RESEARCH ARTICLES
Access to health services: comparing the perspectives of professionals and users on primary care
Maria José Sanches MarinI; Maria Yvette Aguiar Dutra MoracvickII; Milton MarchioliIII
IPh.D. in Nursing and Professor of Nursing. Faculty of Medicine of Marilia. São Paulo. Brazil. E-mail: marnadia@terra.com.br
IIDermatologist and Professor of Medicine. Faculty of Medicine of Marilia. São Paulo. Brazil. E-mail: somebody@terra.com.br
IIIDoctor of Medicine. Professor of Education in Health Sciences. Faculty of Medicine of Marilia. São Paulo. Brazil. E-mail: miltonmachioli@unimedmarilia.com.br
IVPart of the study: “Comparação entre o atendimento das unidades básicas de saúde tradicionais e das unidades de saúde da família da cidade de Marília, na ótica dos usuários e profissionais” (Comparing the care provided at traditional basic health units and at family health units in the city of Marília, in the perspective of users and professionals).
DOI: http://dx.doi.org/10.12957/reuerj.2014.4238
ABSTRACT: The aim of this study was to compare health services accessibility from the perspective of professionals and users of the family health strategy (FHS) and traditional health basic units (THBU) in a municipality in the state of São Paulo. A total of 32 interviews were carried out and two questionnaires with 17 statements were applied, one of them being answered by 396 users and the other by 289 professionals, in 2011 and 2012. In the quantitative analysis, both professionals and users provided answers following a positive tendency, except for the period of operation of the unit and the waiting time for medical consultation. In the qualitative analysis, professionals and users’ opinions were close in the majority of aspects, but they mainly diverged on primary care as the system entrance and on the need for counter-referral. Therefore, changes are needed in the conception of health care.
Keywords: Health services accessibility; Health Services; Primary Health Care; Health Personnel.
INTRODUCTION
On the proposition of the current Brazilian Unified Health System (SUS, as per its acronym in Portuguese), a broad concept of health was defined. This concept considers the different determinants and conditions of the health / disease process, stating that health care should follow the principles of access universality, comprehensive care, equity, decentralization, hierarchy and social participation, with emphasis on primary care.
In terms of the constitutional principles that guarantee the right of all citizens to health care in accordance with the principles and guidelines of the SUS, access to health services is a comprehensive reference landmark for the study of their progresses and difficulties, which may be considered the first step in the pursuit of meeting the health needs of the population.
In the light of these principles and considering the need to check the progresses and challenges of this access, the objective of this study was to compare aspects of the access to health services in the view of users and professionals who work in the Family Health Strategy (FHS) and in traditional basic health units (TBHU).
LITERATURE REVIEW
Health services accessibility has been the target of different interpretations. Its broader concept, however, involves availability, accessibility, acceptability and financial capacity2.
In the study of primary care, some of the main quality indicators include the access, the system entrance, the list of services and the coordination or integration among these3. Access is understood as the location of the unit, which must be close to the population it assists, the hours and days it is open for service, the degree of tolerance for non-scheduled medical consultations, and how the populations is aware of this convenience. The system entrance refers to use of the primary care service as the first service through which people seek health care, with exception for emergencies. The list of services indicates the adjustments made by the unit so that the user can receive the care needed. The coordination or integration of services refers to the ease in accessing other levels of care and following up service in other specialized services. Such aspects are related to the users’ possibility of having their health care needs met at the desired moment, being aware that the healthcare system is hierarchically organized and that, although the system entrance can solve a great part of their health problems, it does not have appropriate technologies to meet care comprehensiveness.
Access comprehends four dimensions of analysis: the economic dimension, which refers to the relationship between supply and demand for health services; the technique dimension, which expresses the planning and organization of the network of services to provide the user with the expected treatment; the political dimension, being the capacity to develop sanitary awareness and social organization; and the symbolic dimension, referring to the social representations regarding the care and the health system organization to meet the users’ needs4.
According to the authors, in order to work the health services accessibility, it is necessary to encompass the greatest possible quantity and quality of variables related.
In this perspective, the access to health services includes elements that are considered to be essential to change the reality and to meet civil rights5, in addition to representing a great progress, since health care has been historically neglected by public policies, especially for low-income people.
Universal access to all health technologies, as a vested right, requires systematic monitoring aiming at its qualification, although its meaning is broad and involves the conception and demand from people and from the community to the services.
It is believed that through experiments and assessment it is possible to advance on the use of health care, especially among the less favored population2.
Following this direction, a national study evidenced the presence of access inequalities in different regions, as well as an internal heterogeneity, mainly manifested in relation to income and age6.7. There are also organizational barriers in the units that stand out, reflected by the profile of the professionals who work there8.
METHODOLOGY
The present study compares the service provided by the FHS and TBHU, from the perspective of professionals and users in a municipality in the interior of the state of São Paulo. Qualitative and quantitative approaches were used in the perspective of complementarity. The city is located in the Midwest region of the state of São Paulo, and it has an approximate population of 220,000 inhabitants. The primary healthcare system has 12 TBHU and 30 family health units (FHU). These FHU provide care to approximately 50% of the city population. Four TBHU and 12 FHU were randomly selected for the development of this study included, namely one TBHU and three FHU from each area of the city (North, South, East and West).
Data were collected from December 2011 to February 2012, based on access conditions, system entrance, list of services and the integration among these services. Qualitative data were collected by means of interviews with semi-structured questions. The criteria for selecting respondents included, among system users, adults of different ages, with severe and non-severe health conditions; and among professionals, areas of graduation were contemplated. Thus, 32 interviews were performed, namely eight with users and eight with professionals from the TBHU; eight with users and eight with professionals from the FHS. All interviews were fully recorded and transcribed.
The analysis of these qualitative data was based on dialectical-hermeneutics, whose interpretation parameters include: comprehensive analysis of the context in which data are generated and creation of analytical structures to seek ideas hidden in the texts9. Broader senses are used, moving forward to a synthesis movement, through the construction of possible meanings.
Quantitative data were collected using two instruments, namely one for the users and a second one for professionals. Each instrument had 17 statements. The Likert scale was used to obtain the opinion of the participants, based on the criterion of frequency (1. Never; 2. Hardly; 3. Sometimes; 4. Often; 5. Almost always; 6. Always), in which users and health professionals specify their level of agreement with each statement.
The population sample for obtaining quantitative data was established based on the simple random sample calculation, which allows the representativeness of the population, with an approximate possibility of sampling error of 5%. Hence, a sample of 400 users was obtained by using the formula ![]() , wherein za/2 = 1.95. (corresponding to 95% of the standard normal distribution), p=0.5 and e=0.05. Of these, 396 agreed to participate in this study. A sample of 150 subjects from the BHU and 164 from the FHS was obtained by means of the sampling calculation of health professionals, since 240 and 280 professionals work in these units, respectively. A total of 289 professionals complied with the study.
, wherein za/2 = 1.95. (corresponding to 95% of the standard normal distribution), p=0.5 and e=0.05. Of these, 396 agreed to participate in this study. A sample of 150 subjects from the BHU and 164 from the FHS was obtained by means of the sampling calculation of health professionals, since 240 and 280 professionals work in these units, respectively. A total of 289 professionals complied with the study.
The application of the instruments was performed by people who had been properly trained by researchers. The questionnaire of the professionals was self-administered, once the appropriate instructions for filling it out had been given. Users who were able to read and understand the content answered the users’ questionnaire without the help of the person responsible for the collection, and for those who did not have such condition, the form was read to them, and they were asked to provide the answers.
Quantitative data were typed into Excel 2000 for Windows spreadsheets, and statistical analyses were then performed using the software Statistical Package for Social Sciences (SPSS version 11.0 for Windows).
Inferential analyses were employed with the aim to verify the association of the assessment between FHS and TBHU users, and the assessment of the professionals from both units was performed using Wilcoxon test11. In all conclusions obtained by the inferential analyses, the significance level of α was set at 5% (p ≤ 0.005).
The research proposal was approved by the Municipal Health Department and by the Human Research Ethics Committee of the Faculty of Medicine of Marilia, under protocol no. 682/08. All subjects who agreed to participate in the study signed a Free and Informed Consent Form (FICF). In order to guarantee the anonymity of the participants, users were identified by the letter "U", and professionals by the letter "P", followed by a number from 1 to 8, according to the sequence of the interviews, and where it took place (TBHU or FHS).
RESULTS AND DISCUSSION
Regarding socio demographic characteristics, 95.2% of the professionals who participated in the study were female; 32% were community health agents; 22.6% were nursing aides or technicians; 9.3% were nurses; 5.3% were physicians, among others. As for the time working in the institution, there was a mean of 10.9 years for TBHU professionals and 6.1 years for FHS professionals. In the case of users, age ranged from 18 to 83 years, with a mean of 44.2 years, being 71.7% female, as presented in Table 1.
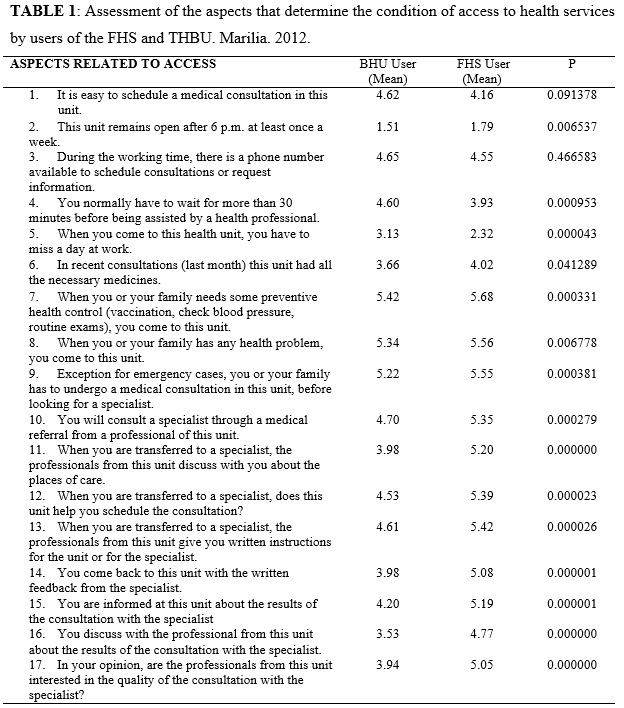
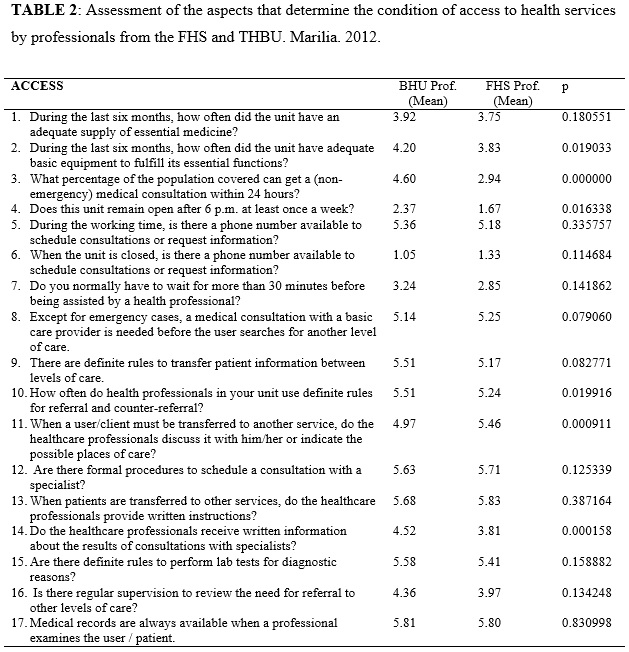
It is possible to note that, from the perspective of both types of care, the FHS had a more favorable mean in all statements. Regarding items four and five, it is important to mention that the answer that best qualifies the condition evidenced had a low score. The comparison of the answers of the professionals from the FHS and the TBHU about accessibility to health services showed significant statistical differences in six statements, considering that professionals from TBHU are prone to a more positive assessment of the analyzed aspects, with exception for item 11, according to Table 2.
In the qualitative analysis, while considering factors related to the health services accessibility from the perspective of users and professionals from the FHS and the TBHU, it was possible to identify three cores of meaning, as follows.
Adequacies and inadequacies of access
In the perspective of the study participants, the unit location is not a problem for any of the types of care. Concerning the availability of time for medical care, users point to the frequent lack of professionals and to the need to arrive very early at the unit so they can get an appointment, besides the waiting time until the consultation.
Look, you have to schedule the consultation […] Then it takes a few months, but when we are not feeling good, they do something […] at least for me, they do. (U2. FHS)
You wake up at 5 in the morning to get an appointment. Then they postpone it to the afternoon, and you are not assisted, you know? Always later, they never have time availability. (U4. TBHU)
In the speech of the FHS user, it is important to consider and highlight the delay of months until the consultation. It is possible that, having to wait for so long after the need is felt, alternatives are found to solve the problem. The delay in care, besides the low resolution was also pointed in a study with FHS users in the capital city of the state of Mato Grosso12.
It is considered that the demand for care occurs when one believes that some intervention can correct a situation considered abnormal, a situation that is absolutely subjective and dependent on factors such as the installation of a specific health problem, the offer of health care and the expectations of the user toward the health services13.
On the other hand, even aware of the users’ complaints, professionals believe that these needs may be met through other mechanisms, such as embracement and guidance, as described below.
Well, users sometimes complain. It is not always possible to please everyone, but all of them are well received and instructed. (P7. FHS).
A study on the perspective of FHS users showed that geographic location, bonding and embracement represent a fortress, even if, on the other hand, a reductionist point of view centered in the medical consultation and in curative actions prevails15. In the healthcare network of a Brazilian capital, access barriers were found even in primary care, but especially in other levels of care16.
It is known that the challenges to be overcome go beyond the aspects of financing, workforce and the models of management and care. There is also the need for health service offer in the right proportions, articulation among the different levels of services aiming at complementarity, and a new health care logic, by means of changes in the relationships between workers and user, especially with enhanced listening14.
Even though the implementation of the FHS expanded the range of services and brought professional and users closer, its characteristics also caused an increase in demand. An analysis on what causes this demand showed several reasons, including “the need felt, psychosocial factors, social security, demographics, epidemiology, use of service, regulation and cultural factors’’13:127. The authors consider that such factors overlap, resulting in an increasing demand that is hard to control.
System entrance from several views
The basic health unit, as the entrance to the healthcare system, represents a condition that makes access bureaucratic to users, whereas professionals understand that the organization is appropriate. Based on this discrepancy, it is possible to perceive that professionals are endowed of an objective logic of inclusion/exclusion to meet the demand, which does not always satisfy users, who think their needs are unique and deserve priority.
In the studied municipality, a risk classification is used to meet the demand, based on essentially objective criteria that do not always coincide with the need felt by the user.
[...] it is quite difficult because sometimes there are no doctors available. We have to look for an emergency unit at night, because you need a medical referral, and it is bureaucratic. (U3. TBHU)
We have to go to other units, then we get lost, not knowing where to go. To Santa Casa or to Hospital das Clínicas. Where do we have to go in emergency cases when there is no doctor available? (U8. FHS)
We come here to be referred somewhere else later. If you don’t come here, you don’t get an appointment. But there, if you arrive in the afternoon, close to 5 p.m., anyone can get an appointment. (U1. FHS)
The speeches of the users show that, after feeling lost with the lack of operation of the system entrance, they change organizational arrangements and find alternatives to have their needs met. In the light of this, the normal flow is changed, leading to the maintenance of care overload in the healthcare levels of a greater complexity.
In the current organization of the health system, primary care constitutes the priority system entrance and this action to reorganize the model brings rationality to its operation. This is based on the need for more adequate health resources, considering that many of the problems can be solved by means of light technologies and that the settings of greater complexity must be optimized to meet specific demands.
In a theoretical review on health services accessibility, advances and setbacks were also identified, confirming that although the access to basic health services has expanded, difficulties concerning the embracement and health care fragmentation still remain17.18. It also states that to ensure access to health care in public services, both interpersonal and socio-organizational relationships must be considered19.
It is possible to consider that professionals work in accordance with the rules and flows imposed in this rationality, not taking into account what is implicit in the needs of each user who demands care.
In general it is difficult, but we do our best to provide her with this possibility. (P5. TBHU)
All of those who arrive in the morning do not leave without being assisted. Only if there is no resource available, then people are referred to the hospital, but all of them are assisted. (P4. FHS)
Hence, the importance of the user’s active participation during the primary care process is emphasized, so as to transform it20.
Compromised service flows
The speech of both users and professionals show that the list of services is insufficient in face of their needs, especially with regard to specialized care. The provision of primary health care has been expanding for more than a decade through the implementation of FHS services. Although this aspect undoubtedly expands the possibility of access, it often limits the system entrance, since the services of greater complexity do not receive the same treatment. It is possible that without the outflow of this demand, the user will frequently return to the entrance and create a cycle of high demand and low resolution, which causes wear and tear to the professionals who daily face the population needs.
In addition, there is the belief of professionals and the population in the model centered in the disease and in complex technology, which limits the possibilities for progress in terms of health promotion and the use of light technology, based on enhanced listening, bonding and accountability as essential conditions to advance in meeting health needs. The following speeches state the difficulties of respondents as to the list of the health services to which they legally entitled, although they are not aware of it.
If I counted on the medicines from here, I would never be treated. So I buy the medicines by myself and have my medical exams made in private clinics. (U5. TBHU)
Medical referral... I waited for two years to get a neurology appointment for my daughter, two years. (U7. TBHU)
They performed a medical consultation to learn about my sickness [referring to the service] […] then I went there 15 days later to have the diagnosis. It worked fine. (U2. TBHU)
Associated with the difficulties found by users in relation to the list of services, there is the low integration among them. In the specialized service, although you need a referral containing the condition of the user to be assisted, the counter-referral is not usually provided by the service. It is the user himself who brings the information, which can affect the treatment continuation. A literature review study identified such aspects among the weaknesses related to primary health care21.
The difficulties in the integration among services are more observed by professionals, maybe because the user does not see its importance for the continuation and complementarity of the treatment.
Few services provide the counter-referral. We do not know if the patient really went there, the diagnosis, the behavior, the follow-up [...] It’s bad, especially concerning to the specialties. (P1. FHS)
Even with the difficulties related to service flows, the analysis of primary care in the coordination of the healthcare networks showed that the strengths overcome the weaknesses21. In terms of secondary care services, the need to improve the capacity of services is considered to improve planning tools and establish protocols, so that they can contribute to the network practices22.
It is noteworthy that the use of the methods of qualitative and quantitative research to analyze a phenomenon represents a complex activity, which is sometimes contradictory. However, this condition is handled in the perspective of complementarity.
CONCLUSION
The verification of accessibility evidenced that most of the aspects analyzed tend to have a positive evaluation, with users from the FHS showing greater satisfaction when compared to those of the TBHU. Regarding the professionals, those from the TBHU evaluate them as more positive.
Concerning to location of the health unit, both professional and users consider it appropriate to meet the existing needs. However, the delay to schedule medical consultations stands out, a fact which is more intense in the FHS when compared with the TBHU. In addition to this aspect, the restricted working hours of the units were also emphasized.
Users sometimes consider the primary care as system entrance to be a hindrance to the desired service.
Professionals understand that the service is appropriate to their needs, possibly because they operate guided by the objectivity of the risk classification system, whereas users seek health services by the immediate desire for medical care.
The list of services available is considered insufficient for all of the study participants, which is observed mainly by the delay of care, and often by the impossibility of having specialized care and specific exams. Regarding the integration among health services at different levels of care, it was noted that although users always reach the higher complexity services through a referral, counter-referral is not a common practice. This aspect is mainly recognized by professionals, since users do not consider this a clear need.
In conclusion, both the TBHU and the FHS have strengths and weaknesses that require new modes of organization and management, especially considering the subjective aspects involved in the needs of each user.
The limitation of this study involves the fact that it was conducted in only one city, which prevents generalizations, considering that each city has different ways of organizing the health care network. However, these results are expected to provide knowledge regarding the organization and operation of health services, as well as about their strengths and challenges.
REFERENCES
1.Lei 8.080. de 19 de setembro de 1990. Dispõe sobre as condições para a promoção. proteção e recuperação da saúde. a organização e o funcionamento dos serviços correspondentes e dá outras providências. Diário Oficial da União. Brasília (DF); 20 set 1990.
2.O’Donnell O. Access to health care in developing countries: breaking down demand side barriers. Cad Saúde Pública. 2007; 23: 2820-34.
3.Starfield B. Atenção primária: equilíbrio entre necessidades de saúde. serviços e tecnologia. Brasília (DF): Ministério da Saúde; 2002.
4.Giovanella L. Fleury S. Universalidade da atenção à saúde: acesso como categoria de análise. In: Eibenschutz C. organizador. Política de saúde: o público e o privado. Rio de Janeiro: Fiocruz; 1996. p. 177-98.
5.Jesus WLA. Assis MMA. Revisão sistemática sobre o conceito de acesso nos serviços de saúde: contribuições do planejamento. Cienc Saúde Coletiva. 2010; 15: 161-70.
6.Pessoto UC. Heimann LS. Boaretto RC. Castro IEN. Kayano J. Ibanhes LC. et al. Desigualdades no acesso e utilização dos serviços de saúde na região metropolitana de São Paulo. Cienc Saúde Coletiva. 2007; 12: 351-62.
7.Travassos C. Viacava F. Acesso e uso de serviços de saúde em idosos residentes em áreas rurais. Brasil. 1998 e 2003. Cad Saúde Pública. 2007; 23: 2490-502.
8.Cunha ABO. Vieira-da-Silva LM. Acessibilidade aos serviços de saúde em um município do Estado da Bahia. Brasil. em gestão plena do sistema. Cad Saúde Pública. 2010; 26: 725-37.
9.Minayo MCS. O desafio do conhecimento: pesquisa qualitativa em saúde. 12ª ed. São Paulo: Hucitec; 2010.
10.Barbetta PA. Estatística aplicada às ciências sociais. 3ª ed. Florianópolis (SC): UFSC; 1999.
11.Oliveira EFT. Grácio MCC. Análise a respeito do tamanho de amostras aleatórias simples: uma aplicação na área de ciência da informação. DataGramaZero [Internet] 2005 jun [citado em 20 jan 2014]. 6(3). Disponível em: http://www.dgz.org.br/ago05/Art_01.htm
12.Corrêa ACP. Ferreira F. Cruz GSP. Pedrosa ICF. Acesso a serviços de saúde: olhar de usuários de uma unidade de saúde da família. Rev Gaúcha Enferm. 2011; 32: 451-7.
13.Zucchi P. Del Nero C. Malik AM. Gastos em saúde: os fatores que agem na demanda e na oferta dos serviços de saúde. Saude Soc. 2000; 9: 127-50.
14.Ministério da Saúde (Br). Acolhimento à demanda espontânea. Brasília (DF): Ministério da Saúde; 2011.
15.Nery AA. Carvalho CGR. Santos FPA. Rodrigues VP. Saúde da Família: visão dos usuários. Rev Enferm UERJ. 2011; 19: 397-402.
16.Souza FOS; Medeiros KR. Gurgel Junior GD. Albuquerque PC. Do normativo à realidade do Sistema Único de Saúde: revelando barreiras de acesso na rede de cuidados assistenciais. Cienc Saúde Coletiva [Scielo-Scientific Electronic Library Online] 2014 [citado 20 set 2014]. 19:1283-93. Disponível em: http://www.scielo.br/pdf/csc/v19n4/1413-8123-csc-19-04-01283.pdf
17.Assis MMA. Jesus WLA. Acesso aos serviços de saúde: abordagens. conceitos. políticas e modelo de análise. Cienc Saúde Coletiva. 2012; 17: 2865-75.
18.Macedo CA. Teixeira ER. Daher DV. Possibilidades e limites do acolhimento na percepção de usuários. Rev enferm UERJ [Internet] 2011 [citado em 20 set 2014]. 19: 457-62. Disponível em: http://www.facenf.uerj.br/v19n3/v19n3a20.pdf
19.Barbosa SP. Elizeu TS. Penna CMM. Òtica dos profissionais de saúde sobre o acesso à atenção primária à saúde. Cienc Saúde Coletiva [Scielo-Scientific Electronic Library Online] 2013 [citado 20 set 2014]. 18:2347-57. Disponível em: http://www.scielosp.org/scielo.php?script=sci_arttext&pid=S1413-81232013001600019
20.Clares JWB. Silva LMS. Dourado HHM. Lima LL. Regulaçao do acesso ao cuidado na atenção primária: percepção dos usuários. Rev Enferm UERJ. 2011; 19: 604-9.
21.Rodrigues LBB. Silva PCS. Peruhype RC. Palha PF. Popolin MP. Crispim JA. et al. A atenção primária à saúde na coordenação das redes de atenção: uma revisão integrativa. Cienc Saúde Coletiva [Scielo-Scientific Electronic Library Online] 2014 [citado em 20 set 2014]. 19:343-52. Disponível em: http://www.scielo.br/pdf/csc/v19n2/1413-8123-csc-19-02-00343.pdf
22.Erdmann AL. Andrade SR. Mello ALSF. Drago LC. A atenção secundária em saúde: melhores práticas na rede de serviços. Rev Latinoam Enferm [Scielo-Scientific Electronic Library Online] 2013 [citado em 20 set 2014]. 21(esp):131-9. Disponível em: http://www.scielo.br/pdf/rlae/v21nspe/pt_17.pdf