Ministério da Saúde (Br). Secretaria Executiva Núcleo Técnico da Política Nacional de Humanização. HumanizaSUS - acolhimento com avaliação e classificação de risco: um paradigma ético-estético no fazer em saúde. Brasília (DF): Editora MS; 2004.
8.Bellucci Júnior JA, Matsuda LM. Implantação do acolhimento com classificação de risco e uso do fluxograma analisador. Texto contexto - enferm. 2012; 21: 217-25.
9.Bellucci Júnior JA, Matsuda LM. O enfermeiro no gerenciamento à qualidade em Serviço Hospitalar de Emergência: revisão integrativa da literatura. Rev Gaúcha Enferm. 2011; 32: 797-806.
10.Ministério da Saúde (Br). Política Nacional de Humanização da Atenção e Gestão em Saúde – HumanizaSUS. Brasília (DF): Ministério da Saúde; 2004.
11.Preto VA, Pedrao LJ. O estresse entre enfermeiros que atuam em unidade de terapia intensiva. Rev esc enferm USP. 2009; 43: 841-8.
12.Donabedian A. The Quality of Care - How Can it be Assessed? JAMA. 1988; 260: 1743-8.
13.Poll MA, Lunardi VL, Lunardi Filho WD. Atendimento em unidade de emergência: organização e implicações éticas. Acta Paul Enferm. 2008; 21: 509-14.
14.Nascimento ERP, Hilsendeger BR, Neth C, Belaver GM, Bertoncello KCG. Classificação de risco na emergência: avaliação da equipe de enfermagem. Rev enferm UERJ. 2011; 19: 84-8.
15.Albino RM, Grosseman S, Riggenbach V. Classificação de risco: uma necessidade inadiável em um serviço de emergência de qualidade. Arquivos Catarinenses de Medicina. 2007; 36: 70-5.
16.Souza RS, Bastos MAR. Acolhimento com classificação de risco: o processo vivenciado por profissional enfermeiro. Rev Min Enferm. 2008; 12: 581-6.
17.Dal Pai D, Lautert L. Sofrimento no trabalho de enfermagem: reflexos do "discurso vazio" no acolhimento com classificação de risco. Esc Anna Nery. 2011; 15:524-30
18.Rossaneis MA, Haddad MCL, Borsato FG, VannuchiI MO, Sentone ADD. Caracterização do atendimento após implantação do acolhimento, avaliação e classificação de risco em hospital público. Rev Eletr Enf. 2011; 13: 648-56.