Source: Pubmed, BVS - Biblioteca Virtual em Saúde e Portal de Periódicos Capes/ MEC. Access Dec. 2017.
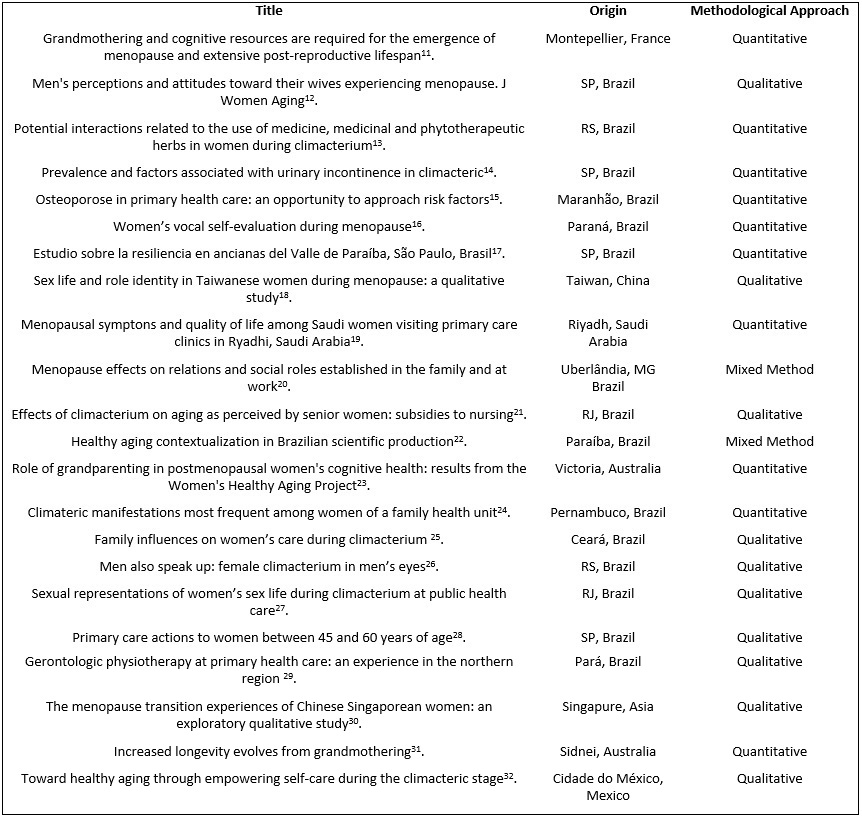
FIGURE 1: Articles selected according to title, origin, and methodological approach. Period 2012-2017.
REVIEW ARTICLE
Knowledge produced on climacteric, family and aging
Glaucimara Riguete de Souza SoaresI; Selma Petra Chaves SáII; Rose Mary Costa Rosa Andrade SilvaIII; Ivis Emília Oliveira SouzaIV; Lucia Helena Garcia PennaV; Marcele ZveiterVI
I
Glaucimara Riguete de Souza Soares. Nurse; Ph.D Escola de Enfermagem Aurora
de Afonso Costa. Universidade Federal Fluminense. Brazil. E-mail: glau_riguete@hotmail.com
II
Selma Petra Chaves Sá; Ph.D in nursing. Nurse. Professor, Universidade
Federal Fluminense. Brazil. E-mail: selmapetrasa@gmail.com
III
Rose Mary Costa Rosa Andrade Silva; Nurse. Ph.D in nursing. Professor,
Universidade Federal Fluminense. Brazil. E-mail: roserosauff@gmail.com
IV
Ivis Emília Oliveira Souza; Nurse; Ph.D in nursing. Professor, Universidade
Federal do Rio de Janeiro. Brazil. E-mail: ivis@superig.com.br
V
Lucia Helena Garcia Penna. Nurse; Ph.D in Nursing. Professor of nursing,
Universidade do Estado do Rio de Janeiro. Brazil. E-mail: luciapenna@terra.com.br
VI
Marcele Zveiter; Ph.D in nursing. Nurse. Professor of nursing, Universidade
do Estado do Rio de Janeiro. Brazil. E-mail: marcelezveiter@hotmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2018.32588
ABSTRACT
Objective: to examine the knowledge produced on climacterium, family and aging. Method: this integrative literature review used the VHL, Pubmed and Capes Journal Portal databases (2012-2017). Results: 22 articles were selected and analyzed by two categories: the family's influence on the aging process of women in the climacteric phase, and coping with the climacterium and its physical and psychological disorders. Conclusion: study of the climacterium needs to go beyond the clinical symptomatology of menopause, with a view to promoting active, healthy aging. The family is an integral part of this process and, accordingly, nurses and other professionals in multidisciplinary teams should include it in the process of learning about, understanding, following up on and curing of transitory symptoms that can affect women in the menopause/climacteric phase.
Descriptors: Climacteric; family; aging; nursing.
INTRODUCTION
In 2018, the Brazilian population has about 280 million people, 50.67% of which integrated by females1. In this context, female aging unveils the challenge of setting up priorities on educational measures concerned with prevention and health promotion as a goal to better quality of living and life expectancy.
Quality of living refers to the interest in life, and has always been an issue for human beings. Therefore, quality of living is not out there to be reached, but to be incorporated to one's daily life out of individual and/or collective efforts. It is granted that what matters in life is the search of good quality in face of his or her chances to act2.
Effects of aging have become a political priority for the World Health Organization, which has brought out into light the concept of active aging. It is applied to both individuals and population extracts and is characterized as an optimization process of health, participation, and safety opportunities aiming at improving quality of living as people age. Today aging has been undergoing a feminization process, for women live at least 4.5 years longer than men3.
Considering profile changes among health users concerning aging and longevity, it must be highlighted that professionals, male nurses in particular, must pay attention to that inflection beyond biological functioning. They must propose prevention and health promotion measures to be integrated into the several women's health care lines.
Attention to climacterium and menopause as part of a far-reaching aging process is a care line which must be accounted for, not just by the woman and by those who surround her, but also by health professionals. It is challenging to consider the implications for female identity along the vital cycle, for both climacterium and aging generate new feelings, involving losses and gains4. This research accounts for climacterium beyond the context of the female being experiencing the phenomenon.
The climacterium is a biological phase in life, a turning point between the reproductive and the non-reproductive phases, topped by the menopause, its physiological sign, around 48 and 50 years of age. If there are symptoms, they comprise the climacterium syndrome, which might account for emotional, social, and physical changes in women's life5.
Nurse care proves to be crucial at this moment in women's life, for that coincides with the days when children leave home and women realize their physiological impediment to maternity on account of absent menstruation 6. Such facts may generate conflicts between women and their families – a term used in the plural on account of the decline of the traditional family with the attached housewife figure.
Major transformations affecting women's presence in the family context must be recalled: mother and homemaker gave way to a woman that, in addition to procreation and house management, is busy with a job outside the home, goes up on the social scale, experiences a liberating sexuality, and not seldom, is the family head. In this sense, the climacterium/menopause phase of fully contemporary women must not be attached to a family model in which individuals integrate the same nucleus in the same household, but instead, it must be attached to families – inter-group alliances which can provide human beings with their socially meaning experience7.
The guiding question in this research is as follows: what scientific knowledge has been produced on the intersection between the concepts of climacterium, family, and aging? Thus, this literature review aims at analyzing the knowledge produced on climacterium, family, and aging.
METHODOLOGY
The research method adopted herein has been an integrative literature review, which aims at synthesizing results on a theme or on an issue in a systematic and encompassing way to provide major subsidies to a specific subject or issue8. Therefore, this review has sought electronic articles on climacterium, family, and aging to analyze what knowledge has been produced on this theme. To that purpose, the following steps have been followed: identification of theme, search of the literature on electronic medium, categorization, and assessment of the studies found in the integrative review, interpretation of results, and finally, synthesis of knowledge found in the research analyzed.
Selection was made according to the following inclusion criteria: production in article format, whose descriptors were climacterium, family, and aging (booleano AND, via Decs/ Mesh-Terms), in full text format, published in the last 5 years, and theme-related titles. Exclusion criterion considered articles unrelated to the research issue.
Sources selected with respective figures are presented as follows: Biblioteca Virtual em Saúde (one article - BDENF), PUBMED (Five articles and Portal de Periódicos Capes: CINAHL (six articles), SCOPUS (six articles), EBSCO (six articles) and WEB OF SICENSE (two articles).
After thorough reading of main themes in the articles, there followed content analysis as proposed by Bardin9. Data were treated on the basis of the following steps: pre-analysis, surface and in-depth reading, coding, result treatment, and interpretation. Two categories were considered: family influence in the aging process undergone by women during climacterium, and coping with climacterium and respective disorders affecting women's physical and psychological nature.
RESULTS AND DISCUSSION
The aging phenomenon has been represented on the social scene by means of a higher concentration of publications in the health area, especially in nursing and psychology10.
Out of the 22 productions selected 11-32, 15 were conducted in Brazil and seven abroad. the prevalence of Brazilian studies on international databases stands out. Equivalence on the nature of the studies has been identified as follows: 10 with quantitative approach, 10 with qualitative approach, exception made to two with mix approach. See Figure 1.
Source:
Pubmed, BVS - Biblioteca Virtual em Saúde e Portal de Periódicos Capes/
MEC. Access Dec. 2017.
FIGURE 1:
Articles selected according to title, origin, and methodological approach.
Period 2012-2017.
Categories emerging out of this integrating review are treated below.
Family influence in women's aging process during climacterium
Analysis of family influence as a part of women's aging during climacterium has highlighted the relation between menopause, ovulation discontinuation, and the end of life expectancy. The Maternal Hypothesis was under discussion, that is, fertilization regulation as of menopause along its natural evolution is found to be likely to occur since the older the woman the higher the risk for death during labor11; additionally, the Grandmother Hypothesis followed, which opens up into longevity as it underlines their daughters' fertility on a horizon with grandchildren, as that is an instance of a lengthy fertile life12. Beyond reproduction, grandmothers are present and capable of promoting cognition as well as the social engagement of their daughters when they offer their grandchildren both assistance and company13.
High life expectancy is promising out of this interaction opportunity between mothers, daughters, and grandchildren. A lengthier life span surpasses the detrimental effects of aging as of the adoption of necessary care in face of time-related changes33. A pleasant passage through climacterium is crucial to healthy aging. On that scene, active aging policies must be fostered. The aging person must accumulate intellectual, social, and financial capital. The public sector, the academy, institutions in civil society, the private sector, and the media must all provide for that assistance33.
Usually, senior women claim that climacterium triggers aging because it initiates a senility process, and several physical changes, cultural influences, changes in life style, and personal history take place21.
One must consider that the health-disease process is a complex phenomenon, conditioned by biological, psychological, cultural, economic, and political factors; and the health needs of those who age are related to multiple dimensions of the real as well as to the particularities of health or disease phenomena which affect individuals and their families34. The family is regarded as an institution of social support, which generates coping conditions towards higher quality of living25.
The family context may have effects on women`s experience of the climacterium. Among central positive factors, loving care and identity relations stand out upon coping with stress. Experience shared by elderly females in the family attenuates anxiety brought about by the expectations as to the unknown18. Among negative factors, lack of listening between spouses may cause conflicts. Engaging in strategies which involve men's participation in the care provided to women during climacterium proves to be decisive to attenuate misunderstandings12.
Men are not at ease talking about climacterium-related issues. Their speeches usually show to-the-point answers; maybe because they might feel uncomfortable admitting they ignore how to about providing the help their companions are in need of26. Those who best understand the changes their wives undergo during menopause can provide emotional support to improve quality in their marital relation12. Thus, family contexts have attracted the interest of scholars and researchers who aim at analyzing and understanding their stories, their changes, their adaptations, their ways of being and the effects to better living35. Seeking and obtaining support among family and friends during climacterium/menopause proves to be relevant to a better experience within that period30.
Resulting symptoms of menopause and climacterium can alter quality in the relations at work and in the family, can have effects over women's well-being, and can affect their routine and/or interpersonal relations. Going through climacterium unprepared may generate difficulty about coping with the emerging challenges and still compromise self-esteem, relationships, and quality of living20. In Brazil, scarce information on that phenomenon has stronger effects on low-income families. In addition, low or no schooling as well as lack of search for health services affect understanding menopause36.
In the context of social representation, sexual life of women duting climacterium is grounded on stereotypes stemming from a conservative cultural background on which sex and love go hand in hand. oweverHhhHowever, women`s sexual aging takes place within a heavily prejudiced culture involved in fears and silences. Socially constrained, they are unable to get ready for a sexually satisfactory and pleasant life 27. Assistance to women undergoing climacterium, including those sexuality-related aspects, must be a priority of Public Health Policies, for quite a few of them are concerned with body changes, sexual pleasure, and reproductive purpose37.
Women's aging during climacterium/menopause is associated to an exhaustion of emotional resources, especially in view of simultaneous losses. Negative effects, such as the death of spouses and friends damage women undergoing climacterium as for physical and psychological engagement17. Children's growth and their leaving home can signal to a serious loss, especially to those who have had a life-long devotion to the family 38. Therefore, female empowerment can improve perception of climacterium/menopause, as well as of the relevance of self-care32.
Approaching healthy aging encompasses regarding and defending the aging person in the family and in society in a participating and constructive way to assure her full social inclusion. Health professionals have the mission to devote to primary healthcare, which must be resolution-oriented, integral, and humanized22. Inclusion of psychological care in the health net, which ensures efficient assistance from initial symptoms of climacterium/menopause becomes relevant to promote quality of living during aging38.
Coping with climacterium and its disorders in women's physical and psychological nature
Melancholy and severe headaches were the most frequent complaints reported by women going through climacterium, higher than arthralgia and myalgia. When they get to understand the reasons for such manifestations, symptoms are lighter as well as the impact on their lives. When fully assisted on menopause, they can go through it with fewer symptoms, especially when it comes to the psychological ones24. Women's perceptions on their body and emotional changes during climacterium must be listened to and understood, so that they can be guided by nurses, in special those in family care strategies, who develop listening and education action-based strategies39. However, in health units, there's lack of specific guidance to women between 45 and 60, and assistance is provided spontaneously, not on an appointment basis28.
Despite the principles of integrality proposed to women's health, there are still few health-promotion activities during climacterium25. In health care actions, professionals reported that female demands start with menopause-related physical symptoms, whereas health care units are still organized for to curative and/or preventive aspects, limited to health-disease process 28.
Voice alteration is a frequent symptom during climacterium/menopause, and that can have negative effects over quality of living. The more women lose their voice power, the more strongly they show their stress, for that affects their social relations negatively16. In the context of public health over a decade ago, prevention campaigns as well as educative programs concerned with voice disturbances were feeble, even among professional groups in which the voice is the main work tool40. That proves to be the result of ignorance still remaining to this date.
Another highly frequent complaint concerns urinary incontinency. In that case, the proposal of primary care strategies proves relevant. Precocious professional intervention from pre-natal moments can preserve pelvic muscles, a prevention gain concerning women's urinary incontinency. That disturbance is usually installed during the postmenopausal span, and can be accounted for by the drop on estrogen levels, which play a major role in urinary continency mechanism. That condition can become incapacitating and can generate high social, physical, economic, and psychological impact 14.
The introduction of gerontological physiotherapy exercises in primary family care units has been a gain to aging population and which requires related adaptations to those needs, as for example, the post menopause period. During aging, women are susceptible to obesity, diabetes, hypertension, muscle weakening, genital atrophy, and urinary incontinency – their major health problems. Thus, primary care physiotherapy to women has been a favorable practice to physical improvement, to self-esteem and consequently has been having positive effects to social and family realationship29.
Osteoporosis turns out to be an additional physical condition which can throw off balance the quality of living of women going through climacterium. It is characterized by low levels of bone mass which make women susceptible to fractures. In primary care, health professionals must be able to identify risk factors, for it is a multifactor disease with increasing prevalence in the female population15.
Physical and psychological climacterium/menopause occurrences prompt women into seeking clinical cure; there was research related to the potential interactions related to the simultaneous use of medicine, medicinal herbs and phytotherapeutic products in women during climacterium. Findings show that intervention strategies must be proposed to avoid possible medical interactions, as well as self-medication on the basis of medicinal herbs and phytotherapeutic products13. In this sense, actions aiming at awareness and training of professionals in charge of prescribing medicine, concerning the safe use of medicinal herbs and phytotherapeutic products, whether or not associated with medicine, are relevant tools to women care. Training of community agents is also relevant by means of the work tools provided for by the Health Department, containing material and certified lists of medicinal herbs in order to guide them into clarifying issues and identifying demands by users and submitting them to health teams 13. It is common sense for women to associate several medications to treat symptoms resulting from climacterium and menopause, related to changes in their sexuality. Part of them reports that physical changes make sexual intercourse hard, and therefore they avoid active sexual life, on the basis of that major discomfort Others try to improve their sex life on the basis of either behavior changes or medication comprised of hormone replacement. Used world-widely, hormones are synthesized in laboratories and have effects similar to those produced by the female body. Potential adverse effects are a theme of interest to public health on account of the potential impact they might have on the population exposed39. Saudi women, for example, are not into synthetic hormones and regard both climacterium and menopause as a necessary development in life. They complain less than western women do of heat waves, the latter also showing joint pain, in addition to physical and mental exhaustion19.
CONCLUSION
The analysis of scientific production on climacterium, family, and aging has shown concern and has pointed to the need of studying beyong clinic symptomatology of menopause. Research is likely to show inovations related to health promotion, prevention of diseases, and quality of living as the pillars to women's active and healthy aging during climacterium.
Outstanding determiners can be found in the valuation of family influence on aging as well as on adaptation to that new phase in life. In this sense, nurses as well as other multidisciplinary team professionals must bring family members into knowledge, understanding, follow-up, and cure of transient symptomatology which may affect women during climacterium/menopause. Family makes a universe of multiple relations among its members and must be valued in the search for integral care.
REFERENCES
1.Instituto Brasileiro de Geografia e Estatística [internet]. Projeção da população do Brasil e das unidades de federação. [cited 2018 Jan 01]. Available from: http://www.ibge.gov.br/apps/populacao/projecao/ .
2.Almeida MAB, Gutierrez GL, Marques R, organizadores. Qualidade de vida: definição, conceitos e interfaces com outras áreas de pesquisa. São Paulo: EACH; 2012.
3.Centro Internacional de Longevidade Brasil. Envelhecimento ativo: um marco político em resposta à revolução da longevidade. [internet] [cited 2018 Jan 01]. Available from: http://ilcbrazil.org/portugues/wp-content/uploads/sites/4/2015/12/Envelhecimento-Ativo-Um-Marco-Pol%C3%ADtico-ILC-Brasil_web.pdf
4.Silva JPL, Marcolino EC, Fernandes NMS, Moura IM, Araújo MZ. Representações do climatério e suas repercussões na vida da mulher: uma revisão sistemática. In: Anais do IV Congresso Internacional de Envelhecimento Humano; 2015; Paraíba, Brasil. Paraíba(PB): IV Congresso Internacional de Envelhecimento Humano; 2015.
5.Pereira ABS, Martins CA, Pereira MS, Lima JR, Souza ACS, Ream PSF. Atenção ao climatério realizada por profissionais da estratégia saúde da família. Rev. enferm. UERJ. 2016; 24(1):e13122.
6.Oliveira ZM, Vargens OMC, Acioli S, Santos RS. Nursing care in the climateric: demedicalizing perspective in primary health care cuidado. Rev. enferm. UFPE on line.2017; 11(Suppl. 2):1032-43.
7.Strey MN, Silva Neto JAS, Horta RL. Família e gênero. Porto Alegre (RS): EDIPUCRS; 2007.
8.Ercole FF, Melo LS, Alcoforado CLGC. Integrative review versus systematic review. REME rev. min. enferm. 2014; 18:12-4.
9.Bardin L. Análise de conteúdo. São Paulo: Editora 70; 2011.
10.Silva MC, Ogata MN, Oliveira DC. O estado de arte das produções científicas nacionais das representações sociais do envelhecimento na perspectiva da saúde. Rev. Kairós. 2015; 18(esp. 19):49-63.
11.Aimé C, André JB, Raymond M. Grandmothering and cognitive resources are required for the emergence of menopause and extensive post-reproductive lifespan. PLoS Comput. Biol. 2017; 13(7):e1005631.
12.Rodolpho JRC, Quirino BC, Hoga LAK, Rosa PLFS. Men's perceptions and attitudes toward their wives experiencing menopause. J. Women Aging. 2016; 28(4):322-33.
13.Gelatti GT, Oliveira KR, Colet CF. Potenciais interações relacionadas ao uso de medicamentos, plantas medicinais e fitoterápicos em mulheres no período do climatério. Rev. pesqui. cuid. fundam. (Online). 2016; 8(2):4328-46.
14.Dellú MC, Schmitt ACB, Cardoso MRA, Pereira WMP, Pereira ECA, Vasconcelos ESF et al. Prevalence and factors associated with urinary incontinence in climacteric. AMB rev. Assoc. Med. Bras. 2016; 62(5):441-6.
15.Costa ALD, Silva MACN, Brito LMO, Nascimento ACB, Barbosa MCL, Batista JE et al. Osteoporosis in primary care: an opportunity to approach risk factors. Rev. bras. reumatol. 2016; 56(2):111-6.
16.Basílio BN, Ribeiro VV, Pereira EC, Leite APD. Vocal self-assessment of women in menopause. Rev. CEFAC. 2016; 18(3):649-55.
17.Araújo CLO, Faro ACM. Estudio sobre la resiliencia en ancianas del Valle de Paraíba, São Paulo, Brasil. Enfermería Global. 2016; 15(2):63-80.
18.Yang CF, Kenney NJ, Chang TC, Chang SR. Sex life and role identity in Taiwanese women during menopause: a qualitative study. J. Adv. Nurs. 2016; 72(4):770-81.
19.AlDughaither A, AlMutairy H, AlAteeq M. Menopausal symptoms and quality of life among Saudi women visiting primary care clinics in Riyadh, Saudi Arabia. Int. J. Womens Health. 2015; 29(7):645-53.
20.Lomônaco C, Tomaz RAF, Ramos MTO. O impacto da menopausa nas relações e nos papéis sociais estabelecidos na família e no trabalho. Reprod. clim.2015; 30(2):58-66.
21.Silva GF, Moura MAV, Almeida MVS, Sá SPC, Queiroz ABA. Climacteric influence for aging in the perception of elderly women: subsidies for nursing. Rev. eletrônica enferm. 2015; 17(3):1-8.
22.Medeiros FAL, Nóbrega MML, Medeiros ACT, Bittencourt GKGD, Leite GA. Contextualization of healthy ageing in the brazilian scientific production. Rev. enferm. UFPE on line. 2015; 9(2):985-93.
23.Burn KF, Henderson VW, Ames D, Dennerstein L, Szoeke C. Role of grandparenting in postmenopausal women's cognitive health: results from the Women's Healthy Aging Project. Menopause. 2014; 21(10):1069-74.
24.Paiva ER, Silva MM, Oliveira CDB, Leal IHS, Araújo VS, Dias MD. Climateric manifestations most frequent among women of a family health unit. Rev. enferm. UFPE on line. 2013; 7(11):6430-7.
25.Santos JS, Fialho AVM, Rodrigues DP. Influências das famílias no cuidado às mulheres climatéricas. Rev. eletrônica enferm. 2013; 15(1):215-22.
26.Leite MT, Taschetto A, Hildebrandt LM, Van der Sand ICP. O homem também fala: o climatério feminino na ótica masculina. Rev. eletrônica enferm. 2013; 15(2):344-51.
27.Araújo IA, Queiroz ABA, Moura MAV, Penna LHG. Social representations of the sexual life of climacteric women assisted at public health services. Texto & contexto enferm. (Online) 2013; 22(1):114-22.
28.Garcia NK, Gonçalves R, Brigagão JIM. Ações de atenção primária dirigidas às mulheres de 45 a 60 anos de idade. Rev. eletrônica enferm. 2013;15(3):713-21.
29.Nascimento RG, Oliveira JSS, Ferreira LS, Santos ZNL, Cardoso RO. Fisioterapia gerontológica na atenção primária à saúde: uma experiência na região norte. Ciência & saúde. 2013; 6(3):222-8.
30.Lim HK, Mackey S. The menopause transition experiences of Chinese Singaporean women: an exploratory qualitative study. J. Nurs .Res. 2012; 20(2):81-90.
31.Kim PS, Coxworth JE, Hawkes K. Increased longevity evolves from grandmothering. Proc Biol Sci. 2012; 279: 4880–4.
32.Doubova SV, Infante-Castañeda C, Martinez-Vega I, Pérez-Cuevas R. Toward healthy aging through empowering self-care during the climacteric stage. Climacteric. 2012; 15(6):563-72.
33.Kalache A. Vested rights, active aging and resiliance: the importance of such concepts throughout life. Rev. bras. geriatr. gerontol.2017; 20(2):159-60.
34.Ciosak SI, Braz E, Costa MFBNA, Nakano NGR, Rodrigues J, Alencar RA et al. Senescence and senility: a new paradigm in Primary Health Care. Rev. Esc. Enferm. USP. 2011; 45(2):1763-68.
35.Aquino DI, Conceição CRFRT, Pereira CRC. A família contemporânea e a estratégia de saúde da família: uma revisão integrativa. Estácio Saúde. 2017; 6(1):48-62.
36.Ferreira ICC, Silva SS, Almeida RS. Menopausa, sinais e sintomas e seus aspectos psicológicos em mulheres sem uso de reposição hormonal. Ensaios Cienc., Cienc. Biol. Agrar. Saúde. 2015; 19(2):60-4.
37.Alves ERP, Costa AM, Bezerra SMMS, Nakano AMS, Cavalcanti AMTS, Dias MD. Climacteric: intensity of symptoms and sexual performance. Texto & contexto enferm. (Online) 2015; 24(1):64-71.
38.Freitas ER, Barbosa AJG. Qualidade de vida e bem-estar psicológico no climatério. Arq. bras. psicol. 2015; 67(3):112-24.
39.Santos AAS, Silva FV, Martins FL. Percepção das mulheres no município de Paulo Afonso, na Bahia, sobre as mudanças corporais e emocionais no período do climatério. Estação Científica (UNIFAP). 2016; 6(1):91-104.
40.Machado MAMP, Aldrighi JM, Ferreira LP. The meanings attributed to the voice by menopause women. Rev. saúde pública. (Online). 2005; 39(2):261-9.