† Except these variables were not questioned during data collection.
ORIGINAL RESEARCH
Assessment of the attributes of primary health care in leprosy control actions
Nayara Figueiredo VieiraI; Fernanda Moura LanzaII; Francisco Carlos Félix LanaIII; José Ramón Martínez-RieraIV
INurse. Master. PhD student of Nursing of the Federal University of Minas
Gerais. Brazil. E-mail: nayarafv5@hotmail.com
IINurse. PhD Adjunct Professor II, Federal University of São João Del Rei.
Brazil. E-mail: fernandalanza@ufsj.edu.br
IIINurse. PhD Full Professor, Federal University of Minas Gerais. Brazil.
E-mail: xicolana@gmail.com
IVNurse. PhD Full Professor, University of Alicante. Spain. E-mail: josera.ferranna@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2018.31925
ABSTRACT
Objective: to evaluate the presence and extent of the attributes of primary health care in leprosy control measures in the view of health professionals. Method: this cross-sectional study involved 251 primary health care personnel in Betim. The Assessment Instrument primary care performance in leprosy control measures was used through interviews, with scores calculated as means of Likert Scale responses. The study was approved by the research ethics committee of Minas Gerais Federal University. Results: strengths (≥6.6) were service orientation to gateway attributes, comprehensiveness of services available and provided, and the family; and weaknesses (<6.6) were access, and orientation towards the community and health professionals. Conclusion: when evaluating the presence and extent of the attributes, the health professionals found deficiencies that impaired the quality of leprosy control measures. Measures to address the endemic must be integrated into primary care in order to eliminate this serious public health problem.
Descriptors: Leprosy; primary health care; health services research; nursing.
INTRODUCTION
Leprosy persists as a public health problem in Brazil due to the high endemicity and the physical disabilities of generated. Strategies such as early diagnosis, multidrug therapy (MDT), prevention of physical disabilities and surveillance of household contacts should be incorporated into health services1.
The Ministry of Health (MOH) recommends as organizational axis of leprosy control actions (LCA) in primary health care (PHC): follow-up of cases and contacts, health promotion through social mobilization and education2, guarantee of comprehensive of care3. As a way to operationalize PHC, Brazil adopted the Family Health Strategy (FHS) aiming to replace the care model, historically based on curative actions and centered on specialists, in line with the principles of the Unified Health System (SUS)3.
In this context FHS, LCA are a priority. Evaluating the performance of services means identifying fragilities, effective and quality health strategies by verifying the attributes of PHC4. Essential attributes include first contact (gateway), continuity or longitudinality of care, comprehensiveness and coordination4. Community guidance, family guidance and cultural competence are also incorporated4. It is opportune to discuss the level of integration and decentralization of LCA in PHC because there are problems such as turnover of professionals, resistance to actions, lack of knowledge about signs and symptoms and reference services and low resolution of PHC5,6. Factors such as prioritization of leprosy in municipal health policies and few training actions contribute to the weakening of decentralization7.
The actions carried out by referral services have been focused on the disease and thus remained distant from the principles of the SUS, keeping the PHC far from being a strategy for the reorientation of the care model. The purpose of this study was to evaluate the presence and extent of attributes of primary health care in the implementation of LCA in the view of professionals who work in the services.
LITERATURE REVIEW
Scientific evidence indicates that health care systems organized based on ordering attributes are effective and of high quality4. The Primary Care Assessment Tool (PCATool - Brazil)8, based on the evaluation of the presence and extent of attributes, has been adopted in Brazil. The instrument specifies structure, process and outcome aspects9. By monitoring trends, the Instrument for Assessment of Performance of Primary Health Care in Leprosy Control Actions (PCAT-leprosy ) is a tool that assesses the degree of guidance provided by PHC in LCA10-12.
The PCAT-leprosy uses essential attributes, namely: access - the way the service is experienced to achieve better results; gateway - implies seeking attention to each new problem; integrality - presupposes the capacity to make arrangements so that the population receives all types of services; continued care - the existence of a regular source of care, which occurs when it is performed by the care is given by the same professional or by the same unit; coordination - availability of information regarding previous problems and services and the recognition of that information4. As for derived attributes: family guidance - when patients are considered within their family context and exposure to health threats; community guidance - when there is an assessment of the patients' needs and recognition of their social context4; and professional guidance - presupposes skills to perform functions, according to the attributes13.
Studies using the PCAT-leprosy demonstrated that problems are related to the derived attributes (community and professional guidance), precisely those that qualify the assistance10,14,15. Despite limited research records in Brazil evaluating the relationship between epidemiological indicators and the quality of PHC, it is verified that the integration of LCA in primary care has the potential to increase access, making it possible to strengthen the actions16.
METHODOLOGY
Evaluative and cross-sectional study. The present study is inserted in evaluative research, because it analyzes the relations of causality between different components of the intervention and allows to understand the outcomes17. The research was carried out in Betim - MG due to its historical and epidemiological importance, because the Santa Izabel Colony was installed there in 1931. From 2002 onwards, there have been investments in the integration of LCA with 90% of the teams trained6. In 2015, the municipality presented a detection rate of 3.11 new cases/100 thousand inhabitants, which characterizes as average endemicity. Operational indicators, contact examination and cure are classified as regular, according to parameters of the MOH18. The coverage of the FHS is around 70%19. At the time of data collection, there were 97 teams, with 90 FHS units and 7 Community Health Agent Strategy (CHAS) units, both models subordinate to the same policy of care to leprosy. Besides PHC, there is the Reference Service for Leprosy of Citrolandia located in Colônia, a pioneer site in the implementation of CT, responsible for conducting training events in the 1980s6.
Data collection took place from February to April 2014, two researchers were trained and prior schedules were performed. We included doctors/nurses who worked in PHC, with the exception of physicians who belonged to the More Physicians Program (MPP) due to their recent inclusion in the work, less than one month prior to the start of data collection. Before the physicians of the MPP were excluded, an interview was conducted and there was a difficulty to understand the language, implying a possible assessment bias. Forty-nine doctors were interviewed. There were 14 exclusions of professionals of the MPP, three refusals and 18 losses due to medical leave, vacations, maternity leave and the impossibility of scheduling. Regarding the nurses, 85 interviews were conducted, with eight losses due to the same reasons above mentioned for the physicians.
The criterion of inclusion of CHAs was to have at least 12 months of experience. This criterion is justified by the fact that acting as an community health agent does not require training in the health area or experience in working with families. When it was not possible to conduct interviews with all CHAs, one agent per team was selected. The CHA interviewed was the one who, at the time of the visit of the researchers, was in the unit and met the inclusion criterion. Thus, 83 interviews were conducted, with 14 losses due to a strike.
The 97 teams are disproportionally distributed in 34 physical units, according to the need of the territory. The criterion of inclusion of managers was to act in PHC services and carry out management activities in the control of leprosy. Thirty-four managers were interviewed, with three losses related to the impossibility of rescheduling.
The PCAT-leprosy in the medical/nursing10, manager11 and CHA12 versions was used and the responses were recorded on a Likert-type scale10-12. The instrument is based on the theoretical framework of PHC3 and in the LCA recommended by the current policy e2. It is noteworthy that the attributeprofessional guidance is not contemplated in the PCATool-Brazil8, but its inclusion was recommended in another study because the SUS offers training13.
The calculation of the score is based on the mean, and on the sum of the items of each attribute divided by the number of items; later this average is transformed into a scale of 0 to 1010-12. Then the mean represents, within each attribute or calculated score, the overall performance of the PHC in the LCA. As overall result of the PCAT-leprosy assessment, there were three measures: essential score - the average of the essential attributes (access, gateway, continued care, coordination and comprehensiveness of services provided and available); derived score - the mean of the derived attributes (family, community and professional guidance); and, overall score - average of the components of the essential and derived attributes, and this characterizes the degree of orientation. Strong orientation was indicated when the mean score was equal to or greater than 6.610-12.
The Pearson chi-square test was used for statistical testing, and the data were analyzed in the IBM SPSS version 19, with a significance level of 5%.
The study was approved by the Research Ethics Committee of the Federal University of Minas Gerais under Opinion nº CAAE 24578213.2.0000.5149 and the participants signed the Informed Consent Term. The study was funded by the Health Surveillance Department (197/2012) and the Foundation for Research Support of the State of Minas Gerais.
RESULTS AND DISCUSSION
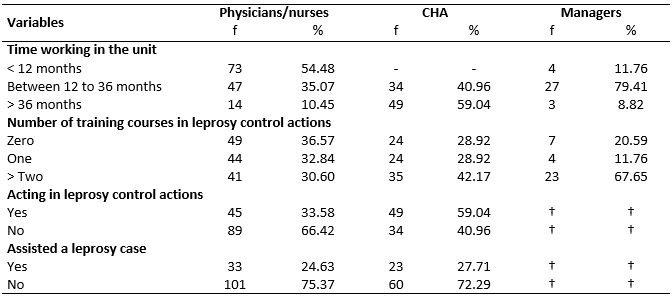
Of the 251 interviewees, 53.4% were physicians/nurses, 33.1% were CHAs and 13.5% managers. Physicians/nurses stood out because of the shorter time working in the unit. Moreover, the majority of the participants had received training in LCA. The majority of the interviewees did not assist leprosy cases. However, CHAs said to perform LCA in the territory, as shown in Table 1.
TABLE 1:
Distribution of professional variables according to the category of the
interviewees. Primary care units. Betim/MG, Brazil, February to April 2014.
† Except these variables were not questioned during data collection.
The overall assessment of the degree of orientation of PHC in the performance of LCA was borderline in the view of physicians/nurses and CHAs (6,7). However, this was not evidenced by the managers (7,3), indicating a distance between what happens in the territory and the planned actions, as shown in Table 2. The absence of a qualified coordination team in LCA at municipal level and political support tends to compromise the integration of actions20. It is necessary to prioritize qualification in the municipal health care policy, as well as commitment on the part of managers7.
TABLE 2:
Mean scores and percentage of high scores (≥ 6.6) of attributes of primary
health care in leprosy control actions according to the interviewees'
experience. Betim/MG, Brazil, February to April 2014.
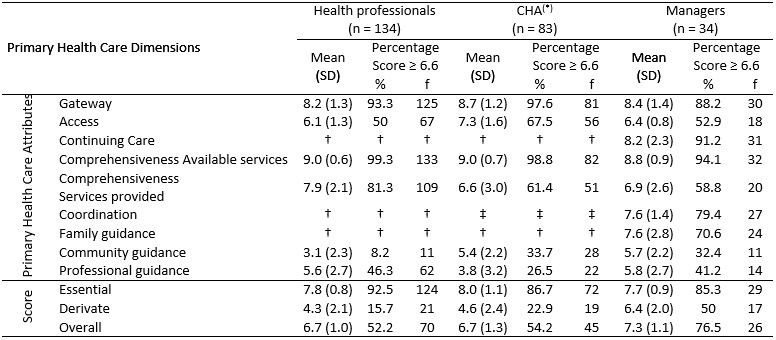
(*)
CHA: Community Health Agent; † Health professionals and community health
agents who had not followed a leprosy case did not respond to the items in
these blocks and due to the number of missing data (> 50%), it was not
possible to calculate the average of these scores; ‡ There are no items in
the performance assessment tool on the attribute coordination in the
Community Health Agent version.
The essential score was very high (≥ 6.6), and gateway and comprehensiveness of the services available and provided contributed the most to this better evaluation. It is recognized that cases of suspected contamination seek the units, but difficult access compromise the effectiveness of PHC as the first place of choice, resulting in the pilgrimage of clients through the network as the disease progresses. Besides PHC, there is the Leprosy Reference Service at Citrolândia, which is also the gateway to suspected cases and treatment.
Comprehensiveness should characterize the procedures and guidelines given in the PHC8. Despite the structural weaknesses, it is undeniable that the expansion of the FHS has promoted advances in health conditions, reduction of maternal and infant mortality, and reduction of infectious and parasitic diseases21,22.
There was fragility in access; only the group of CHAs evaluated it as strongly oriented, being a bottleneck; studies of PCATool- Brazil 8 which evaluated the access to PHC in general and in cases of tuberculosis corroborate this finding. Access barriers are related to delay in consultations and the restricted period of operation of the services 23-25. In Betim, there were weaknesses in relation to the geographic aspect, poor location of the units, precarious pavements, distant microareas, difficulties in public transportation, restriction in the period of operation and overload of the teams. In leprosy, access depends on the knowledge of the population, availability of instruments to perform the dermatoneurological evaluation, and the presence of trained professionals7. The therapeutic itinerary of people with leprosy still reveals the difficulties of PHC professionals to define the suspicion of the signs and symptoms of the disease, whose diagnosis is confirmed only by specialists26.
The experience of monitoring cases improves the evaluation in the overall, essential and derived score. Comparing the proportion of the high score (yes/no) among physicians and nursing professionals and CHAs by presence of case by the Pearson chi-square test, there were significant differences in the comprehensiveness of services provided, community guidance and derived and overall score, as shown in Table 3.
TABLE 3: Mean score, standard deviation, percentage of high score and chi-square
test of the attributes of primary care in leprosy actions, according to the
experience of the interviewees and absence or presence of a leprosy case.
Betim/MG, Brazil, February to April 2014.
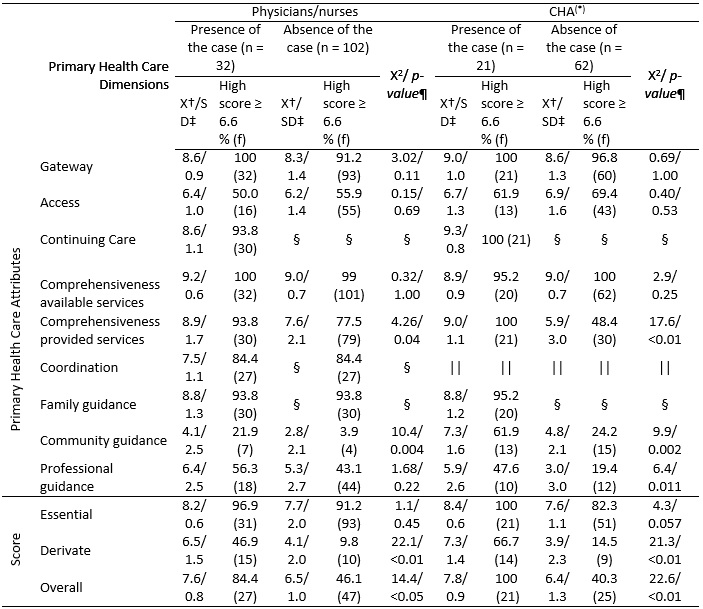
*CHA: Community Health Agent; †Arithmetic mean; ‡SD: standard deviation;
§Health professionals and CHAs who did not follow a case of leprosy did not
respond to the items of these blocks, and it was not possible to calculate
the mean of these scores (missing data > 50%); || There are no items in
the performance assessment tool on the attribute coordination in the
Community Health Agent version; ¶ X2: Qui-square.
Continuing care, family guidance and coordination are calculated for physicians/nurses and CHAs who followed cases; managers, regardless of this criterion, answered the items.
In coordination, physicians/nurses and managers said that PHC is strongly oriented; however, access problems make it difficult to enter the system, where the service is operative. The teams are responsible and maintain coordination when there is a need for attention elsewhere in the network. Strategies can strengthen PHC as the organization of the gateway, construction of protocols in conjunction with multiprofessional teams, facilitating the coordination, adherence to guidelines and an effective referral and counter-referral service16,27,28.
Regarding continuing care, there was a positive evaluation from managers (8.2); physicans/nurses (8.6); CHAs (9.3). This is a reflection of the follow-up of cases; these results should be analyzed with caution and the same observation applies to the family guidance, which was evaluated as strongly guided: physicans/nurses (8.8); managers (7.6) and CHAs (8.8). This suggests a different look for the cases followed in the PHC, in which there is the presence of bond, bringing the team closer to the family context.
A study with the PCAT-leprosy tool in Teófilo Otoni- MG pointed out that, in the view of the managers, there is poor guidance in continuous care10. In this municipality, users have the reference as a source of care, which may justify the low guidance. In Betim, the results were different, possibly reflecting the integration of actions. Tactics such as the user being assisted by the same professional at each supervised dose, search for information about adherence to treatment, and general guidelines can strengthen the continued care.
The strong family guidance shows concern with context, understanding that relationships and conflicts directly influence health. Studies that evaluated the family approach in PHC demonstrated little incorporation of families in the practices and insufficient interest on the part of professionals to know the life conditions of the patients29,30. In leprosy, families must be inserted in the therapeutic process because the family nucleus represents the group of people at risk of contamination. The items are related to knowledge about the family, suspicion of new cases, examination of contacts, self-care guidelines and the appearance of complications recognized by relatives10. Families should understand the health-disease process and the drug therapy and facilitate the adherence to treatment. The familiarization with the life and health conditions of the populations allows the understanding of their needs that go beyond curative practices6,31.
The comprehensiveness of the services provided refers to the items that identify subjects approached by the professionals during consultations8. In the PCAT - leprosy, the actions advocated by the MOH such as monitoring suspected cases, diagnosis, general guidelines, supervised dose administration and evaluation of contacts2.
There was poor community guidance in PHC, as well as to significant differences in the presence of cases. The weaknesses are related to the unavailability of educational material and lack of active search. Moreover, more than 60% of the physicians/nurses reported not performing actions in the territory. Research carried out with health advisors and community leaders in an endemic municipality of Minas Gerais showed absence of social participation in the control of leprosy and fragility in health education strategies used by PHC professionals who are not capable of provoking spontaneous demand of the population to perform diagnostic actions for suspected cases32.
Studies of PCATool - Brazil8 also obtained unsatisfactory scores in community guidance according to the general view of users of PHC and caregivers of children24,25,33,34. As for studies with PCAT - leprosy, there was also weak community guidance in three municipalities of Minas Gerais10. These evidences corroborate the results. Thus, incorporating strategies such as reviewing the work process, encouraging user participation, and conducting home visits would facilitate health surveillance and community monitoring24,35.
In professional guidance, there was weak guidance in LCA and statistical differences in the proportion per case assisted by CHA. The majority of the participants reported training, suggesting little effectiveness, and it was necessary to evaluate methodologies and periodicity. Scientific evidence indicates that training increases detection, makes professionals responsible for the epidemiological situation and stimulates disease control actions36.The challenge is to overcome the insecurity of professionals in carrying out the diagnosis and treatment. Thus, qualification has the potential to modify an epidemiological situation.
CONCLUSION
The strong guidance of the service in the attributes gateway, comprehensiveness of services available and provided, family guidance; and the weaknesses in access and community and professional guidance demonstrate that it is necessary to strengthen the decentralization policy. It is important to value the care model based on health surveillance and identification of needs of the population. This study can support future research regarding the effectiveness of the offered training, because despite training, the teams feel unprepared.
However, when assessing the presence and extent of primary care attributes in LCA, the professionals found deficiencies that impair the quality of the service. It is necessary to integrate the actions of control of the endemicity to eliminate this serious public health problem, mainly in regions as Betim, scenario of a former colony.
The limitations of this study are the strike of CHAs that occurred during the research, the recent inclusion of physicians/nurses in the PHC service and the difficult schedule of the participants. There was a possible bias of intention on the part of managers, because they were evaluating the services that they coordinate.
REFERENCES
1. World health organization. Global leprosy: update on the 2013 situation. 26th. Geneva (Swi): Weekly Epidemiological Record; 2014.
2. Ministry of Health (Br). Ordinance No. 149, of February 3, 2016 (BR). Approves the Guidelines for Surveillance, Attention and Elimination of Leprosy as a Public Health Problem, in order to guide the managers and professionals of the health services. Brasília (DF): Ministerial Cabinet, 2016.
3. Ministry of Health (Br). National Policy of Primary Care. Brasília (DF): Ministry of Health; 2012.
4. Starfield B. Primary care: balancing health needs, services and technology. Brasília (DF): Unesco; 2002.
5. Mendes MS, Trindade LC, Cantídio MM, Aquino JAP, Campos GP, Zamora A, Barbosa JC, Heukelbach J. Decentralization of leprosy control actions in João Pessoa (Paraíba): the managers' view. Cad. saúde colet. 2008; 16(2): 217-30.
6. Fuzikawa PL, Acúrcio FA, Velema JP, Cherchiglia ML. Decentralisation of leprosy control activities in the municipality of Betim, Minas Gerais State, Brazil. Lepr. rev. 2010; 81 (3): 184-95.
7. Lanza FM, Lana FCF. Decentralization of leprosy control actions in the micro-region of Almenara, State of Minas Gerais. Rev. latinoam. enferm. (Online). 2011; 19(1): 187-94.
8. Ministry of Health (Br). Manual of the instrument for evaluating primary health care: Primary Care Assessment Tool PCAtool- Brazil. Brasília (DF): Ministry of Health; 2010.
9. Donabedian A. Evaluating the quality of medical care. The Milbank Quarterly. 2005; 83(4): 691-729.
10. Lanza FM. Evaluation of primary care in leprosy control: instrument validation and performance analysis of endemic municipalities of the State of Minas Gerais [doctoral dissertation]. Belo Horizonte (MG): Federal University of Minas Gerais; 2014.
11. Lanza FM, Vieira NF, Oliveira MMC, Lana FCF. Evaluation of leprosy control actions developed in primary care: a proposed tool for managers. REME rev. min. enferm. 2014; 18(3): 606-13.
12. Lanza FM, Vieira NF, Oliveira MMC, Lana FCF. Instrument for evaluation of leprosy control actions in primary care. Rev. bras. enferm. (Online). 2014; 67(3): 339-46.
13. Pan American Health Organization. Validation of a methodology for the rapid assessment of organizational characteristics and performance of primary health care services of the Unified Health System (SUS) at local level. Brasília (DF): Ministry of Health; 2006.
14. Vieira NF. Evaluation of primary health care in leprosy control actions in the city of Betim, Minas Gerais [master's thesis]. Belo Horizonte (MG): Federal University of Minas Gerais; 2015.
15. Sousa GS, Silva RLF, Xavier MB. Attributes of primary health care in leprosy control: nurse's perspective. Rev. baiana enferm. 2017; 31(1): 1-10.
16. Saltarelli RMF, Seixas DH. Limits and possibilities in the care of leprosy patients within the family health strategy. Rev. APS. 2016; 19(4): 613- 22.
17. Brousselle A, Champagne F, Contandriopoulos AP, Hartz, Z. Evaluation concepts and methods. Rio de Janeiro: Editor Fio Cruz; 2011.
18. Ministry of Health (Br). [Internet site] Strategic Management Support Room. [cited 2017 Dec 12] Available from: http://sage.saude.gov.br/
19. Ministry of Health (Br). [Internet site] Strategic Management Support Room. [cited 2017 Dec 12] Available from: http://dab.saude.gov.br/portaldab/
20. Ramos- JR NA, Heukelbach J., Hinders DC, Gomide M, Schreuder PAM. Investigations in health service systems as a tool to reach more effective Leprosy Control Programs in Brazil. Cad. Saúde Pública (Online). 2008; 16(2):147-68.
21. Victora CG, Aquino EML, Leal MC, Monteiro CA, Barros FC, Szwarcwald CL. Health of mothers and children in Brazil: progress and challenges. J. Lancet. 2011; 6736(11): 32-46.
22. Barreto ML, Teixeira MG, Bastos FI, Ximenes RAA, Barata RB, Rodrigues LC. Successes and failures in the control of infectious diseases in Brazil: the social and environmental context, policies, interventions and research needs. J. Lancet. 2011; 6736 (11): 47-60.
23. Arakawa T, Arcêncio RA, Scatolin BE, Scatena LM, Ruffino-Netto A, Villa TC. Accessibility to tuberculosis treatment: assessment of health service performance. Rev. latinoam. enferm. (Online). 2011; 19(4): 994-1002.
24. Pereira MJB, Abrahão-Curvo P, Fortuna CN, Coutinho SS, Queluz MC, Campos LVO et al. Evaluation the organizational and performance characteristics of a unit of Primary Health Care. Rev. gaúch. enferm. 2011; 32(1): 48-55.
25. Mesquita M Filho, Luz BSR, Araújo CS. Primary health care and its attributes: the situation of children under two years old according to their caregivers. Ciênc. Collective health (Online). 2014; 19 (7): 2033-46.
26. Aquino CMF, Rocha EPAA, Guerra MCG, Coriolano MWL, Vasconcelos EMR, Alencar EN. Pilgrimage (Via Crucis) to the diagnosis of leprosy. Rev. enferm. UERJ. 2015; 23(2):185-90.
27. Almeida PF, Fausto MCR, Giovanella L. Strengthening primary health care: a strategy to enhance coordination of care. Rev. panam. salud pública. 2011; 29(2): 84-95.
28. Giovanella L, Mendonça MHM, Almeida PF, Escorel S, Senna MCM, Fausto MCR et al. Family health: limits and possibilities for a comprehensive approach to primary health care in Brazil. Ciênc. saúde coletiva (Online). 2009; 14(3):783-94.
29. Alencar MN, Coimbra LC, Morais APP, Silva AAM, Pinheiro SRA, Queiroz RCS. Evaluation of family focus and community guidance in family health strategy. Ciênc. saúde coletiva (Online). 2014; 19(2): 353-64.
30. Silva NC, Giovanella L, Mainbourg EMT. The family in the practices of family health teams. Rev. bras. enferm. (Online). 2014; 67(2): 274-81.
31. Oliveira MAC, Pereira IC. Essential attributes of primary care and family health strategy. Rev. bras. enferm. (Online). 2013; 66(esp): 158-64.
32. Lopes FN, Lana FCF. Popular participation in the control of leprosy: a challenge for the health services. Rev. enferm. UERJ. 2015; 23(2):235-40.
33. Castro RCL, Knauth DR, Harzheim E, Hauser L, Duncan BB. Evaluation of the quality of primary care by health professionals: comparison between different types of services. Cad. Saúde Pública (Online). 2012; 28(9): 1772-84.
34. Sala A. Luppi CG, Marsiglia OSR. Comprehensiveness and primary health care: evaluation from the perspective of users of health units in the city of São Paulo. Saúde Soc. 2011; 20(4): 948-60.
35. Leão CDA, Caldeira AP, Oliveira MMC. Attributes of primary care in child health care: assessment of caregivers. Rev. bras. saúde matern. infant. 2011; 11(3): 323-34.
36. Moreno CMC, Enders BC, Simpson CA. Evaluation of leprosy skills: opinion of physicians and nurses of family health teams. Rev. bras. enferm. (Online). 2008; 61(esp): 671-5.