ORIGINAL RESEARCH
Health service performance in tuberculosis care in the Family Health Strategy
Keidi Vianna BenettiI, Sheila Nascimento Pereira de FariasII, Maria Helena do Nascimento SouzaIII, Maria Yvonne Chaves MauroIV, Célia Regina da Silva MedeirosV, Pedro Miguel Diniz ParreiraVI
I
Nurse. Master degree. Federal University of Rio de Janeiro. Brazil.
E-mail: keidi.b@globo.com
II
Nurse. Ph.D. Assistant Professor, Federal University of Rio de Janeiro.
Brazil. E-mail: sheilaguadagnini@gmail.com
III
Nurse. Ph.D. Professor, Federal University of Rio de Janeiro. Brazil.
Email: mhnsouza@yahoo.com.br
IV
Nurse. Ph.D. Professor, University of Rio de Janeiro State. Brazil. Email: mycmauro@uol.com.br
V
Nurse. Master degree. Ph.D. student, Federal University of Rio de Janeiro.
Brazil. E-mail: celiamedeiros@globo.com
VI
Ph.D. Professor of the Nursing School at the University of Coimbra
-Portugal. Email:
pedromiguel.parreira@gmail.com
DOI: https://doi.org/10.12957/reuerj.2018.31643
ABSTRACT
Objective: to evaluate health service performance in tuberculosis care as perceived by family health strategy teams. Methods: in this quantitative, cross-sectional study, the PCATool-tuberculosis was applied between August and November 2015, to 210 professionals from family health strategy teams in a planning area in Rio de Janeiro. Data were processed and analyzed using Epi Info software, version 7.1.5. The project was approved by the research ethics committees of the Anna Nery School of Nursing and Municipal Health Secretariat. Results: the units' performance was observed to be reasonable in tuberculosis diagnosis, and satisfactory in treatment. Conclusion: health service performance displays weaknesses and meets client needs partially.
Descriptors: Nursing; Tuberculosis; Health management; Family Health.
INTRODUCTION
Tuberculosis (TB) still remains a major public health problem. Its relevance and magnitude could now be evidenced by the estimates of the Ministry of Health, which indicates 70,000 new cases of tuberculosis and 4.6 million deaths per year¹. Brazil occupies the 17th place among the 22 countries responsible for 80% of the total tuberculosis cases in the world2.
However, in the last 17 years, tuberculosis had a 38.7% drop in the incidence rate and 33.6% in the mortality rate. The downward trend in both indicators is accelerating year after year in a national effort, coordinated by the ministry, which may determine the effective control of tuberculosis in the near future, when the disease may no longer be a public health problem2.
Primary health care (PHC), in particular, the Family Health Strategy (FHS), is now considered to be the main gateway for patients with TB. The partnership with PHC to integrate health surveillance actions should be stimulated and prioritized by local TB Control Programs3.
The ESF is an alternative for the reorganization of the provision of health services and the proposal is part of the debate about the options for reorientation of the current care model, predominantly hospital-centered and curative. The main change with the ESF proposal is the focus of attention, which is no longer exclusively focused on the individual and the disease, but also on the collective, and the family is the privileged space for action. This implies learning to deal with this new clipping, now taking the family as an object of work, identifying tools and knowledge that can transform care practice towards a practice based on ethical and moral principles and leading to greater autonomy of patients.
In the context of the health model proposed by the ESF, the management of health services should be taken as an instrument that can enable the sharing of power within health units and teams and, in this sense, may constitute an important tool in the implementation of policies3.
In this perspective, the manager has a fundamental role in favoring the access of patients with TB to PHC, since he has a prominent role in the health unit to manage, supervise and mediate the care with these patients.
Thus, if the manager performs his/her role of managing, monitoring cases and supervising the teams in relation to the patient with signs/symptoms of TB, the unit will be more efficient in carrying out active search and diagnosis of new cases.
The objective of the study was to evaluate the performance of health services in tuberculosis care, in the perception of the ESF teams.
LITERATURE REVIEW
The greater the number of basic health units and trained professionals developing TB control actions, the more effective the search and detection of cases. Moreover, the speed at the beginning of treatment and its supervision favors healing and the breakdown of the transmission chain4.
Historically, health services have not shown satisfactory, timely and resolute results to the growing demands and needs of the population. Adherence to treatment, the patient's commitment to treatment, and consequently the regularity of medication will depend in large part on how the patient is treated in the health service4.
It is necessary to invest in the qualification of health services, in the training of human resources for surveillance, evaluation and control activities to increase the diagnostic capacity through bacilloscopy, promote healing, intensify the search for respiratory symptomatology and patient contacts, in the Brazilian municipalities and especially in the priority municipalities for the National Tuberculosis Control Program5.
This program favors the decentralization of control measures for basic care, as well as increasing the access of the population in general and the populations most vulnerable to tuberculosis. It can be emphasized that one of the basic conditions for successful treatment of TB is easy access of the patient to the health service. This decentralization implies the recognition of primary care as a protagonist in the organization of the health care system through the attribution and organization of organizational and material mechanisms that can guarantee the longitudinal of care6.
The access to health services understood as the gateway is the place of acceptance of the patient at the time of expressing their need. From this perspective, access goes beyond the pure and simple connection to the concept of the door of entry, configured as a transforming device of reality7.
However, it is recommended that tuberculosis control programs, rather than reducing the patient´s time to seek diagnosis and maximize treatment initiation, should be user-friendly and participatory. Thus, ESF professionals must actively listen to the complaints of the patients, adjusting care and proposing solutions together (health team and patient), establishing a relationship based on the host and the link8.
METHODOLOGY
This is a cross-sectional study with a quantitative approach, carried out in a planning area of the Municipality of Rio de Janeiro in 2015. The study was carried out by 210 professionals from five health clinic units of the family, who accepted to participate in the study.
These units were chosen because they had a high number of people diagnosed with tuberculosis, according to DATASUS data. The professionals who constituted the health teams of both genders, employees of the family clinics of program area 3.1 of the Municipality of Rio de Janeiro participated. For the data collection, a presentation of the thematic in the clinics was first made, for the health professionals. Then, a schedule was set for the application of the questionnaire, which occurred in the initial period of the team meetings in the family clinics. The respondent answered each item according to a Likert Scale from zero to five. The value zero was assigned to answer I do not know or does not apply; the values from 1 to 5 record the degree of preference relation of the statements. The lowest score (score 1) represents a bad indicator, that is, it refers to the idea that access never happens. The highest value score (score 5) represents a positive indicator since it conceives the idea that it is always accessible to the patient. The population of this study consisted of 43 nurses, 43 doctors, 43 nursing technicians and 258 community health agents, with a total of 387 professionals from the ESF, who form the staff of the program area.
Regarding the sample of health professionals, of the total of 387, simple sampling was performed; using a random equation the following equation9:
n= 000N.Z².p.(1-p)000
00Z².p.(1-p)+ e².(N-1)
The simple random sample was: n = calculated sample; N = Population; Z = standardized normal variable associated with the confidence level; p = true event probability; e = Sample error.
A sample error of 5% and 95% confidence level were considered. The minimum sample calculated was 194 professionals of the health teams of A.P.3.1, defining 210 subjects. To evaluate the performance of the health units, the Primary Care Assessment Tool-tuberculosis questionnaire, represented by the dimension of access to diagnosis and access to treatment was used. The indicators were analyzed individually and also by health unit. A composite index was determined for each group (access to diagnosis and treatment) by summing the answers of all professionals interviewed in each group and divided by the total number of respondents. This index will represent the performance of each group.
Among the independent variables analyzed regarding access to the diagnosis of tuberculosis, the following stand out: the time it takes to get a consultation; if patients go to the health facility closest to their home; more than 60 minutes to be assisted; if some motorized means of transportation must be used to move to the unit; lose the work shift and get information over the phone. For the variables related to the access of the treatment stands out: if they can get consultation in 24 hours; if the professional accompanying the treatment makes home visits; if they lose their work shift; if they have difficulty moving to the unit; if they need motorized transportation; if there was a lack of medication in the last 12 months and more than 60 minutes are expected to be assisted, among others.
The performance of services in TB care was classified according to the values obtained from the indicators. The values of 1 and 2.49 were classified as unsatisfactory performance, close to 2.50 to 3.49, regular and greater than 3.49, satisfactory.
The study project was approved by the Research Ethics Committee of the Anna Nery School of Nursing/Federal University of Rio de Janeiro, approval protocol 1,035,492/2015 and also by the Municipal Health Secretary of Rio de Janeiro, protocol nº 1.141.398/2015, to comply with Resolution 466/12 of the National Health Council, observing the ethical principles of the research, with application of the Term of Free and Informed Consent in all participants.
RESULTS
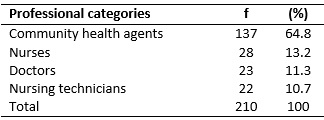
It was identified that 137 of the 210 participants in the survey (64.8%) were community health agents and 28 (13.2%) were nurses. See Table 1.
TABLE 1:
Professional categories of respondents. Rio de Janeiro, 2015.
It is observed that 135 (64.4%) of the respondents answered that patients are always looking for the nearest unit to diagnose TB. There were 93 (44.4%) of them that said patients never expected more than 60 minutes to be served; 66 (32.2%) revealed that patients can never obtain information over the telephone; 88 (40.2%) never have difficulty moving; 90 (42.9%) never have to use some means of motorized transportation and 78 (36.9%) revealed that patients sometimes lose their work shift due to the consultation in the unit. See Table 2.
TABLE 2: Distribution of the variables of access to the diagnosis of tuberculosis,
according to the professionals interviewed of A.P. 3.1 of the Municipality
of Rio de Janeiro, 2015 
The patient´s access to the diagnosis of TB was evaluated by the professionals of the ESF teams as reasonable, obtaining an average of 3.32 and a standard deviation of 1.35. When the average score is applied, this result is between 2.50 and 3.50 and then it is classified as regular. See Table 3.
TABLE 3: Variables referring to the access of patients to the
diagnosis of tuberculosis, according to the health team of the family
interviewed in the program area of the Municipality of Rio de Janeiro,
2015.

(*) Average according to the likert scale: always, often, sometimes, hardly
ever and never.
(**) Score for the classification of the results: <2.50 -
Unsatisfactory; From 2.50 to 3.49 - Average; and> 3.49 - Satisfactory.
SD-Standard Deviation
It should be noted that only the health unit C had the access classified as satisfactory. The other units participating in the research obtained the average concept.
The results indicate that the variables evaluated as unsatisfactory for the access of the patient with TB were - difficulty in obtaining information and difficulty in make consultations by telephone. On the other hand, the following variables reached the regular concept: difficulty of moving, use and expense with means of transportation and loss of work shift. Finally, the variables - looking for the nearest unit and waiting more than 60 minutes - were evaluated as satisfactory.
DISCUSSION
It is widely known that distance-related barriers are associated with the level of complexity of THE services: the less specialized they are, the closer they are to the population, and the reverse is true. In this sense, another study identifies that the access was not criticized by the patients, but the reports pointed out that the distance was short and they could walk home from the ESF10.
The results of this research converge to another study, whose professionals emphasize the patients´ preference for care closer to their homes 11.
Some authors reveal that one of the great indicators of abandonment of TB patient adherence to the Tuberculosis Control Program is the waiting time for consultations in PHC12.
Telephone communication can be a very attractive means for patients with signs and symptoms of TB to improve their access to the health unit. Some interviewees reported that there is a telephone in the administration of the clinic, only that the employees do not have information about the disease and cannot explain how the care is performed.
In England, there is a telephone answering program where people call and nurses give information about the problem revealed. The population seeks care in case of emergency or in the appearance of various signs and symptoms and are welcomed by professionals who solve their problems 12.
A study done in Itaboraí/RJ reported that on average, the patients often use motorized transportation to go to the health unit13, diverging from the findings in this study.
The accessibility to the health service must be valued for the diagnosis to be made and treatment efficacy. Studies have reported that patients who use public transportation and who have transportation costs tend not to go to the ESF or abandon treatment once started, more frequently than those who use their own means8,12,13.
It is important that patients with signs and symptoms of TB receive the necessary guidance, from the health unit search by telephone. There is a need for ESFs to use strategies that train the staff to guide the patients in the first contacts. It is necessary to make it clear to the patients that all doubts will be solved to help them and they should seek the health services whenever necessary. The ESF brings the expansion of access to health services as a philosophy, being strategically located in areas where the family grant program exists, which is a mechanism of social protection and favors the approximation of the patient to health units14.
There is a tendency of health professionals to point out that the patient is responsible for the success of adherence or abandonment of treatment. However, team members should be constantly evaluating the results of their actions, identifying strengths and difficulties found in the service. It is necessary that all those involved find ways to contribute to the efficiency and effectiveness of disease control, effectively motivating adherence to treatment15.
CONCLUSION
In this study, regarding the performance of the health services of the ESF, the access to the diagnosis for tuberculosis was considered average, which requires improvements. The access to tuberculosis treatment was satisfactory.
The limitations of the study on the small number of health units participating are acknowledged, which does not make it less relevant since it gives visibility to the social problem of TB in Rio de Janeiro.
It is necessary to improve the reception of individuals with TB who seek ESF to ensure a positive impact on the control, treatment, and prevention of this disease in the population. The diagnosis of the disease is essential for the control of this important endemic that still persists in these days. The faster the health units make this diagnosis, the sooner the patient will start treatment and the chances of spreading the disease decrease.
The studies that still need to be carried out for TB control, including research on the self-assessment of professionals working in this area, especially the professionals of the ESF, are not exhaustive.
REFERENCES
1. Ministry of Health (Br). Secretary of Health Care. Department of Primary Care. History of family health coverage. [Internet] 2016 [cited in 2017 Jun 01]. Available from: http://dab.saude.gov.br/portaldab/historico_cobertura_sf.php
2.Ministry of Health (Br). Health Portal: Tuberculosis. [Internet] 2015 [cited in 2017 Jun 01] Available from: http://portalsaude.saude.gov.br/index.php?option=com_content&view=article&id=11045&Itemid=674
3.Ministry of Health (Br). Department of Health Surveillance. Directly observed treatment (DOT) of tuberculosis in primary care: nursing protocol. [Internet] 2014 [cited in 2017 Dec 15]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/tratamento_diretamente_observado_tuberculose.pdf
4.Ministry of Health (Br). Department of Health Care. Health Surveillance: Dengue, Schistosomiasis, Leprosy, Malaria, Trachoma, and Tuberculosis. 2ª ed. Brasília (DF): Publishing MS; 2008.
5.Ministry of Health (Br). Executive Secretary. Datasus. Health information. Epidemiological information and morbidity. [Internet] 2014 [cited in 2017 Aug 15]. Available from: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?idb2011/c17.def
6.Clementino F, Miranda F. Tuberculosis: reception and information from the perspective of the domiciliary visit. Rev. enferm. UERJ [Online]. 2015 [cited in 2017 Jul 01]; 23(3):350-4. Doi: https://doi.org/10.12957/reuerj.2015.4289
7.Loureiro RB, Villa TCS, Netto AR, Peres RL, Braga JU, Zandonade E, Maciel ELN. Access to the diagnosis of tuberculosis in health services in the city of Vitória, ES, Brazil. Ciênc. saúde coletiva[Online]. 2014 [cited in 2017 Aug 15]; 19(4):1233-44. Doi: http://dx.doi.org/10.1590/1413-81232014194.01002013
8.Andrade S, Rodrigues D, Barreto A, Oliveira A., Santos A & Sá L. Tuberculosis in the Elderly: the gateway to the health system and the late diagnosis. Rev. enferm. UERJ [Online]. 2015 [cited in 2017 Sep 17]; 24(3):e5702. Doi: https://doi.org/10.12957/reuerj.2016.5702
9.Medronho RA, Carvalho DM, Bloch KV, Luiz RR, Werneck GL. Epidemiology. São Paulo: Atheneu; 2006.
10.Azevedo ALM, Costa AM. The narrow entrance door of Brazil's National Health System (SUS): an evaluation of accessibility in the Family Health Strategy. Interface - Comunic Saude Educ [Online]. 2010; 14(35):797-810. Doi: http://dx.doi.org/10.1590/S1414-32832010005000029
11.Villa TCS, Netto AR. Performance assessment questionnaire regarding TB control for use in primary health care clinics in Brazil. J. bras. Pneumol [Online]. 2009 [cited in 2017 Jun 01]; 35(6): 610-2. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1806-37132009000600014&lng=en . Doi: http://dx.doi.org/10.1590/S1806-37132009000600014
12.Orfão NH, Andrade RLP, Beraldo AA, Brunello MEF, Scatena LM, Villa TCS. Adherence therapeutic to the treatment of tuberculosis in a municipality of the São Paulo state. Ciênc. Cuid. Saúde [Online]. 2015 [cited in 2017 Aug 15]; 14(4):1453-61. Doi: http://dx.doi.org/10.4025/cienccuidsaude.v14i4.25093
13.Lafaiete RS, Silva CB, Oliveira MG, Motta MCS, Villa TCS. Research on access to tuberculosis treatment in Itaboraí /RJ. Esc. Anna Nery Rev. Enferm [Online] 2011 [cited in 2017 Jun 01]; 15(1):47-53. Doi: http://dx.doi.org/10.1590/S1414-81452011000100007
14.World Health Organization. Global Tuberculosis Report 2017 [Internet]. Geneva (Swi): World Health Organization; 2017 [cited in 2017 Nov 09]. Available from: http://apps.who.int/iris/bitstream/10665/191102/1/9789241565059_eng.pdf
15.Costa AG, Rodrigues ILA, Garcia WMB, Nogueira LMV. Monitoring of actions for the prevention and control of tuberculosis in basic health units. Rev enferm UFPE on line 2016; 10 (Supl. 3): 1378-86. DOI: 10.5205/reuol.7057-60979-3-SM-1.1003sup201605