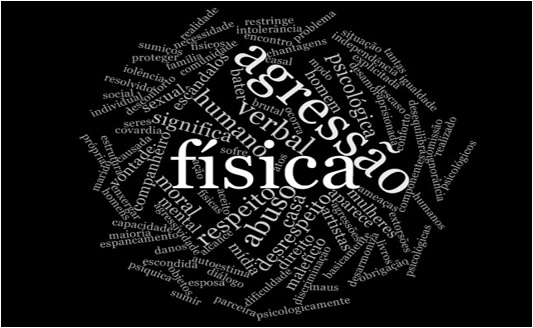
Figure 1: Word cloud formed by nursing professionals about DVAW. Rio Grande, RS, Brazil, 2013.
ORIGINAL RESEARCH
Assimilating the theory and practice of domestic violence: nursing professionals providing primary care for victims
Cristiane Lopes AmarijoI; Edison Luiz Devos BarlemII; Daniele Ferreira AcostaIII; Sérgio Correa MarquesIV
I
Ph.D. student in Nursing from Federal University of Rio Grande. Rio Grande
do Sul, Brazil. E-mail:
cristianeamarijo@yahoo.com.br
II
Ph.D. in Nursing. Professor at the Federal University of Rio Grande. Rio
Grande do Sul, Brazil. E-mail: ebarlem@gmail.com
III
Ph.D. in Nursing. Professor at the Federal University of Rio Grande. Rio
Grande do Sul, Brazil. E-mail: nieleacosta@gmail.com
IV
Ph.D. in Nursing. Professor at the Federal University of Rio de Janeiro.
Brazil. E-mail: sergiocmarques@uol.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2018.33874
ABSTRACT
Objective: to examine how nursing professionals in a family health unit assimilate the theory and practice of domestic violence against women (DVAW). Method: in this qualitative study, based on Social Representations Theory, data were collected from 25 nursing professionals by semi-structured interview, entered into Nvivo 10 software and treated by content analysis. Results: two analytical categories were elaborated: the components of DVAW (concept, image and attitude); and detection of cases of DVAW. Conclusion: the structured representation (containing image, concept and attitude) reveals the influence of the professional context. It is believed that articulating victim protection and care services in a network would render primary care for women more effective, decisive and comprehensive.
Descriptors: Domestic violence; violence against women; family health; nursing.
INTRODUCTION
Domestic violence against the women (DVAW) is a global, old and current phenomenon, with important cultural relevance and social thickness. Usually, they are shown in the media, and they are cases that arouse the attention of the civilian population. Some of them express a feeling of revulsion, while others seek a justification for the fact. They are beliefs, practices, values, judgments present in society, even shared among health professionals1.
DVAW is considered to be practiced in the space of permanent conviviality of people, regardless of family ties. VDCM causes a loss of nine million of healthy years of life annually in the face of physical, psychic and sexual disorders to the victims, which defines it as a serious public health problem2.
Young women are the main victims who may experience this form of violence for years without seeking help. Fear of the aggressor, usually the intimate partner, financial dependence, embarrassment of being judged by the neighbors and threat of death to themselves or their children are among the factors that inhibit the search for legal, social or family protection.
When professionals search for health services, especially those directed to primary care3,4 to address chronic or acute problems resulting from violent acts, not all cases are identified. This is because health care still has a strong influence on biomedical practice, inhibiting the understanding of the needs of women victims.
In this context, the family health units (FHU) reinforcing the integral care are at a privileged level for the detection of risk situations, identification of possible victims and aggressors, health promotion and prevention of injuries to patients and the community5. The multidisciplinary team that acts in this scenario has the responsibility to strengthen light technology such as bonding, listening and welcoming, conditioning factors for a health care model that addresses social problems with health impact, such as DVAW.
Professionals who work directly in the care of victims need to understand the phenomenon beyond the conceptual aspect, overcoming barriers that hinder a more effective action. It is necessary to know the support network to guide women and guide them to services, together with an approach that values the complaints and marks of the soul, not only the visible marks caused by the physical injuries, qualifying the care in its affective/expressive dimension6. Such care needs to be exempt from judgments, negative criticism or even blame of the woman. Considering that the practices are governed by social representations and that this conceptual assimilation influences the practices and that DVAW is a phenomenon present in the professional context of nursing that works in primary care, the question is: what is the theoretical and practical assimilation of nursing professionals about DVAW? The purpose of this study was to analyze the theoretical and practical assimilation of domestic violence against women among nursing professionals, considering the care provided to the victims in the family health unit.
THEORETICAL REFERENCE
It is considered unequal to problematize the conceptual and practical assimilation about VDCM among professionals involved in care. These elements constitute the Social Representation (SR) about the phenomenon defined as "a modality of knowledge generated through communication in everyday life, with the practical purpose of guiding behaviors in concrete social situations"7:68. It determines the behavior considered acceptable, tolerable and lawful, under the influence of the social context of individuals. It designates a "particular mode of knowledge" with the function of "the elaboration of behaviors and the communication between individuals"8:27.
SRs are always the representation of something (object) for someone (subject)8. The conceptions of the individual about the context, in which he is inserted, when verbalized, express the SR that he has about the world around him, and can influence his behavior, because "representation contributes exclusively to the processes of formation of the behavior and orientation of social communications"8:71.
The components of a SR are structured in three dimensions: concept/information, attitude/judgment, and image/representation field. The concept consists of information, the knowledge that a certain group has about an object. The attitude constitutes the opinion, the judgment one has about the object8. Opinion "is, on one hand, a socially valued formula to which a subject adheres and, on the other hand, a position on a controversial [discussed] problem of society"8:43. It is the most frequent of the three dimensions since people only represent after they have been positioned in front of the object and in function of this position taken8. The image or mental sensations represents the impressions that people or objects leave in our brain. "The image is conceived as an internal reflection of the external reality, a copy according to the thought of outside. Thus, it is a passive reproduction of the immediate given [...]"8:44. These dimensions allow the knowledge of the content and the meaning of representation8.
METHODOLOGY
This is a descriptive, exploratory social research with a qualitative approach, developed in 19 FHU in the city of Rio Grande/RS/Brazil, divided into rural and urban areas to contemplate various sociocultural contexts of the municipality.
All the nurses and nursing technicians of the units were invited to participate in the study. Those who were on leave or health leave were excluded. The data were collected from July to November of 2013, through a semi-structured interview. They were questioned about the knowledge, experiences, practices and personal and professional perceptions about DVAW.
The interviews were recorded with the consent of the informants, transcribed and inserted in the NVivo Software version 10 and submitted to the content analysis proposed by Bardin9. NVivo is qualitative analysis software that allows creating categories, encode, search, and explore the material. It was developed to facilitate the organization, analysis, and sharing of data, regardless of the method used10.
Initially, the sources that is, the interviews were explored and encoded innodes, which constitute information storage structures. The nodes contain fragments of the sources that later, the analytical categories will emerge. The codification of the nodes can provide the researcher with the hierarchical organization of the nodes11, forming trees of nodes according to need and creativity. This structure resembles categories and subcategories or classes and subclasses.
The theme was chosen as the unit of record. "To make a thematic analysis consists in discovering the nuclei of meaning of communication and whose presence or frequency of appearance can mean something[...]" 9:135.
Regarding the presentation of the results, the software enables the use of a variety of resources such as the word cloud, obtained from the word frequency tool that allows generating a list of the most frequent terms in the interviews. In this cloud, there is a direct relationship between the size of the word design and its frequency of verbalization.
Aiming for anonymity, the statements were identified by N (Nursing) and NT (Nursing Technician) followed by the number corresponding to the interview plus the abbreviation UZ for urban area and RZ for rural zone. The project was approved by the Research Ethics Committee of the Federal University of Rio Grande, opinion number 010/2013.
RESULTS AND DISCUSSION
There were 13 nurses and 12 nursing technicians participating in the interviews. Six of the N and six of the NT worked in the urban zone; the others in the rural zone. Only two informants were male, ranging from 30 to 57 years old, predominantly from 40 to 49 years old. Nine N and eight NT participated in courses, lectures or seminars related to the theme. As for the marital status, six were single, two had stable partner and 17 resided with a partner. Six NT and 12 N completed the vocational training course before 2003, the others did it after that year.
The components of DVAW: concept, image, and attitude
Most often naturalized by common sense, DVAW is part of daily life of health professionals. However, cases diagnosed and valued socially are those that have physical marks12, causing other forms of violence to remain veiled before the non-disclosure of women.
In the word cloud (Figure 1), the terms most frequently mentioned by the participants appear highlighted, confirmed by the participants' speeches. See Figure 1.
Figure 1:
Word cloud formed by nursing professionals about DVAW. Rio Grande, RS,
Brazil, 2013.
The salience of the terms physical, aggression, abuse and verbal are highlighted. These words are permeated by respect, home, disrespect, moral, psychological, among others. These words reveal the recognition of forms of violence and judgment about the object.
Referring to the aggressive acts, the greatest was the physical term. Other expressions of violence such as verbal, moral and psychological have also been reported. The psychological form impacts on health with the same intensity and is usually associated with physical and sexual violence 13. The words, disqualifying phrases, used with the intention of contempt,14 the threats of death cause inertia in the woman and social isolation making her more vulnerable to the violent cycle. The following speeches clearly expose the graphic representation of the word cloud.
Domestic violence against women means a violation of women's rights... There is physical violence, but there are other types of violence to which they submit. (N5-UZ)
For me, domestic violence against women ranges from verbal aggression to physical violence. Violence is in many ways. It may even be in the look. (NT6-UZ)
A study carried out with 150 nurses from Lisbon, which aimed to identify SR of violence against women, revealed that when faced with the stimulus When I think of violence, I remember... the six words mentioned most frequently were: aggression, pain, physical aggression, psychological aggression, ill-treatment, and injuries. For them, physical aggression comes to the forefront of the injuries presented15.
Considering that SR is formed by three dimensions: representational field/image, concept/information, and attitude/judgment, physical marks characterize the image of the object, something visible in the body of the woman thus allowing the identification of the phenomenon. The image represents the mental impressions that people or objects leave in the brain before the induction to the theme, and is conceived as an internal reflection of the external reality8, as illustrated by the following speech:
When you think of DVAW, the first thing you think is physical aggression, but I think domestic violence is not restricted to the physical violence... I think physical violence happens a lot because it is the one that people who see more, who listen on the radio, see on TV, in the newspaper, who goes to the media, which appears with the artists, which ends up generating the scandals. (N144-RZ)
The concept consists in the information, in the knowledge that certain group has about the object, being represented by the different forms of violence reported. The attitude constitutes the opinion, the judgment on the phenomenon listed by the terms abuse and disrespect. Both, present in the cloud of words may indicate that for these professionals, violence constitutes a disrespect that occurs in the victim's home, or the couple, a place that should be a protection, becomes insecure because the aggressor is inside the home.
Domestic violence against women means a disregard, a lack of respect for the woman at home... (N103-RZ).
Domestic violence against the woman is an aggression, an abuse of the companion to his own wife. (NT75-UZ)
The view of a partner husband, caretaker, protector of woman and children is misrepresented by the figure of a perverse, aggressive man who injures his companion through violence and brutality. Statistics point to the intimate partner as the aggressor in most DVAW cases. Between 2007 and 2012, the Women's Care Center, also known as Ligue 180 had 257,562 reports of domestic violence, of which most of them were intimate partners16.
Based on female subalternity, many men adopt violence as a way of correcting behavior they consider incorrect. The right of women to make choices is understood as an erroneous behavior that should be penalized.
DVAW case detection
The cloud of this category allows inferring that the practices experienced by the professionals contribute to the construction of their SR on the theme and vice versa17. This cloud brings patient evidence followed by conversation. Through it, the nurse develops the reception and the consultation in the healthunit. As forms of diagnosis of the violence, the presence of bruises, the injured, scared and fear patient were mentioned. The terms house, companion, and aggression evidence the scene of the violent act as well as its causative agent. See it in Figure 2.
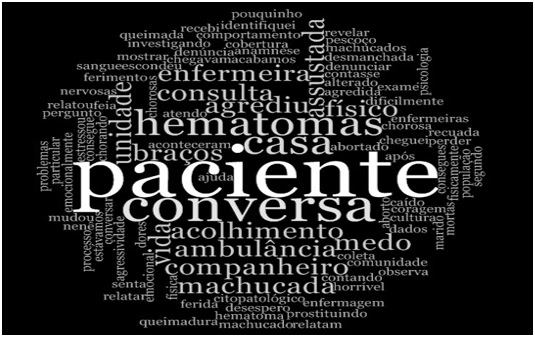
Figure 2:
Word cloud formed by nursing professionals about VDAW. Rio Grande, RS,
Brazil, 2013.
These terms can reveal how professionals visualize the victims and the actions that make up the care. When the patient searches for the service, the conversation is one of the main resources for detecting victimization. During the reception, the victims should be guided about their rights and the resources they can use in the fight against violence, such as self-help groups, care by members of the multi-professional team18 or problematization about the life project. In this sense, the terms reveal that informants give global care to clients involving biological, psychological and social aspects.
I identified the case in a nursing consultation [...]. We have been talking, we have been talking, and they are telling us their lives. (N167-UZ)
The patient came to us asking for help because she had been beaten by her companion... the patient was able to speak exactly how things happened, how she even came to physical violence. (N166-UZ)
The expression managed to speak exactly as things happened illustrates that in this case, there was facility in communicating the occurrence; there is often difficult for victims to report the experience. Generally, when the woman searches for the service and does not reveal or even does not present apparent physical injuries, violence is masked by non-specific symptoms3 hindering to identify the case.
It was a horror! When we arrived at the place, I had an abortion at home. The scene was pretty ugly. She had aborted and the baby had a way of being all formed, had the way to have about 8 to 9 months of gestation. At the time she said she felt pain, began to squeeze and evacuated. She had blood, she had feces, it was a movie scene, horrible! And she had aborted. And we sent her and the fetus to the hospital... Then, investigating, I know that it was violence, she had been beaten by her partner. (N144-RZ)
I got a husband and wife who were arguing. She was making food and he, I do not know why threw a pan of hot oil in her. [...] The woman arrived badly, she came all burned, all dismantled from the burn. (N103-RZ)
It is observed that the chronification of violence is a problem to be faced in health units. In addition, the repetitive cycle hinders cases by making primary care a place where the professionals need to be prepared to overcome everyday challenges in impacting and disabling situations like DVAW.
Due to the complexity of the DVAW, and also to the effective care of victims, a holistic and multi-professional view of the phenomenon is required. As observed in this study, the different ways of being-acting have positive repercussions on care. The heterogeneity of the group, the individual strategies of care, the subjective view of the nurse and the established bond lead to a mutual reflection, encouragement, and elaboration of a life project bringing the light expected by the women victims, as shown below.
I do not even need the patient to talk. You see by the state, sometimes physical, emotional that it is... (NT6-UZ)
I started to talk to her, I put the gauze where she was bruised. I put the gauze to draw the blood. I was talking and saying that everything would calm down, it would get better. I went softening to see if she would stop crying. A comfort with the words to see if she was less anxious, because she was very emotional, crying. I try to do my best that is reassuring, doing the dressing, giving affection in that hour that she is needing, understanding. (NT8-UZ)
During the conversation with the woman, the matter arose and the agent called the responsible nurse who began to solve the problem. (NT145-RZ)
In this way, the care in the FHU is permeated by the affective dimension, which consists in the valorization of the other. Affection can be expressed by demonstrations of empathy or even subtle gestures such as a touch, tone of voice or a smile. Caring with affectivity requires interest and commitment to the patient4, present among nursing professionals in this study.
Before the SR on DVAW, the role of the nurse in caring for the woman victim emerges, as presented in the word cloud. In FHU, the community agents and nursing technicians use this professional category to give resolubility to cases. Also, there is the knowledge that the unit nurse, as coordinator, has a prominent position in the integration among the team, in the elaboration of training activities, among others.
DVAW is not justified, however, there are factors considered precursors. At the same time, the can act as motivators or inhibitors of denunciation. Some inhibitors are lack of economic conditions to live without the partner, concern for children and fear of being killed. As motivators, there are desire to end the situation experienced, desire to have peace and return to life and plans to study, work, and relate to friends and family, wear clothes of their choice, as noted below.
The patient arrived at the unit for help because she had been beaten by her partner. After the data collection, the patient was able to tell exactly how things happened, how she even came to physical violence. He talked about the behavior of the partner at home, of having been always violent. She talked about all this time that they are together until she has the courage to go to the unit [...] In a second moment, that patient has already changed the speech a little, that old question that she has no way to stay out of it. He spoke of the fear of denunciation, of not having to do with children, of losing the children. (N166-UZ)
The high frequency of women in health services is also due to their social role as caregiver for their children and their husbands. In these opportunities, the nursing consultation constitutes an adequate resource for the detection of cases of violence4. However, for the care provided to be transformative, it is necessary for the nurse to consider the experiences, valuing the professional-patient relationship19 .
When providing care, nursing needs to look beyond the fact or the complaint presented, think about the macrosomic factors that can trigger violence and direct their care actions to the person considering their specificities and singularities.20:176
However, studies of health professionals' representations about health DVAW revealed that fear can act as an influential factor of professional activity21,22.
CONCLUSION
DVAW is a reality in FHU and nursing professionals are usually the first to provide care to victims. For nursing professionals working at FHU in the city of Rio Grande/RS, the SR of violence has a concept, image, and attitude. The strong salience of the imagery dimension is highlighted, illustrated by the frequency of the expression physical violence in the participants' speech, which can be fed by the visualizations of the marks left on the bodies of the victims.
It should be considered that the SR that these professionals have of the DVAW can influence their practices, both preventive and care, contributing positively or negatively to the detection and outcome of cases, as well as to ensure the rights of women.
It was found that different from the literature, the care provided by the professionals of this study was not restricted to the physical aspect. They are concerned with welcoming the victims, establishing a bond of trust based on dialogue, listening, and caring.
Difficult actions to confront and assist women in situations of violence will be decisive if they continue to be based on the model of biomedical attention.
It is believed that despite detecting the theoretical and practical assimilation about the DVAW observed by the nursing professionals in the care of the victims, in primary care, reality reinforces the need for multidisciplinary action with emphasis on the problematization of the phenomenon in different spaces, as community, schools, university context, companies, campaigns with the population to demystify their naturalization and promote gender equity.
It is recognized that the limitations of this study include a reduced sample and restricted to a Brazilian municipality, which prevents the generalization of the findings.
REFERENCES
1.Silva CD, Gomes VLO, Oliveira DC, Marques SC, Fonseca AD, Martins SR. Social representation of domestic violence against women among Nursing Technicians and Community Agents. Rev. Esc. Enferm. USP. (Impresso). 2015; 49(1): 22-9.
2.Senado Federal (Br). Lei nº 11.340, of August 7, 2006. Creating mechanisms to curb domestic and family violence against women. Brasília (DF): Gráfica Senado Federal; 2006.
3.Gonzáles GC, Bejarano CR. Gender violence: evolution, impact, and keys to its approach. Enfermería Global. 2014; 33:424-39.
4.Guedes RN, Fonseca RMGS, Egry EY. Limits and evaluation possibilities of the Family Health Strategy for gender violence. Rev. Esc. Enferm. USP. 2013; 47(2):304-11.
5.Hesler LZ, Costa MC da, Resta DG, Colomé ICS. Violence against women from the perspective of community health agents. Rev. gaúch. enferm. 2013; 34(1):180-6.
6.23.Gomes VLO, Silva AL, Ern E. The care of children in day care centers: a space for nursing. Rev. gaúch. enferm. 2003; 24(2):177-88.
7.Sá CP. The construction of the research object in social representations. In: The identification of phenomena of social representation. Rio de Janeiro: Editora UERJ; 1998.
8.Moscovici S. Psychoanalysis, its image, and its audience. Translated from English by Sofia Fuhrmann. Petrópolis(RJ): Editora Vozes; 2012.
9.Bardin L. Content analysis. São Paulo: Editions 70; 2011.
10.QSR International. Manual NVivo 10. Pty Ltd; 2014.
11.Grijó WP. Use of qualitative research software in data analysis of the
media reception. X POSCOM - Seminar of Postgraduate Students in Social
Communication of PUC-Rio November 04, 05 and 06 of 2013. [cited 2017 Jun 16]; Available from:
http://pucposcom-rj.com.br/wp-content/uploads/2013/11/Wesley-Pereira-Grijo%CC%81.pdf.
12.Acosta DF, Gomes VLO, Barlem ELD. Profile of police incidents of violence against women. Acta paul. enferm. 2013; 26(6):547-53.
13. Albuquerque JBC, César ESR, Silva VCL, Espínola LL, Azevedo EB, Ferreira Filha MO. Domestic violence: sociodemographic characteristics of women enrolled in a Family Health Unit. Rev. eletrônica enferm. [Internet]. 2013; [cited 2017 Jan 08]; 15(2):382-90. Available from: http://dx.doi.org/10.5216/ree.v15i2.18941.
14. Giraldo SLH, Ballén MNR. Female experiences and imaginaries that naturalize domestic violence. Index de enfermería. 2014; 23(1-2):26-30.
15. Leal SMC, Lopes MJM, Gaspar MFM. Social representations of violence against women in the nursing perspective. Interface - comunic. saude, educ. 2011; 15(37):409-24.
16. Senado Federal (Br). Joint Parliamentary Committee of Inquiry. To investigate the situation of violence against women in Brazil and to investigate allegations of omission by the public authorities regarding the application of instruments established by law to protect women in situations of violence. Final report. Brasília (DF): Gráfica Senado Federal; 2013.
17. SÁ CP. Central core of social representations. Petrópolis (RJ): Vozes; 2002.
18.Kind L, Orsini MLP, Nepomuceno V, Gonçalves L, Souza GA, Ferreira MFF. Underreporting and (in) visibility of violence against women in primary health care. Cad Saúde Pública (Online). 2013; 29(9):1805-15.
19. Souza MC, Mendes GFR, Lima SDLM, Santana JMAMP, Oliveira MBB, Silva JS. A Inter-American Convention to Prevent, Punish, and Eradicate Violence Against Women (the Convention of Belém do Pará) and Maria da Penha Law. Revista Âmbito Jurídico. Caderno Internacional. 2014. [cited 2017 Mar 03]; Available from: http://www.ambito-juridico.com.br/site/index.php?n_link=revista_artigos_leitura&artigo_id=7874#.
20. Batista JMS, Trigueiro TH, Lenard MH, Mazza VA, Labronici LM. The bioecological model: unveiling contributions to the nursing praxis for domestic violence. Esc. Anna Nery Rev. Enferm. 2013; 17(1):173-8.
21. Silva CD, Gomes VLO, Oliveira DC, Amarijo CL; Acosta DF, Mota MS. Representation of domestic violence against women among the health professionals: age as an attribute of differentiation. Rev. enferm. UERJ. 2016; 24(3):e13212.
22. Amarijo CL, Gomes VLO, Gomes AMT, Fonseca AD, Silva CD. Social representation of nursing professionals about domestic violence against women: a structural approach. Rev. enferm. UERJ. 2017; 25:e23648.