ORIGINAL RESEARCH
Job insecurity among obstetric nurses
Jane Márcia ProgiantiI; Noelle Juliana Melo de Paula MoreiraII; Juliana Amaral PrataIII; Manoel Luís Cardoso VieiraIV; Terezinha Andrade AlmeidaV; Octavio Muniz da Costa VargensVI
I
Nurse. PhD. Associate Professor. Rio de Janeiro State University. Rio de
Janeiro, Brazil. E-mail: jmprogi@uol.com.br
II
Nurse. MS. Municipal Health Department of Rio de Janeiro. Rio de Janeiro,
Brazil. E-mail: moreiranoelle86@gmail.com
III
Nurse. PhD. Assistant Professor. Rio de Janeiro State University. Rio de
Janeiro, Brazil. E-mail: juaprata@gmail.com
IV
Nurse. Student of the doctorate course in nursing. Rio de Janeiro State
University. Rio de Janeiro, Brazil. E-mail: mlcv22@uol.com.br
V
Nurse. Student of the doctorate course in nursing. Rio de Janeiro State
University. Rio de Janeiro, Brazil. E-mail: uerjuesb@gmail.com
VI
Nurse. PhD. Full Professor. Rio de Janeiro State University. Rio de
Janeiro, Brazil. E-mail: omcvargens@uol.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2018.33846
ABSTRACT
Objective: to think about concrete working conditions identified in sociodemographic profiling of obstetric nurses working in Brazil's Unified Health System. Methodology: this quantitative, descriptive study was conducted with fifteen obstetric nurses in Rio de Janeiro, Brazil, in 2016. Data was collected by interview and subjected to statistical analysis. The study was approved by the research ethics committee. Results: taken together, the labor relations, wages, number of jobs, and working hours of obstetric nurses' working in the Brazilian Unified Health System pointed to increasing job insecurity in the public service. Conclusion: considering the advancing influence of capitalist rationale in Brazil's Unified Health System, obstetric nurses need to strengthen their class unity in order to develop strategies for coping with these conditions that are degrading their work process, which has great potential for harming their health and care for women.
Descriptors: Obstetric nursing; Women working; Health systems; Job market.
INTRODUCTION
In the 1990s, the neoliberalism conquered the Brazilian scenario with proposals for reforms involving the containment of the social expenses, the privatization of public assets, the deregulation of the market and the globalization of the economy.1
At the same time, flexible management and work organization models were introduced in the labor field, demarcating the beginning of the productive restructuring that presupposes innovations in the productive processes in order to reduce costs, increase competitiveness and improve efficiency. 2
This political, economic and labor reconfiguration has determined the reduction of the State's role in the social areas, having important impacts on the financing of the Unified Health System (SUS - "Sistema Único de Saúde", in Portuguese language) and, consequently, on the health work process.
On the one hand, there were flexible models for managing human resources and services, culminating in the expansion of the care network, through partnerships with non-profit organizations and Social Organizations (SO), and in the advent of different forms of labor contracts in the public sphere. On the other hand, health policies emphasized the need to rethink the care provision from the perspective of the comprehensiveness and autonomy of individuals, valuing the focus on the living work, the one that materializes in the act of interaction between professional and user, and on the use of light technologies, based on relational processes, to the detriment of the dead work and the use of hard technologies, typical characteristics of the biomedical model, still predominant in the Brazilian health services.3
In this context, nursing, especially the obstetric nurse, has been standing out in the scope of care to women's health as strategic agents to change the logic of care, since the work process of these specialists presents itself focused on the living work and on the use of light technologies.
Thus, this study aimed to reflect on the objective conditions of work, identified in the socio-demographic profile of the obstetric nurses who work in the Unified Health System.
LITERATURE REVIEW
The way of producing care of the obstetrical nurses responds to the demands of the public policies by promoting a change in the health care model, improving the maternal and neonatal indicators, in addition to reducing the cesarean rates. In addition, the performance of these specialists in SUS is also economically interesting for neoliberal politics, because investing in a work process based on living work and light technologies represents a way to reduce costs.3
The recognition of these potentialities of the obstetric nurse is evident in the increase in the participation of these specialists in the labor and delivery care and in the expansion of jobs positions in the health care of women in the context of SUS, mainly from 2011, with the implementation of the "Cegonha" Network at the national level and the "Cegonha Carioca" Program, in the city of Rio de Janeiro.4-6
Despite the absorption of obstetrical nurses in the SUS labor market shows a growing trend in recent years, the existence of different types of labor relations, such as the statutory regime and hiring through the SO is observed, which can be interpreted as a weak contract, because it does not guarantee the same social benefits of the public servant and, therefore, assumes a configuration that is similar to the employment in the private sector.4
Such a multi-contract configuration reaffirms the flexibilization in the public sector, because the differences in the relationship between the statutory and the OS employees and the State characterize a fragmentation of the links with the public administration, referring to one of the faces of the precariousness of the work at SUS, regarding the difficulties of regulation regarding admission, dismissal and performance of the workers. 2,7
Beyond this dimension, the precariousness can also be seen in the instability of labor relations, which may present weaknesses in social protection rights or in the conditions of work that put workers in a situation of vulnerability, in the sense of insecurity, intensification and demotivation.1,7
Due to the general deregulation of the working conditions in Brazil, the obstetric nursing is in a delicate position, in which the precariousness can affect more deeply because it is a female labor process.
METHODOLOGY
This text constitutes a quantitative cut of a broader research, 8 of the descriptive type, which sought to analyze the effects of the nurses' working conditions in the obstetric field.
The study participants were 15 obstetric nurses from the city of Rio de Janeiro, who concluded their postgraduate studies at the end of 2011, year of the implementation of governmental initiatives that increased the jobs for obstetric nurses in SUS.
As inclusion criteria, it was adopted: to have at least six months of work experience in the obstetric area of the public sector and to have a contractual relationship as an obstetric nurse. As exclusion criteria, it was considered: to have less than six months of work experience in the obstetric area; work only in the private sector or to have a contract as a generalist nurse.
The data collection was carried out from April to May 2016, through a semi-structured interview, following a script divided into two sections. The first one, containing closed questions that seized, from the socio-demographic profile of the participants, the objective conditions of the obstetric nurses' work. The second, with open questions that captured the subjective conditions. The interviews were carried out of the work place of the participants and had an average duration of 45 minutes.
For the purpose of this text, only the objective conditions, defined as those related to the material production of the company and which are given in the material reality, such as the contract, the salary/income and the working day were considered.9 Thus, the quantitative data produced by the first part of the script were analyzed by simple descriptive statistics and presented as absolute frequency and percentage.
In compliance with Resolution 466/2012, the participants signed a Free and Informed Consent Term and their anonymity was preserved. The study was approved by the Ethics and Research Committee of the State University of Rio de Janeiro, under CAAE 54061315.9.0000.5282 and opinion no. 1.459.532.
RESULTS AND DISCUSSION
Regarding the objective dimension of the working conditions of the obstetric nurses interviewed, it was verified that ten (66.66%) participants accumulate two employment contracts, prevailing the employment relationship governed by the Consolidation of the Labor Laws (CLL), in the hiring modality established through the SO. Regarding salaries, eight (53.33%) had monthly income above R$ 6,000.00 and seven (46.66%) between R$ 3,500.00 and 6,000.00.
The data show that the eight nurses with a monthly income above R$ 6,000.00 have two employment contracts in the public sector. Of this group, six declared to have two CLL-type contracts and two said to associate a statutory contract with a CLL one.
Of the seven nurses with a monthly income between R$ 3,501.00 and R$ 6,000.00, five have only one contract, four were hired through the CLL and one statutory. The other two participants, who are also in this salary range, reported having two contracts, one accumulating two statutory contracts and the other accumulating a statutory and a CLL contracts.
As for the working days, most of the participants develop their professional activities in the obstetrical center. However, as a result of the accumulation of contracts, these activities include activities in the welcoming and risk classification (mentioned by 6 obstetric nurses) and/or prenatal care (scored by 2 obstetric nurses). Thus, by working in different occupational spaces, nine (60.00%) participants reported working for 60 hours a week, three (20.00%) for 30 hours, two (13.33%) for 40 hours and one (6,66%) for 50 hours.
As one of the effects of capitalism on the labor process, there is the separation between man and the means of production, with the consequent alienation of the worker about the objective conditions of their work, because the productivist model places the worker in a social position of subalternity to the capital, incurring in the loss of control over their material life.10 These conditions are expressed in the division of labor, in the possession of the means of production, in the conjuncture, in the objects and fields of intervention, in the occupational spaces, in the work relations, in the resources used by the workers, in the deregulation of contracts, in low salaries, in rotation and fragmentation of the work.9
Regarding the nature of the labor relations established between the participants and the public sphere, the prevalence of CLL-related contracts was found to be detrimental to the statutory regime. This finding stems from the productive restructuring under way in the Brazilian public health services, which have been adopting new formats for the management of the services and human resources, mainly through the SO, with the justification of improving the quality and efficiency of SUS.3
However, this speech of managerial innovation emerged in an adverse panorama of limitations in the investments for SUS that, added to the complexity of its bureaucratic structure and the restrictions imposed on the statutory regime, reinforced the representation of the administrative incapacity of the public machine and the need for the participation of the private initiative, with the consequent introduction of the market logic of the capital in the public services.11 To this end, legal provisions were created that allowed for changes in the form of hiring and structuring of the workforce, with emphasis on the Constitutional Amendment No. 19/1998, which reconfigured the SUS's labor field based on new modalities of contract for professionals, with the coexistence of statutory, contractual, temporary and outsourced health workers. 7,12
It should be highlighted that the adoption of flexible hiring practices in the Brazilian health field began in the midst of the decentralization and municipalization processes, gaining strength with new policies and local execution programs, such as:the Family Health Program, the Community Health Agents Program, the Mobile Emergency Care Service and, more recently, the "Cegonha" Network and the "Cegonha Carioca" Program.5
Under the aegis of flexibilization, precarious work contracts proliferated in SUS, defined as one that is exercised under conditions in which the worker is in a situation of risk, fragility and vulnerability.13 In this sense, the activities in the informal sector and the outsourced and temporary jobs in the formal sector are classic examples of precarious work because they form fragile bonds that do not ensure proper labor and social security rights. To these are added the forms of entrance into the public administration that are not by means of a public tender, which constitute irregularities by disobedience to the current norms of administrative law and work.14
Based on these considerations, it was verified that the thirteen obstetrical nurses who have at least one CLL contract, although they enjoy labor rights, are in the condition of precarious work for not complying with the rules of investiture in the public service, since they were hired through a selective process involving only titles evaluation.15
On the other hand, in the case of the five obstetrical nurses who are under the statutory regime, despite the stability of this type of contract, the precariousness lies in the working conditions. These indicative conditions of precariousness may be due to the absence of salary adjustments, the absence of a career plan, the growth of variable forms of remuneration among statutory workers and, above all, the relationship with other workers in the same category.11 In this context, with the incorporation of the capital logic in the SUS management, the meanings attributed to the work in the public sector are similar to those typical of the private sector.2,7
As an effect, it is evident the precariousness of the work at SUS, result of the multiplicity of labor realities and the difficulty of regulating them. The confrontation of this problem has been done with programs and strategic actions, especially the creation of the Department of Management and Regulation of Work in Health, the National Program for the Desprecarization of the Work at SUS and the Program for Qualification and Structuring of Labor Management and Education at SUS.14
Despite these efforts, some issues remain far from the discussion, such as the salary differences between statutory and CLL workers.12 In the case of the participants of this study, these inequalities, outlined by the nature of the labor relationship, add up to the differentiated remuneration among professionals who perform the same activity (normal birth care), which is limited between obstetric nurses and obstetricians.
Comparing the base wage offered in the last public tender for the provision of nurses in effective position in the Municipal Health Department of Rio de Janeiro, published in 2013, with the provisions of a call for a selection process for the hiring of obstetric nurses, performed in 2014 by a SO, it can be seen that, even with the annual adjustments, the SO offers a salary that is 108.14% higher than what is established for professionals under the statutory regime. This discrepancy is even higher when compared to the salaries of obstetricians hired by the SO, reaching a value that is 257.88% higher than that received by statutory obstetric nurses. 15-17
Faced with these distinctions, it is observed that health professionals are better paid when hired through SO. This fact corroborates the dissemination of negative representations about the work in the public sector that, by allowing differentiated conditions of remuneration among professionals who carry out the same activity, disaggregates the collective ideology of struggle among workers, creating more obstacles for the consolidation of SUS.7,10
In addition, by practicing unequal salaries among professionals of the same category and specialty, internal competitions emerge among obstetrical nurses who contribute to the degradation of the environment in the service. Thus, those who receive higher salaries enter the capitalist mode of production of the private sector, seeking productivity through often repetitive practices, focusing on technical aspects and optimizing their production time.18 Meanwhile, those who find themselves in a pay gap perceive the devaluation of their work process and feel discouraged.
This conformation among obstetrical nurses working in the public sector, with exacerbated salary differences and particularized labor relations, results in the fragmentation of the nursing workforce,12 weakening the power of mobilization of these workers to fight for recognition and appreciation of work in the specialty, which is precarious in comparison to the salaries offered to obstetricians.
In view of this, it is possible to affirm that the statutory nurses are submerged in a process of precarious work since, in the relation with obstetric nurses and doctors who have a common contract with the SO, they receive smaller salaries and, therefore, can be perceived as exploited and devalued in the obstetric field. In this aspect, it is evident one of the faces of the precariousness of the SUS work that reaches even the servants with stable contracts and high schooling.18
In addition, by offering higher salaries than those practiced under the statutory regime, the SO induces the CLL professionals to work harder to achieve production goals and justify the salaries received. In addition, it should be emphasized that the statutory nurses receive the same salary independent of the sector of activity and the nature of the activities developed, as well as there are no salary differences between the CLL professionals who work in the obstetric center and the ones allocated in the welcoming sector. This reality shows the devaluation of the scientific capital of obstetrical nurses due to the non-recognition of the specialist title, and the specificities of their work process in the delivery rooms.
With this, it is possible to identify the polyvalence of work, defined as the multiplication of the intellectual abilities and the capacities of the worker to perform different tasks, to perform and to occupy different roles and job positions.19 This demand for the multifunctionality of the obstetrical nurses in the labor process of delivery rooms reveals the flexibilization of these workers, a necessary instrument for the productive restructuring under way in the public sector.
There is also a contradiction between the programmatic discourse of SUS and its operationalization in the health services, as the investment in the insertion of obstetrical nurses in maternity delivery rooms is a recommendation of the public health policies for women in order to humanize and qualify the obstetric care.4,5 However, while recognizing the active role of these specialists to achieve these objectives, there is no concrete appreciation of them, because the established work contract disregards the amount of scientific capital required for their professional practice in delivery rooms, that is, the set of knowledge, skills, competences and attitudes of the specialty.
Despite the appreciation of the obstetrical nurses in the policies, the absorption of these specialists into the SUS labor market without due remuneration for their qualification and specialization show another aspect of precariousness, expressed by the social devaluation of the work that materializes in the salary discrepancy found among obstetricians and the participants of this study.
Such devaluation results from the sexual division of labor, as a form of social division of labor, modulated historically and socially from the conception of masculine work being destined to the productive sphere and the feminine work to the domestic reproductive sphere. From this perspective, gender inequalities are formed, with men performing works of greater visibility and hierarchically superior, while women, when they enter the productive public space, receive lower remunerations and suffer from the disqualification of their work, regardless of their level of schooling.20,21
Thus, the obstetric nurses, women of a female profession associated with human care, inserted in a specialty that requires relational skills related to nature and to the feminine, have their work process disqualified against the social status that the medical profession incorporates in a society marked by the male domination principle.21-23
As a result of these gender inequalities arising from the sexual division of the health work, it is common for nurses to have more than one job, having long working days in the productive world, in addition to unpaid activities developed in the private sphere.5,18 In this sense, nursing is recognized as the professions that is most prone to illness due to their intense working hours, especially when they work in hospitalization units.18,19
This is also the reality of the working conditions of the participants of this study, since most of them report having a monthly income higher than R$ 6,000.00 for accumulating two employment contracts, working 60 hours per week, much of it developed in the obstetrical center sector. This situation points to the labor intensification, defined by the increase in the degree of intensity of the work that is expressed in the prolongation of the working days, in the increase of the pace and speed of activities, in the accumulation of functions, in the demand for polyvalence and flexibility, in the search for productivity and variable remuneration. 18,19,23
In the last decades, this process has affected several professional categories in the public and private sectors, being common among health workers, especially nurses, because they are more involved in the direct care provision to the clientele and because the accumulation of jobs is frequent due to the low salaries. In this group, the intensification also results from the psychic attrition, the complexity and heterogeneity of the activities developed in the hospital environment, which are configured as overload by adding a greater volume of material and immaterial labor. 19,24
At first, work should be a source of satisfaction and professional achievement, however, in conditions of labor intensification, it can be a factor that generates stress, dissatisfaction and frustration, which compromises the functional and moral capacity of the workers, with important impacts on the quality of services.12,19,24
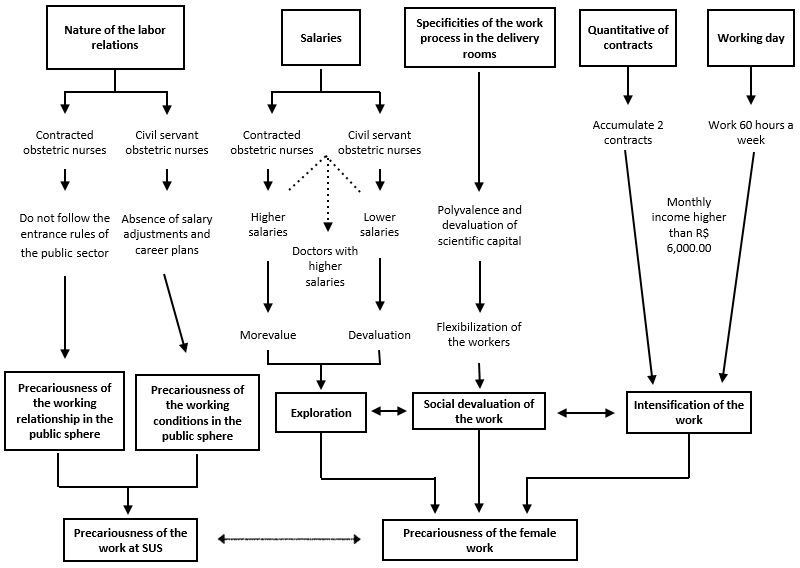
In this sense, it is observed that the obstetrical nurses working at SUS are more susceptible to the effects of intensification since many objective conditions of their work process point to precariousness, as shown in Figure 1:
Figure 1: The dimensions of the precariousness of the obstetric nurses' work from the objective conditions of their work process at SUS. Rio de Janeiro, Brazil, 2016.
CONCLUSION
As a result of the productive restructuring implemented in SUS, the obstetrical nurses maintain labor relations with the public administration through the statutory regime and, mainly, through the CLL regime mediated by the SO. Despite the formality of these contracts, they have precarious work conditions, because the CLL workers do not obey the rules of entrance in the public service and the statutory ones are directly affected by the budgetary restrictions of SUS.
The exacerbated salary differences found among workers performing the same activity revealed the sexual division of labor, because statutory nurses have lower salaries than those in a CLL regimen and obstetricians receive much higher salaries. Moreover, there is no recognition of the scientific capital of the obstetric nurses, since they are not remunerated for the exercise of their specialty, bringing the idea of flexibilization that refers to the social devaluation of their work process.
Thus, most of the participants have long working hours and accumulate two labor contracts in order to reach a monthly income closer to their demands. In this context, exploration, devaluation and intensification are characteristics incorporated into the work process of obstetric nurses, which evidence the precariousness of the female labor in the public sector.
In addition to the probable deleterious effects of this configuration on the life of obstetric nurses, the negative impacts of the fragmentation of this work force on the collective struggle of the specialty for social valuation and recognition must be considered. Also, in the long term, precariousness can trigger the leaving of these specialists from the delivery rooms, jeopardizing the effectiveness of the public health policies for women, which reinforce the importance of obstetrical nurses.
Thus, it is essential that these specialists strengthen their class unity in order to devise strategies to face the objective conditions that are deteriorating their work process, with potential to harm their own health and the care provision to women.
Nevertheless, it is important to reflect on the repercussions of the advance of the capitalist logic in the public service which, by producing derogatory representations about the work at SUS, creates more obstacles to its consolidation.
The study had as a limitation the reduced number of participants, due to the reduction of obstetric nurses working in maternity hospitals, cause and consequence of the precarious work conditions of these nurses.
REFERENCES
1.Massimo L. Como se explica o neoliberalismo no Brasil? Uma análise crítica dos artigos publicados na Revista Dados. Rev. Sociol. Polít. [periódico da internet]. 2013 [cited 2017 Aug 23]; 21(47):133-87. Available from: http://www.scielo.br/scielo.php?pid=S0104-44782013000300010&script=sci_abstract&tlng=pt
2.Marques APP. Reestruturação produtiva e recomposições do trabalho e emprego. Um périplo pelas "novas" formas de desigualdade social. Ciênc saúde coletiva. (Online). 2013 [cited 2017 Aug 23]; 18(6):1545-54. Available from: http://www.scielo.br/scielo.php?script=sci_abstract&pid=S1413-81232013000600007&lng=es&nrm=iso&tlng=pt
3.Prata JA, Progianti JM, David HSL. A reestruturação produtiva na área da saúde e da enfermagem obstétrica. Texto & contexto enferm. (Online). 2014 [cited 2017 Aug 23]; 4(23):1123-9. Available from: http://www.scielo.br/pdf/tce/v23n4/pt_0104-0707-tce-23-04-01123.pdf
4.Progianti JM, Prata JA, Barbosa PM. A reestruturação produtiva na saúde: os efeitos da flexibilização nas maternidades do Programa Cegonha Carioca. Rev. enferm. UERJ. (Online). 2015 [cited 2017 Aug 23]; 23(2):164-71. Available from: http://www.facenf.uerj.br/v23n2/v23n2a04.pdf
5.Pereira ALF, Nicácio MC. Formação e inserção profissional das egressas do curso de residência em enfermagem obstétrica. Rev. enferm. UERJ. (Online). 2014 [cited 2017 Aug 23]; 22(1):50-6. Available from: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/11418/8977
6.Leal MC, Pereira APE, Madeira MRS, Theme Filha MM, Dias MAB, Pereira MN et al. Intervenções obstétricas durante o trabalho de parto e parto em mulheres brasileiras de risco habitual. Cad. Saúde Pública. (Online). 2014 [cited 2017 Aug 23]; 30(suppl. 1):17-47. Available from: http://dx.doi.org/10.1590/0102-311X00151513
7.Martins MIC, Molinaro A. Reestruturação produtiva e seu impacto nas relações de trabalho nos serviços públicos de saúde no Brasil. Ciênc saúde coletiva. (Online). 2013 [cited 2017 Aug 23]; 18(6):1667-76. Available from: http://www.scielo.br/scielo.php?script=sci_abstract&pid=S1413-81232013000600018&lng=pt&nrm=iso&tlng=pt
8.Moreira NJMP. Precarização do trabalho no campo obstétrico: percepções de enfermeiras [dissertação]. Rio de Janeiro: Universidade do Estado do Rio de Janeiro; 2017.
9.Santos MT, Manfroi VM. Condições de trabalho das/os assistentes sociais: precarização ética e técnica do exercício profissional. Em Pauta. [periódico da internet]. 2015 [cited 2017 Aug 23]; 13(36):178-96. Available from: http://www.e-publicacoes.uerj.br/index.php/revistaempauta/article/view/21057/15716
10.Duck G. A terceirização na saúde pública:formas diversas de precarização do trabalho. Trab. Educ. Saúde. [periódico da internet]. 2016 [cited 2017 Aug 23];14 (suppl. 1):15-43. Available from: https://dx.doi.org/10.1590/1981-7746-sol00023
11.Ribeiro CVS, Mancebo DO. O servidor público no mundo do trabalho do século XXI. Psicol. Ciênc. Prof. [periódico da internet]. 2013 [cited 2017 Aug 23]; 33(1):192-207. Available from: http://www.scielo.br/scielo.phpscript=sci_arttext&pid=S1414-98932013000100015
12.Ribeiro AC, Souza JF, Silva JL. A precarização do trabalho no SUS na perspectiva da enfermagem hospitalar. Cogitare enferm. Rev. (Online). 2014 [cited 2017 Aug 23]; 19(3):569-75. Available from: http://revistas.ufpr.br/cogitare/article/view/33034/23247
13.Dedecca CS, Trovão CJBM. A força de trabalho no complexo da saúde: vantagens e desafios. Ciênc. saúde coletiva. (Online). 2013 [cited 2017 Aug 23]; 18(6):1555-67. Available from: http://www.scielo.br/scielo.php?pid=S1413-81232013000600008&script=sci_abstract&tlng=es
14.Ministério da Saúde (Br). Gestão do trabalho e da regulação profissional em saúde: agenda positiva do Departamento de Gestão e da Regulação do Trabalho em Saúde. 3ª ed. Brasília (DF): Ministério da Saúde; 2009.
15.Centro de estudos e pesquisa 28. Organização Social em Saúde. Edital nº 16 de 30 de dezembro de 2014. Dispõe sobre o Processo Seletivo de vagas e formação de cadastro reserva para Enfermeiros Obstetras HMMR – Cegonha Carioca. [Internet]. [cited 2017 Aug 23]. Available from: http://www.cep28.org.br/transparencia/processos-seletivos-2014/.
16.Rio de Janeiro. Secretaria Municipal de Saúde. Edital nº 144 de 3 de junho de 2013. Regulamenta o concurso público para provimento de cargos de nível superior, médio e fundamental completos, prioritariamente, no âmbito da secretaria municipal de saúde do município do Rio de Janeiro. [Internet]. [cited 2017 Aug 23] Available from: http://doweb.rio.rj.gov.br/visualizar_pdf.php?edi_id=2086&page=1
17.Centro de estudos e pesquisa 28. Organização Social em Saúde. Edital nº 01 de 05 de janeiro de 2016. Dispõe sobre o processo seletivo de vagas para médicos obstetras. [Internet]. [cited 2017 Aug 23] Available from: https://www.cep28.org.br/transparencia/edital-processo-seletivo-medico-obstetra/
18.Melo CMM, Carvalho CA, Silva LA, Leal JAL, Santos TA, Santos HS. Força de trabalho da enfermeira em serviços estaduais com gestão direta: Revelando a precarização. Esc. Anna Nery Rev. Enferm. (Online). 2016 [cited 2017 Aug 23]; 20(3):e20160067. Available from: http://www.scielo.br/scielo.php?pid=S1414-81452016000300211&script=sci_abstract&tlng=pt
19.Gonçalves FGA, Souza NVDO, Pires AS, Santos DM, D`Oliveira CAFB, Ribeiro LV. Modelo neoliberal e suas implicações para a saúde do trabalhador de Enfermagem. Rev. enferm. UERJ. (Online). 2014 [cited 2017 Aug 23]; 4(22):519-25. Available from: http://www.facenf.uerj.br/v22n4/v22n4a14.pdf
20.Pereira AV. O cotidiano de enfermeiras e enfermeiros: relações de gênero, a partir do tempo no hospital. Rev. latinoam. enferm. (Online). 2015 [cited 2017 Aug 23]; 23(5):945-53. Available from: http://www.scielo.br/pdf/rlae/v23n5/pt_0104-1169-rlae-23-05-00945.pdf
21.Mies M. Origens sociais da divisão sexual do trabalho. A busca pelas origens sob uma perspectiva feminista. Rev. Direito e Práx. [periódico da internet]. 2016 [cited 2017 Aug 23]; 7(15):838-73. Available from: http://www.redalyc.org/articulo.oa?id=350947688027
22.Bourdieu P. A dominação masculina. Tradução de Maria Helena Kuhner. 2ª ed. Rio de Janeiro: Bertrand Brasil; 2002.
23.Souza MMT, Passos JP, Tavares CMM. Sofrimento e precarização do trabalho em enfermagem. Rev. pesqui. cuid. fundam. (Online). 2015 [cited 2017 Aug 23]; 7(1):2072-82. Available from: http://www.seer.unirio.br/index.php/cuidadofundamental/article/view/1515/pdf_1456
24.Dodou HD, Sousa AAS, Barbosa EMG, Rodrigues DP. Sala de parto: condições de trabalho e humanização da assistência. Cad. Saúde Colet. (Online). 2017 [cited 2017 Aug 23]; 25(3):332-8. Available from: http://www.scielo.br/scielo.php?pid=S1414-462X2017000300332&script=sci_abstract&tlng=pt