Notes: CLASS: Classification; PERT: Pertinence. Subject 7 hospitalized for only four days, total 13 clients in T2.
ORIGINAL RESEARCH
Nursing care to comfort people with immunobullous dermatoses: evaluation by fuzzy logic
Euzeli da Silva BrandãoI, Iraci dos SantosII, Regina Serrão LanzillottiIII
I
Nurse. PhD. Adjunct Professor, Federal Fluminense University. Niterói, Rio
de Janeiro, Brazil. E-mail: euzelibrandao@gmail.com
II
Nurse. PhD. Full Professor, University of the State of Rio de Janeiro.
Brazil. E-mail: iraci.s@terra.com.br
III
Statistian. PhD. Adjunct Professor, University of the State of Rio de
Janeiro. Brazil. E-mail: reginalazillotti@gmail.com
IV
Thanks to the National Council for Scientific and Technological Development
(CNPq) for the financial support for the development of the project.
DOI: https://doi.org/10.12957/reuerj.2018.32877
ABSTRACT
Objectives: to evaluate whether interventions proposed in nursing care technology for clients with immunobullous dermatoses contribute to reducing discomfort, and to recognize patterns of discomfort before and after application of the technology. Method: the evaluation protocol was applied to 14 patients hospitalized in dermatology wards in Rio de Janeiro and Mato Grosso do Sul, Brazil, from June 2012 to April 2013. Care was performed by way of identified diagnoses and recommendations in the technology. The role of subjectivity in recognizing comfort patterns in clients with rare diseases indicated the use of fuzzy logic with attributes of pain, mobility, sleep pattern, and body exposure/lesions. The study was approved under CAAE: 0258.0.228.000-11. Results: of the 14 patients, eight reported diminished pain after 24 hours. After one week, three reported larger reductions; five, no change; and five, increased pain. Conclusion: evaluation of patterns of discomfort by fuzzy inferential analysis supported the hypothesis that the technology contributes to promoting client comfort.
Descriptors: Nursing care; dermatology; patient comfort; fuzzy logic.
INTRODUCTION
Promoting the comfort of people with immune bullous dermatosis (ID) becomes a challenge because this disease is disfiguring, uncomfortable, in addition to its complexity and vulnerability to complications such as infections and infestations, which can lead to a lethal success. This situation is aggravated by treatment with immunosuppressant medications.1,2 Nurses are responsible for protecting these people, including when hospitalized in units that do not have therapeutic resources, professionals specialized in dermatology, specific equipment and materials, associated with environmental and structural conditions, which are not always favorable. Despite the highly disorganizing nature of these cutaneous affections, it is observed that the care has been predominantly focused on the drug therapy.3 Thus, the need to expand the care provided to the client, not limited to the compliance with the prescriptions of other health professionals, but rather, the specificity of the nursing care, aiming at attending to the physical, emotional, social and spiritual dimensions is ratified.3,4 Regarding this, it was verified the precariousness of the number of nurses who are specialist in this area; according to the Brazilian Association of Nursing in Dermatology, only 72 nurses were graduated between 2002 and 2016.5 In this context, it should be highlighted the consequent scarcity of nursing references, especially on ID. The rare literature highlights the etiology, pathophysiology and drug therapy without privileging the fundamental aspects of the nursing care.1,2 Faced with a clientele that needs care that goes beyond the competencies of the general nurse, it is essential to produce knowledge through clinical investigations with significant levels of evidence, directing the use of technologies to reduce discomfort and to prevent injuries. It is urgent, therefore, the dissemination of such knowledge to qualify the service to the people in their coexistence with ID. Thus, over twelve years of experience in caring for this clientele, one of the authors has developed alternatives to assess the client, relieve their discomfort and reduce the complications arising from ID. In order to do so, the Protocol of Assessment of the Client in Dermatology (PACD), validated and published in a scientific journal, 6 and the Nursing Care Protocol to the Client with Immuno Bullous Dermatosis (NCPCIBD), both are part of the Nursing Care Technology to the Client with Immuno Bullous Dermatosis (NCTCIBD).
Based on these considerations, and the need to evaluate the proposed technologies scientifically, the following research problem was formulated: can the nursing interventions proposed in the NCTCIBD contribute to reducing the client's discomfort? In view of the above, the objectives were established: to assess if the interventions proposed in the nursing care technology to the client with immunological bullous dermatosis (NCTCIBD) contribute to reduce the discomfort; To recognize patterns of discomfort of people with ID before and after application of the fuzzy logic (FL) technology by algorithm.
THEORETICAL REFERENCE
It is assumed that the nursing intervention based on the philosophical principles of Henderson7 and in Kolcaba's Theory of Comfort, 8 for the care of clients with ID, contributes to reducing the discomfort. For Virgínia Henderson, the nurse's role is specific, autonomous and independent, with its own functions in the attempt to promote comfort, even if shared with other professionals.2 For Kolcaba, the existence of the need for comfort presupposes interventions to maximize it, ratifying the relation between comfort and care.8 In this study, the technology for customer service with ID aims to ratify the nurse's role in promoting comfort, considering that it is an immediate experience, which has three technical senses: relief, calm, and transcendence.8
In order to defend the assumption, it was considered relevant to recognize the patterns regarding the client's discomfort after NCTCIBD-directed interventions. The minimum, medium and maximum standards for the attributes of pain, mobility, sleep pattern, body exposure/lesions, from the objectives proposed in the NCPCIBD, among them, stand out: to relieve the discomfort; to promote healing; to prevent further injury; to prevent infections/infestations; to maintain the hydrolic balance, to control adverse effects of the treatment; to assess social, spiritual and emotional influences; to guide the client/family.
METHODOLOGY
A quasi-experimental, longitudinal and prospective study, using the artificial intelligence from the fuzzy inference perspective to recognize the patterns of discomfort in ID clients. This is about the use of an intelligent system that uses the fuzzy logic (FL) as a qualitative-quantitative method of pattern recognition.9 It was decided on the use of the alternative design for clinical investigation with a single non-randomized group. Such an option occurred due to the ethical and humanistic difficulty of establishing a control group with people affected by the same disease, but who would not benefit from an innovative care that supposedly would promote their comfort. The impossibility of establishing a control group considered that the participants of the research exerted their own control10 when assessing the application and the effects of the interventions obtained through the NCTCIBD. The research was developed from June/2012 to April/2013, in three units, two in university hospitals in Rio de Janeiro and one at a private hospital in Campo Grande, MS, Brazil. These were selected to contemplate institutions with dermatology wards or beds intended for this clientele.
The participants were 14 people (nine with pemphigus vulgaris, two with pemphigus foliaceus and three with bullous pemphigoid), who were included from a sample for convenience10 and met the criteria: hospitalized adults with a diagnosis of ID, independent of previous admissions, gender, age, use of systemic medication or not. Exclusion criteria: people in psychiatric treatment and/or unable to respond to requests. The NCTCIBD was a predictor, independent variable/cause, characterized by the nursing interventions applied to the clients, and the dependent variable/presumed effect,10 the results obtained through the interventions in relation to the intensity of the discomfort. The intensity of the discomfort was measured using a chromatic scale, which served as support of the fuzzy sets for the standards to be measured in relation to the attributes. As a research strategy the nursing consultation was chosen, performed by the researcher according to the phases of the nursing process. The participants were assessed through the use of the PACD. In this, there are 92 nursing diagnoses (NDE) according to NANDA-Internacional.11 In the case of subjects with pemphigus vulgaris, the Pemphigus Vulgaris Mucous Cutaneous Commitment Index (PVMCCI) was adopted.12 The interventions were performed based on the nursing diagnoses identified and the objectives described in the NCPCIBD.
The FL Theory: a reference for data treatment
Due to the fact that it is a group of rare diseases, the sample is reduced, and the FL methodology allows to recognize patterns of discomfort for each client and to compare the taxonomy of levels of discomfort. The subjectivity of the discomfort directed the treatment of the data produced according to the FL embodied in the Fuzzy Sets (FS), a theory that helps in the understanding of the concepts that extrapolate the barriers of the formal logic.13 Thus, the boundaries and limitations imposed by the binary analysis, which would establish only two aspects, by a low, medium and high graded hierarchical classification with their pertinence values are broken. These are sets that do not have well-defined boundaries that have been introduced to deal with problems where transitions from one class to another occur smoothly.13 It was decided to use three FS, a triangle, having as neighbors two trapezes. The support of these FS was constituted by a chromatic scale, because it would facilitate the understanding of the subjects on the intensity of each attribute, since the increase of the color tone meant greater expressiveness, while its reduction, less expressiveness. Thus, the object for the recognition of the discomfort patterns before and after the application of the NCTCIBD for each attribute was made through the use of a form, where each client marked their perception of intensity of each attribute in the support of the chromatic scale, initiated by the white color followed by different shades of yellow to red.
In the fuzzification stage, it was indicated the gradual in the support corresponding to the conceptual analysis of the term comfort recommended by the Kolcaba's theoretical.8 Since it was not allowed the visualization of the FS by the subjects, inhibiting their curiosity, the value of the pertinence of each formulated question was obtained according to the mathematical expression of the equations of the line; being that in the nebulous region, the maximum value of the pertinence of the two sets of the area of intercession was adopted. For example, if the area of intersection of the linguistic terms was indicated as low and medium, we chose the one that found the most pertinence, leading to the low classification. The following three measures were used to assess the reception of the nursing interventions: before (T0), 24 hours after (T1) and one week after (T2) the nursing interventions were received, based on the three technical senses recommended by Kolcaba: relief, calm and transcendence. Thus, the fuzzification procedure, qualitative and quantitative, performs the taxonomy with its pertinence value.13 The association between antecedent and consequent can be translated as: if there is pain and high mobility, the consequent will lead to the end result of maximum discomfort, generating the fuzzy rules. The appreciation of the crossings from the fuzzy inference machines14 allows to determine if the implementation of the NCTCIBD interfered positively or negatively.8 Thus, fuzzy13 inference was activated by three machines that determined the fuzzy rules: if...so, antecedents...consequent. The first one was elaborated with two antecedent attributes, pain and mobility, considering that the pain interferes in the mobility and the mobility can cause pain, having as a consequence, the discomfort patterns (low, medium or high). In this sense, the rules of the first fuzzy machine for determining the discomfort patterns according to the linguistic terms inferred by the pain and mobility attributes can be broken down: if the client indicates high pain and high or medium or low mobility, then their discomfort tends to be maximum; If they indicate medium pain and high or medium mobility, then their discomfort tends to be medium; If they indicate medium pain and low mobility, then their discomfort tends to be maximum; If they indicate low pain and high mobility, then their discomfort tends to be minimum; If they indicate low pain and medium mobility, then their discomfort tends to be medium; If they indicate low pain and low mobility, then their discomfort tends to be maximum. In the second machine, the standard attribute of sleep was included besides the pain and mobility attributes, since it interferes in the discomfort, establishing the following rules: If the client indicates high pain and high or medium or low mobility and high or medium or low sleep pattern, then their discomfort tends to be maximum; If they indicate medium pain and high or medium mobility and high or medium sleep pattern, then their discomfort tends to be medium; If they indicate medium pain and low mobility and low sleep pattern, then their discomfort tends to be maximum; If they indicate low pain and high mobility and high sleep pattern, then their discomfort tends to be minimum; If they indicate low pain and medium mobility and average sleep pattern, then their discomfort tends to be medium; If they indicate low pain and low mobility and low sleep pattern, then their discomfort tends to be maximum.
In the third machine, to the pain and mobility attributes, it is included the attribute exposure of the body and injuries, since such exposure can inhibit the mobility motivated by the constraint felt by the client. Rules: If they indicate high pain and high or medium or low mobility and the exposure of the body and lesions is high or medium or low, then their discomfort tends to be maximum; If they indicate medium pain and high or medium mobility and the body exposure to the lesions is high or medium, then their discomfort tends to be medium; If they indicate average pain and low mobility and low body and injury exposure, then their discomfort tends to be maximum; If they indicate low pain and high mobility and high body and injury exposure, then their discomfort tends to be minimal; If they indicate low pain and medium mobility and the exposure of the body and the lesions is medium, then their discomfort tends to be medium; If they indicate low pain and low mobility and low body and injury exposure, then their discomfort tends to be maximum.
Thus, the veracity of the hypothesis of the association by the cross between the attributes contributes to reveal if the implementation of the NCTCIBD promotes the reduction of the discomfort. Although the promotion of comfort was the goal of the NCTCIBD, it was considered that the assessment, within a period of seven days, might not necessarily promote comfort, but reduce, maintain or increase the discomfort among clients.
This is a clipping of a doctoral thesis defended in 2014. The project was submitted to the approval of the Research Ethics Committee of the Pedro Ernesto University Hospital of the State University of Rio de Janeiro, approved by CAAE: 0258.0.228.000-11, registry 3119/2011 and Resolution No. 466/2012 of the National Health Council.
RESULTS AND DISCUSSION
Through the application of the PACD, the subjects of the study 17 DE were highlighted, among them the risks of: unstable glycemia, electrolyte and fluid imbalance, compromised human dignity, contamination, infection, unbalance of the body temperature; in addition to ineffective protection, poor knowledge, body image disorder, low situational self-esteem, impaired social interaction, anxiety, contamination, impaired skin integrity, impaired comfort, and social isolation.
It was observed that of the nine clients with medical diagnosis of pemphigus vulgaris, one presented index = 30; one = 35; one = 40; three = 60; two = 80 and one = 100. The FL allowed us to analyze the pertinence of each attribute in moments T0, T1 and T 2 during the assessment of the 14 participants. Regarding the pain attribute, it was found that 11 clients reported high and medium-intensity pain before starting the proposed care (T0) and, after 24 hours, only six were under these conditions, which corresponds to a reduction of 45%. In the following period (T2), only one person reported maintaining a high intensity pain.
The mobility attribute showed that 7 (50%) clients indicated low mobility before the nursing care was completed (T0), revealing the interference of the cutaneous lesions, and after the first day of intervention, none were considered in this condition, which was maintained until the following week (T2).
Before applying the NCTCIBD (T0), 13 participants were considered to have altered sleep patterns, a fact modified in T1 and T2.
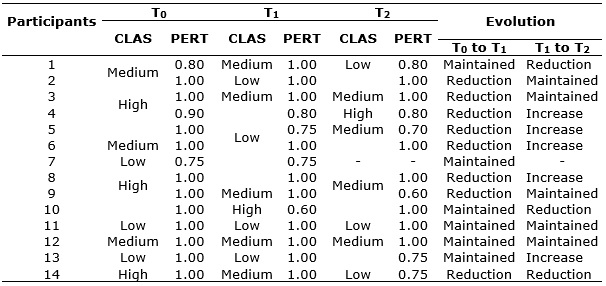
A qualitative-quantitative analysis was performed under the temporal optics of the pain attribute (T0, T1 e T2) of the 14 participants' statements according to the linguistic terms and their pertinence values assigned in the closed range of zero to one. If two clients are classified with high pain, the one that obtains a greater degree of pertinence should be considered in a more serious situation. Of the 14 participants, eight had pain reduction from T0 to T 1, while after one week, of the 13 clients who continued hospitalized, three further had their pain reduced, five maintained and five increased. See Table 1.
TABLE 1:
Evolution of the subjects according to the linguistic terms in relation to
the pain attribute in moments T0, T1 and T2 with their respective pertinence. Rio de Janeiro, Brazil,
2014. (N=14)
Notes: CLASS: Classification; PERT: Pertinence. Subject 7 hospitalized for only
four days, total 13 clients in T2.
Association between the NCTCIBD and the discomfort reduction
The cross between pain and mobility attributes revealed that eight of the 14 clients improved the discomfort from T0 to T1, being that from T1 to T2, of the 13 clients, nine maintained the frame of reduction of the discomfort or even less discomfort. Only four reported increased discomfort, according to Table 2.
TABLE 2:
Pattern of discomfort in linguistic terms by pain and mobility and pain,
mobility and exposure of the body and injuries, T0, T 1 e T2. Rio de Janeiro, Brazil, 2014. (N=14)
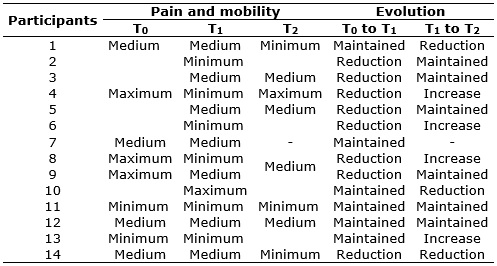
Note:
participant 7 hospitalized only four days, total of 13 clients in T2.
Adding the pain and mobility attributes to the body and lesion exposure attribute, it was found that, after one day of hospitalization, the half investigated (seven) presented a reduction of discomfort. Four subjects reported the reduction of discomfort only of the moment T0 to T 1. It should be highlighted that only one subject mentioned their discomfort increased from T0 to T1, however, reported the reduction of the discomfort from T1 to T 2, as shown in Table 3.
TABLE 3:
Pattern of linguistic discomfort due to pain, mobility and exposure of the
body and lesions, T0, T1 and T2. Rio de
Janeiro, Brazil, 2014. (N=14)

Note:
participant 7 hospitalized only four days, total of 13 clients in T2.
It should be highlighted that the references that address the nursing care to ID clients are scarce.1,2 Thus, the results reveal the essential role of the application of a specific nursing care technology to reduce the discomfort of this clientele. Regarding this, it is important to mention a study carried out with the objective of identifying the nursing diagnoses in clients with immune bullous dermatoses, being identified, among the main ones, the ineffective protection, with defining characteristics - deficiency in immunity and immobility; the nursing diagnosis impaired comfort, which presented among the defining characteristics the pattern of disturbed sleep and the report of feeling uncomfortable, besides the risk/related factor - lack of privacy; and the nursing diagnosis risk of compromised human dignity, with risk/related factors - stigma and body exposure.15
Regarding the discomfort, one cannot fail to mention the pain felt by clients with ID, a subjective and personal experience associated with actual or potential damage to the tissues.
In the skin, the pain is characterized by a multidimensional experience, being able to vary in the sensorial intensity, besides suffering affective-emotional interferences. Described as the fifth vital sign, acute or chronic pain, should be evaluated and recorded from the client's admission.16 Thus, it is emphasized that the comfort promotion begins at the moment of hospitalization, during the first interaction and welcoming of the client, social and spiritual support,17 highlighted in the protocol. It was found that the reduction of pain and exposure of the body and lesions and increased mobility and sleep pattern occurred from T0 to T1 in a quick and simultaneous way; the pain, especially in the first 24 hours. This evolution was attributed mainly to the application of the dressing proposed in the NCPCIBD, which allowed the rest and mobility in the bed, preventing the adhesion of the lesions to the clothes and contact surfaces, besides facilitating the extension/flexion of the limbs and sitting outside the bed.18 The proposed dressing does not cause adherence to the lesions and, because it promotes greater client mobility, it contributes to the prevention of pressure injuries, a challenge in everyday practice, 19 mainly because they are people with compromised skin integrity. In addition to preventing infections and infestations, the dressing protects the disfigured body, reducing the exposure of the body image compromised to stigmatizing eyes, which promotes the promotion of the self-esteem.
The least expressive evolution for all the attributes occurred in the comparison of the results from T1 to T2, however, the majority remained in a more favorable condition than in T0. The results of Table 2 show that the NCPCIBD interventions reduced the pain and mobility discomfort in 24 hours in 50% of subjects and there was no worsening of the discomfort in the transition from T0 to T 1. In the migration from T1 to T2, four subjects presented an unexpected evolution, since one went from the minimum discomfort to the maximum and the others to the medium. In the evolution of the association from T0 to T2, a satisfactory evolution was observed, since seven participants had maximum discomfort and five in T0, and in T2, only one client indicated maximum discomfort, according to Table 2.
The interaction of pain with mobility and exposure of the body/lesions revealed that from T0 to T1, clients had their discomfort reduced (seven), maintained (six) and increased (one), while from T1 to T2, four, six and three presented, respectively, the same gradation. It was observed that there was an increase in discomfort for three people from T1 to T2 , which was not expected. This is explained by the delay in the individualized response to medication. In this sense, it is emphasized that both the nursing care and the response to the drug therapy should converge.
From the point of view of the multiprofessional care, it is emphasized that on the physical aspect there was improvement when the care proposed in the NCPCIBD was carried out, since they minimized the discomfort; promoted healing and prevented injury, infections/infestations; and, controlled adverse effects. In the psycho-spiritual, it is observed that the subjects demonstrated resilience in the fight against the disease and favoring the reduction of anxiety and the interpersonal relationship. In the socio-cultural context, the welcoming was facilitated by the willingness to listen and establish a relationship of trust, as proposed in the protocol.
The presence of DE was observed – willingness to improve self-care, coping, hope, disposition and comfort, showing a desire to increase independence in maintaining health and well-being; there was also the expression of the desire to increase comfort, relaxation, and to intensify the resolution of complaints.11
The application of the NCPCIBD provided the basic needs in the technical sense: relief and calm. As for comfort, outcome of care, and sensitive to changes in the timeline, it is considered that transcendence (the state in which one is above problems or pain),8 was achieved by eight of the 14 clients, especially those with extensive injuries. Among those with pemphigus vulgaris, those with an index equal to or above 40 were those who had the greatest reduction of discomfort.
CONCLUSION
A qualitative and quantitative fuzzy inferential analysis allowed us to evaluate if the interventions proposed in the NCTCIBD contribute to reduce the discomfort of the clients, which pointed to the veracity of the substantive hypothesis, especially those with extensive skin lesions. Therefore, it was possible to follow the evolution of people with ID by recognizing patterns of discomfort, based on their active participation, expressed in the assessment of each attribute considered fundamental to identify the discomfort in three moments of interlocution. The results from a qualitative and quantitative perspective of nursing practice point to possibilities to guide other research, involving phenomena in which the quantification is insufficient to decide on the efficacy of the intervention. Due to the lack of qualitative and quantitative studies related to the nursing care provided for this clientele, this study provides nurses and researchers with essential information, with a view to a decent and personalized service, with a view to systematization, besides being a contribution for caring, educating, and research in nursing in the dermatology area.
REFERENCES
1.Brandão ES, Santos I dos, Carvalho MR, Pereira SK. Nursing care evolution to the client with pemphigus: integrative literature review. Rev. enferm. UERJ. [Internet]. 2011 [cited in 2018 Jan 15]. 19(3): 479-84. Available from: http://www.facenf.uerj.br/v19n3/v19n3a24.pdf
2.Brandão ES, Santos I dos. Evidences related to the care of people with pemphigus vulgaris: a challenge to nursing. Online Braz. J. nurs. (Online). [Internet]. 2013 [cited in2018 Jan 15].12(1):162-77.Available from: https://www.objnursing.uff.br/index.php/nursing/article/view/367455
3.Santos I dos, Brandão ES, Clos AC. Dermatology nursing: sensitive listening skills and technology for acting skincare. Rev. enferm. UERJ. [Internet]. 2009 [cited in 2018 Jan 18]. 17(1): 124-30. Available from: http://www.facenf.uerj.br/v17n1/v17n1a23.pdf
4.Santos I dos, Caldas CP, Gauthier J, Erdmann AL, Figueiredo NM. Caring for the whole person: the contributions of aesthetics/sociopoetics perspectives to the field of nursing. Rev. enferm. UERJ. [Internet]. 2012 [cited in2018 Jan 18]. 20(1): 4-9. Available from: http://www.facenf.uerj.br/v20n1/v20n1a02.pdf
5.Associação Brasileira de Enfermagem em Dermatologia. Titulados. São Paulo: SOBENDE; 2017. http://sobende.org.br/wp/titulados/
6.Brandão ES, Santos I, Lanzillotti RS. Validation of an instrument to assess patients with skin conditions. Acta Paul. Enferm. (Online) [internet]. 2013 [cited in 2018 Jan 20]. 26(5): 460-6. Available from: http://www.scielo.br/scielo.php?pid=S0103-21002013000500009&script=sci_arttext&tlng=enn
7.Ferin CF, Rodrigo MTL. El modelo de Virginia Henderson. In: Ferrín CF, Gómez MVN. De la teoria a la práctica: el pensamiento de Virginia Henderson en el siglo XXI. Barcelona: Masson; 1998.p.33-8.
8.Down T. Katherine Kolcaba: theory of confort. In: Tomey AM, Alligood MR. Modelos y teorías em enfermería. 7ª ed. Barcelona (ES): Elsevier-Mosby; 2011. p.706-21.
9.Drablei RG, Molii ACA, Legeyiii AP. Evaluation of the use of fuzzy logic for predicting risk of Human Papiloma Virus. Rev. Eletron. de Comum. Inf. Inov.Saúde. [internet]. 2014 [cited in 2018 Jan 25]. 8(3): 344-358. Available from: https://www.reciis.icict.fiocruz.br/index.php/reciis/article/view/674
10.Hulley SB, Cummings SR, Browner WS, Grady DG, Newman TB. Delineando a pesquisa clínica: uma abordagem epidemiológica. 3ª ed. Porto Alegre (RS): Artmed; 2008.
11.NANDA International. Diagnósticos de Enfermagem da NANDA: definições e classificação 2012-2014. Porto Alegre (RS): Artmed; 2013.
12.Souza SR, Azulay-Abulafia L, Nascimento LV. Validation of the Commitment Index of Skin and Mucous Membranes in Pemphigus Vulgaris for the clinical evaluation of patients with pemphigus vulgaris. AnBras.Dermatol. [Internet]. 2011 [cited in2018 Jan 24]. 86(2): 284-91. Available from: http://www.scielo.br/pdf/abd/v86n2/v86n2a12.pdf
13.Zadeh LA. Fuzzy sets. Inform.Control. 1965; 8: 338-53.
14.Brandão ES, Santos I dos, Lanzillotti RS, Moreira Junior A. Proporsal for recognation of the comfort pattern in clientes with pemphigus vulgaris using fuzzy logic. Rev. Esc. Enferm. USP. [Internet]. 2013 [cited in 2018 Jan 26]. 47(4): 958-64. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0080-62342013000400958&lng=en&nrm=iso&tlng=pt
15.Brandão ES, Santos I dos, Lanzillotti RS.Ferreira AM, Gamba MA, Azulay-Abulafia L. Nursing diagnoses in patients with immune-bullous dermatosis. Rev. Latinoam. Enferm. (Online) [Internet]. 2016 [cited in 2018 Mar 24]. 24 e 2766. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-11692016000100385&lng=en&nrm=iso&tlng=en&ORIGINALLANG=en
16.Bottega FH, Fontana RT. Pain as the fifth vital sign: use of the assessment scale by nurses in general hospital. Texto contexto enferm [Internet]. 2010 [cited in 2018 Mar 24]. 19(2): 283-90. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-07072010000200009
17.Ponte KMA, Silva LF, Aragão AEA, Guedes MVC, Zagonel IPS. Clinical nursing care to comfort women with acute myocardial infarction. Texto & contexto enferm. [Internet] 2014 [cited in 2018 Mar 30]. 23(1): 56-64. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-07072014000100056
18.Brandão ES, Santos I dos, Lanzillotti RS. Reduction of pain in clients wit autoimmune bullous dermatoses: evaluation by fuzzy logic. Online Braz.J. nurs. (Online). [Internet]. 2016 [cited in 2018 Mar 24]. 15(4): 675-82. Available from: https://www.objnursing.uff.br/index.php/nursing/article/view/5467/pdf
19.Brandão ES, Mandelbaum MHS, Santos I dos. A challenge in nursing care: preventing pressure ulcers in the client. Rev. enferm. UFPE on line [Internet]. 2012 [cited in 2018 Feb 02].6(8): 1965-70. Available from: https://periodicos.ufpe.br/revistas/revistaenfermagem/article/viewFile/7292/6725