ORIGINAL RESEARCH
Illness among nursing workers in the hospital context
Ana Terra Porciúncula BaptistaI, Norma Valéria Dantas de Oliveira SouzaII, Cristiane Helena GallaschIII, Thereza Christina Mó Y Mó Loureiro VarellaIV, Isabela da Rosa NoronhaV, Isabele da Rosa NoronhaVI
I
Nurse. Resident in Neonatal Nursing at Instituto Fernandes Figueira
(IFF/FIOCRUZ). Rio de janeiro Brazil. Brazil. E-mail: anaterrapb@gmail.com
II
Nurse. PhD in Nursing. Professor at the State University of Rio de Janeiro,
Brazil. E-mail: norval_souza@yahoo.com.br
III
Nurse. PhD in Nursing. Professor at the State University of Rio de Janeiro,
Brazil. E-mail:
cristiane.gallasch@gmail.com
IV
Nurse. PhD in Nursing. Professor at the State University of Rio de Janeiro,
Brazil. E-mail: thereza1208@gmail.com
V
Nursing student. Faculty of Nursing, State University of Rio de Janeiro,
Brazil. E-mail: isabela.rosa_@hotmail.com
VI
Nursing student. Faculty of Nursing, State University of Rio de Janeiro,
Brazil. E-mail: isabele-rosa@hotmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2018.31170
ABSTRACT
Objective: to determine the health problems that lead nursing professionals to leave work for more than 15 days or to undergo functional readjustment. Methods: in this quantitative, retrospective, documentary study, 886 records of absence of the nursing staff at an university hospital were examined. Data were presented using descriptive statistics. Results: workers' absences were attributed mainly to mental and behavioral disorders (22.6%), followed by musculoskeletal system and connective tissue diseases (24.4%). The main causes that led nursing staff to undergo functional rehabilitation, were musculoskeletal diseases (56.3%), followed by mental disorders (18.8%). Conclusion: nursing workers display high rates of illness from musculoskeletal diseases; however, growing mental illness is worrisome. Therefore, it is necessary to intensify protective measures to prevent illness and improve working conditions.
Descriptors: Nursing; occupational Health; sick leave; employment, supported.
INTRODUCTION
During the 1990s, university hospitals (UH) were incorporated into the Unified Health System (SUS). Aiming to make the process less costly and adjusted to the political direction of the State Reform of the Federal Government, an adjustment was made in the work force of those institutions that adhered to the Multiple Juridical Regime (RJM in Portuguese). This change allowed for different forms of occupational relationships, bringing flexibility to labor relations and the lack of public tenders1.
The precariousness of labor relations, derived from the neoliberal model, is based on precepts that directly influence the world of work: workers have precarious employment relationships, losing stability in their jobs and labor rights. In addition, they work long hours and receive ignominious remunerations. So, to keep themselves in minimum subsistence conditions, they expose themselves to double and even triple shifts of work2.
These issues adversely reflect the worker's health, provoking manifestations, such as stress, tachycardia, systemic arterial hypertension, drowsiness, sweating, physical and mental exhaustion, depression, fatigue, headache, epigastric pain and irritability3. These manifestations compromise the care provided to the patients and the quality of life of the professionals4.
Conditions inherent in nursing work, such as coping with suffering and experiencing the process of death and dying5, are added to the high demand in work, rigid supervision on the activities performed, low salaries and the reduced social recognition that the profession holds in the national scenario6. Such conditions increase the worker's vulnerability to illness and, consequently, the need to take leave of absence.
In this perspective, the present study has as object of study the reasons that lead nursing workers to take leave from their job functions or undergo functional re-adaptation. A study carried out with 1,509 nursing professionals revealed that 20.3% of leaves of absence was due to the illness of these workers7. It is added that the leave negatively influences workers' perception of their quality of life and health8, demonstrating the central role that work still plays in the individual's life.
The leave of absence also has a negative impact on the care provided to the user, as it results in less professionals to set in motion the work process, overloading the other members of the nursing team who remain in the care, and it is necessary to carry out management measures to substitute that employee, such as the relocation of professionals and/or the hiring of a substitute employee9. However, even if the professional in sick leave is replaced, there is a loss in the quality of the assistance, since it takes time for the substitute professional to reach the same level of productivity of the former employee.
Granting a leave for these workers from their general functions, therefore, triggers suffering for the worker himself and precariousness of care. Therefore, considering the initial contextualization, the present study aimed to determine the health issues that lead nursing professionals to leave work for more than 15 days or to undergo functional re-adjustment.
LITERATURE REVIEW
Health work can be performed within any of the levels of care: primary, secondary and tertiary10. However, the hospital remains the great employer of nursing professionals, a complex environment due to the multiplicity of actors involved in the planning and execution of actions11.
Among situations triggering psychophysical suffering and sickness of nursing workers in hospitals, we can mention the relationship between the nursing team and patient-family members, the intense rhythm of work and the need to maintain attention and concentration to avoid iatrogenias12,13, a work process marked by exposure to ergonomic, biological, chemical and physical occupational hazards. Due to its specificity, this complex work encompasses situations that can deplete workers' health.
Added to this, there has been an even more adverse context for these workers because of the new configurations of the world of work, influenced by the neoliberal precepts14. It is known that work is never neutral in the health-worker process15. These stressful situations trigger processes of physical and psychic somatization and/or emotional disorders that result in signs of distress, lack of motivation, fear, pathological anxiety and depression16.
As protection measures, we seek the use of personal protective equipment, permanent education in service, as well as adequate machinery and materials17, in addition to preventing workers from being exposed to stress, if unavoidable, reducing the impact thereof16.
In spite of these strategies, the high scientific production in the field of occupational health that demonstrates the causal link between the work process and the disease process, health promotion and protection actions implemented by the force of law and the institution of assistance models that are seeking a recovery of the workforce, we have found that professionals have been increasingly sick, discouraged and with degrading salaries. This has a direct impact on the quality of life and can lead to high evasion from the profession, high percentage of sickness, presenteism, early retirement and even death of workers.
METHODOLOGY
This is a retrospective, documental, quantitative study conducted in a large university hospital located in the city of Rio de Janeiro, which was operating, during the study period, below its full capacity, with approximately 235 beds.
This is a study of the census type, that is, with counting and rational organization of information, that is, analysis of all elements of a given population18. In this study, the population was defined as all the nursing professionals that worked in the referred hospital, in the statutory regime, between January and December 2015, which in this period corresponded to 324 nurses and 1,078 nursing technicians, totaling 1,402 professionals.
We analyzed 886 records available in the health care system of these workers, in the Department of Occupational Safety and Health, and selected data referring to leaves longer than 15 days and/or functional re-adaptation, forming a sample of 380 professionals. The period of absence was defined as being greater than 15 days because, at the institution, starting from the 16th day of leave, the worker is referred to the National Institute of Social Security, when in a Consolidated Labor Laws (CLT) regime.
For data collection, a form developed by the team of researchers, which contained the following variables: age, sex, professional category, type of employment relationship, place of employment, reasons for absence, leave length, start and end date of the leave, benefit granted/outcome of the situation – sick leave, retirement due to disability, death or functional readjustment.
The data collected were coded and tabulated in a spreadsheet in Microsoft Excel®2013 software. The analysis was performed through descriptive statistics with conversion to absolute and relative frequencies for the categorical variables.
The study complied with the ethical requirements contained in the national and international norms regulating research involving human beings and was approved by the research ethics committee under protocol no. 1,690,589 on August 23, 2016.
RESULTS
Most of the removed professionals in the period studied belonged to the female sex (91.3%), were between 46 and 55 years old (42.1%) and worked in the institution as a nursing technician (76.5%). It should be noted that the participants were counted according to professional ties, that is, an individual who had more than one registration in the hospital was counted twice, since it is understood that, despite being a single worker, the impact of his or her removal or functional re-adaptation will be proportional to the number of ties.
A study carried out in Brazil, whose objective was to outline the profile of nursing professionals, observed that, despite the growth in recent years of male professionals, there is still predominance of female professionals, representing 85.1% among the 1,804,535 research participants19. In this perspective, the present work presents a similar result to other studies20-22. Women have a greater workload compared to men. This workload stems from their double or triple work shift. In addition to professional (formal) work, they also have to perform household chores and family care, which implies a greater physical and mental exhaustion for these professionals, generating guilt for unsatisfactory fulfillment in their roles, including the professional one, and all this can be translated as a potential factor for their illness 23.
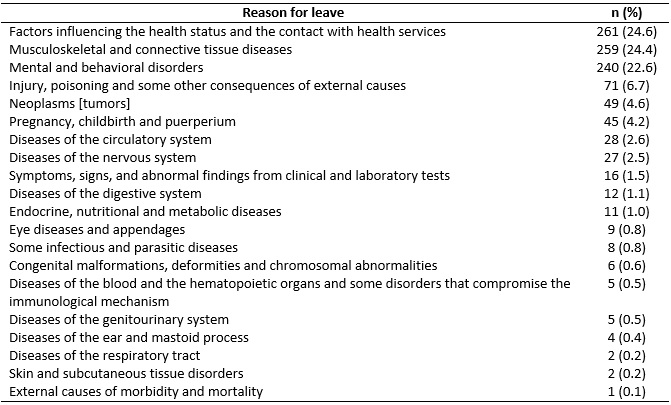
There was a great variety of reasons that led these professionals to take a leave, as observed in Table 1. It should be noted that the number of leaves was 829, but the number of reasons found (1,061) is higher, since in some cases, the professionals had more than one impairment to justify it. Data were categorized using the large grouping of the International Classification of Diseases (ICD-10).
According to the survey, the professionals had taken leave mainly due to factors that influence the health status and the contact with health services, 261 times (24.6%); next, due were diseases of the musculoskeletal system and connective tissue, 259 times (24.4%); and due to mental and behavioral disorders, 240 times (22.6%). Workers had taken an average of 36 days of leave. No records of death or disability were found for nursing professionals.
Table 1:
Reasons for leave, as stated by professionals. Rio de Janeiro Brazil, 2016.
Approximately 67.8% of nursing professionals are between 31 and 55 years old19. Thus, the age group that has taken more leaves is also the one that includes the greatest majority of the professionals, which can demonstrate a bias of the study. In addition, we also found early sick leave of these professionals, being more frequent in professionals between 30 and 49 years old21,22. The early illness of these workers, besides resulting in absenteeism, also leads to the inability to carry out their work temporarily or permanently, compromising the assistance and the worker's quality of life4.
Under the neoliberal model, there is the uncertainty of permanence at work, high unemployment, informal and unstable labor ties, which lead workers to remain in more than one job in order to guarantee material subsistence and a more economically stable future. This situation reinforces the wear and the psychophysical suffering of the workers, thus evidencing an even greater potential for the sickness of the professionals as a group 3.
A study carried out previously in a university showed that nursing professionals have taken longer leaves and more frequently when compared to other professional categories. There was a higher frequency of diagnoses among this population related to mood disorders, controlled medication prescriptions, search for multiprofessional care and sick leave due to mental disorders24.
Professionals in this category play a role that deals directly with human suffering. Added to this is the nature of the nursing work, in which the worker has low control over the activity performed and faces a high degree of demands. These characteristics are notoriously predictive of psychic suffering25,26.
The category that presented the greatest amount of sick leaves, in this study, was the nursing technicians, representing 76.6% of the total. Nursing technicians and assistants currently account for 77.0% of the professional category and are therefore the largest nursing workforce, which would easily explain the higher incidence of leaves among these categories19. These professionals perform activities that demand greater physical effort and high emotional exhaustion, because they are in direct contact with the patients, experiencing the illness, family suffering and the death-dying process 5, situations that lead to psychophysical illness. Also, they become more vulnerable to occupational hazards and occupational accidents 27.
As a reflection of low pay, professionals must have more than one employment relationship in order to meet their personal needs. The multiplicity of jobs wears the professionals physically and emotionally, increasing the likelihood of getting sick. An inferior workload, coupled with an adequate remuneration, would make the professional more productive, with a lower risk of illness, and consequently, taking less leaves, which would positively impact the final costs of labor28.
Regarding the recurrent causes of leave indicated by the study, other works with the same theme point to diseases of the musculoskeletal system and connective tissue as the major cause of sick leaves20-22. Nursing professionals are the ones who most suffer from "Work-Related Musculoskeletal Disorders," and the causes mentioned by the professionals themselves are working for long periods in the same position, working in inadequate positions and performing the same task repeatedly29. As it is difficult to change the nature of nursing work, which is pointed to be a predictor of illness, it is undeniable the importance of reducing the workload of these professionals.
In several studies, mental and behavioral disorders were described as one of the first five causes of leave20-22. A time series carried out in a university hospital verified that there has been an average increase of 1% in each year of nursing professionals who take leaves due to mental and behavioral disorders30. The main reasons for these leaves are the depressive episodes, the recurrent depressive disorder and the affective-bipolar disorder5.
Nowadays, occupational sickness due to mental health issues is growing and worrying. This phenomenon can be related to the predominance of the neoliberal precepts that bring uncertainty to the worker, imposition on workers by polyvalence and multifunctionality, subjection to the pressures of daily work, to the precarious bond of work and to wages increasingly degrading, among other developments that impact negatively the subjective dimension of the worker. In this sense, there is a conducive context for triggering mental illness and behavioral changes31.
The units with the greater amount of professionals on leave were the Surgical Unit, with 273 (32.9%), the Intensive Care Unit, with 177 (21.4%), and the Women and Child Care Services, with 148 (17.9%) leaves. The units of performance that had similar characteristics were grouped and arranged in categories in order to not have dispersion of results.
The number of days of leave totaled 29,931 days of work, during the studied period, a very significant figure. This amount is equivalent to approximately 82 years of work, which reflects a great loss to the employer. Thus, this scenario does not only generate economic impact, but also leads to the overload of the workers who remain in the work environment and need to perform the tasks of the absentees32.
With regard to the data on re-adaptations, it was found that, analogous to the profile of the professionals who had taken leave, it was also found that the majority of the re-adapted professionals belonged to the female sex (79.5%), were between 46 and 55 years old (70.4%) and performed the role of nursing technicians (79.5%). There was a significant number of nurses who had undergone functional re-adaptation, that is, nine professionals, representing 20.4% of the sample.
There was a total of 64 records of professional re-adaptation in the study period. It is important to clarify that the number of reasons for rehabilitation is higher than the number of professionals who were re-adapted, because in some cases there was more than one reason that led the professional to functional re-adjustment.
For the presentation of data, we used the classification system adopted by the service in which the study was performed. This classification is similar to the major ICD-10 groups and divides health problems in the following categories: musculoskeletal, mental health, neurological, genital-urinary, gastroenterology, endocrine, auditory, cardiovascular, respiratory, general infections, hematological, skin and cutaneous tissue, ophthalmologic, cancer and others. However, among the existing categories, gastroenterology, general infections and hematology did not obtain entries and therefore are not presented in the table.
Table 2:
Reasons that led nursing professionals to readaptation. Rio de Janeiro,
Brazil, 2016.
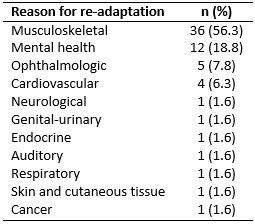
Consistent with the reasons for leave, the categories that most resulted in functional re-adaptation were musculoskeletal, with 36 (56.3%) occurrences; followed by mental health, with 12 (18.8%); and ophthalmological causes, with 5 occurrences (7.8%).
The sites with the greatest number of professionals who had undergone functional re-adaptation were the Surgical Unit, with 14 (26.9%); the Medical Clinics, with 12 (23.0%); and the Intensive Care Unit, with 10 (19.2%), which had a high adherence with the places that had the greatest number of professionals on sick leave.
It should be noted that eight of the 52 re-adaptations described above represent professionals who had been re-adapted twice within the same year. This may mean that the limitations established a priori were insufficient and needed to be reviewed a posteriori or that the professional had his/her health condition even more deteriorated and had to suffer new labor restrictions.
The profile of the re-adapted professionals was very similar to that of the professionals on leave, that is, the majority were female (79.5%), between 46 and 55 years old (70.4%) and worked as nursing technicians (79.5%). This may indicate a progressive reduction of the workers' working capacity due to illness, making the process of functional re-adaptation necessary to make their work compliant with their health restriction. To confirm this, further cause-and-effect studies will be needed.
Among the participants who had undergone functional re-adaptation, 9 (20.4%) were nurses (20.4%). The nurse occupies leadership positions in the nursing team. The managerial characteristic of the nurse, while distancing them from direct contact with the patient, exposes them to a high stress load, as they are responsible for the performance of their own work and the supervision the work of others. As a result of this situation, nurses end up avoiding to take leaves, even when ill, because of the responsibility towards their team7.
The two main reasons for functional re-adaptation were the same ones that motivated the leave of the other professionals studied, that is, musculoskeletal disorders, with 56.2%; and mental health problems, with 18.7%. Musculoskeletal problems have great relevance in the process of functional re-adaptation. A study pointed out that bodily pain was one of the most frequently mentioned domains referred by re-adapted nursing professionals, since it is incapacitating, besides breaking concentration and attention during the accomplishment of labor tasks33.
The multidimensional precariousness of the work environment, such as the lack of material and human resources, for example, impels the worker to accelerate their work to fill this gap, and the obligation of polyvalence so that they can perform multiple tasks at the same time increase wear29-34.
CONCLUSION
Most of the professionals had taken leave due to factors that influence the health status and due to contact with health services, especially due to diseases of the musculoskeletal system and connective tissue and mental and behavioral disorders. The total number of days off, which was 29,931 days, represents more than 82 years of work lost. In relation to the re-adapted professionals, the main causes of re-adaptation were musculoskeletal disorders and mental health. Despite its relevance, the functional re-adaptation of nursing professionals is still a topic that is scarcely discussed in publications. This situation makes it difficult to understand more clearly the reasons that result in the limitation of the work capacity of the professionals, making it necessary that more studies are carried out in this area.
REFERENCES
1.Alves AP, Pedrosa LAK, Coimbra MAR, Miranzi MAS, Hass VJ. Prevalence of common mental disorders among health professionals. Rev enferm UERJ. 2015; 23(1):64-9. Doi: http://dx.doi.org/10.12957/reuerj.2015.8150
2. Felli VEA. Nursing work conditions and sickness: reasons to reduce the workday to 30 hours. Enferm foco[Internet]. 2012 [cited in 2016 Dez 15]; 3(4):178-81. Available from: http://revista.portalcofen.gov.br/index.php/enfermagem/article/view/379/170
3.Gonçalves FGA, Souza NVDO, Pires AS, Santos DM, D'Oliveira CAFB, Ribeiro LV. Neoliberal model and its implications for the health of nursing workers . Rev enferm UERJ [Internet]. 2014 [cited 2016 May 12]; 22(4):519-25. Available from: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/15395/11646
4.Mininel VA, Felli VEA, Silva EJ, Torri Z, Abreu AP, Branco MTA. Workloads, strain processes and sickness absenteeism in nursing. Rev Latinoam Enfermagem. 2013; 21(6):1290-97. http://dx.doi.org/10.1590/0104-1169.2992.2366
5.Marques DO, Pereira MS, Souza ACS, Vila VSC, Almeida CCOF, Oliveira EC. Absenteeism – illness of the nursing staff of a university hospital. Rev Bras Enferm. 2015; 68(5):876-82. http://dx.doi.org/10.1590/0034-7167.2015680516i
6.Silva AM, Guimarães LAM. Occupational stress and quality of life in nursing. Paidéia. 2016; 26(63):63-70. http://dx.doi.org/10.1590/1982-43272663201608
7.Ferreira RC, Griep RH, Fonseca MJM, Rotenberg L. A multifactorial approach to sickness absenteeism among nursing staff. Rev Saúde Pública. 2012; 46(2):259-68. http://dx.doi.org/10.1590/S0034-89102012005000018
8.Faria JIL, Kurcgant P. Nursing professionals' sick leave: characteristics and actions adopted by nurse managers. Cogitare Enferm. 2014; 19(2):224-31. http://dx.doi.org/10.5380/ce.v19i2.34334
9.Dutra FCMS, Costa LC, Sampaio RF. The influence of medical work leaves in the perception of health and quality of life of adult individuals. Fisioter Pesqui. 2016; 23(1):98-104. http://dx.doi.org/10.1590/1809-2950/14900923012016
10.Rouquayrol MZ, Gurgel M. Epidemiologia e Saúde. 7. ed. Rio de Janeiro: Medbook, 2013.
11.Fischborn AF, Viegas MF. The activity of nursing workers in a hospital: between norms and renormalizations. Trab educ saúde. 2015; 13(3):657-74. http://dx.doi.org/10.1590/1981-7746-sip00060 .
12.Gutierrez BAO, Ciampone MHT. Nursing professionals facing the process of death in intensive care units. Acta Paul Enferm. 2006; 19(4):456-61. http://dx.doi.org/10.1590/S0103-21002006000400015 .
13.Silva AM, Guimarães LAM. Occupational stress and quality of life in nursing. Paidéia. 2016; 26(63):63-70. http://dx.doi.org/10.1590/1982-43272663201608 .
14.Gonçalves FGAG, Souza NVDO, Pires AS, Santos DM, D'Oliveira CAFB, Ribeiro LV. Neoliberal model and its implications for the health of nursing workers. Rev. enferm Uerj [Internet]. 2014 [cited in Mar 29, 2016]; 22(4):519-25. Available from: http://www.facenf.uerj.br/v22n4/v22n4a14.pdf> .
15.Shoji S, Souza NVDO, Farias SNP. Impact of the work environment on the health disease process of nursing workers of a specialized outpatient unit. Rev min enferm. 2015; 19(1): 43-8. http://www.dx.doi.org/10.5935/1415-2762.20150004 .
16.Mininel VA, Baptista PCP, Felli VEA. Psychic workloads and strain processes in nursing workers of Brazilian university hospitals. Rev latinoam enfermagem. 2011; 19(2): 340-7. http://dx.doi.org/10.1590/S0104-11692011000200016 .
17.Malaguti SE, Hayashida M, Canini SRMS, Gir E. Nurses with leadership positions and preventive measures to occupational exposure: facilities and barriers. Rev esc enferm Usp.2008; 42(3):496-503. http://dx.doi.org/10.1590/S0080-62342008000300012 .
18.Sass O. On the concepts of census and sampling in education, in Brazil. Statistics and Society [Online]. 2012 [Accessed in Aug 28, 2018]; 2:128-41. Available from: http://seer.ufrgs.br/index.php/estatisticaesociedade/article/download/34902/23645 .
19.Machado MH, Filho WA, Lacerda WF, Oliveira E, Lemos W, Wermelinger M, et
al. General Characteristics of Nursing: the sociodemographic profile.
Enferm foco. 2016; 7:9-14.
https://doi.org/10.21675/2357-707X.2016.v7.nESP.686
.
20.Santana LL, Miranda FMAM, Karino ME, Baptista PCP, Felli VEA, Sarquis LMM. Description of workloads and fatigue experienced among health workers in a teaching hospital. Rev GaúchaEnferm. 2013; 34(1):64-70. DOI: http://dx.doi.org/10.1590/S1983-14472013000100008 .
21.Bernardes CL, Vasconcelos LHS, Silva SM, Baptista PCP, Felli VEA,
Pustiglione Met al. Health problems of nursing workers in a public
educational institution. Rev. Esc Enferm USP. 2014; 48(40):677-83. DOI:
http://dx.doi.org/10.1590/S0080-623420140000400015
.
22.Guimarães ALO, Felli VEA. Notification of health problems among nursing workers in university hospitals. Rev. Brás enferm. 2016; 69(3):507-14. DOI: http://dx.doi.org/10.1590/0034-7167.2016690313i
23.Rodrigues BC, Lima MF, Maschio Neto B, Oliveira GL, Corrêa ACP, Higarashi IH. Being a mother and a nurse: issues about gender and overlapping social roles. Rev Rene. 2017; 18(1):91-8. DOI: http://www.dx.doi.org/10.15253/2175-6783.2017000100013
24.Araújo GS, Sampaio AS, Santos EM, Barreto SMG, Almeida NJV, Santos MLD. Profile of nursing professionals assisted by a multidisciplinary mental health team. Rev Rene. 2014; 15(2):257-63. DOI: http://www.dx.doi.org/10.15253/2175-6783.2014000200010
25.Rodrigues EP, Rodrigues US, Oliveira LMM, Laudano RCS, Nascimento Sobrinho, CL. Prevalence of common mental disorders in nursing workers in a hospital in Bahia. Rev. bras. enferm. 2014; 67(2):296-301. DOI; I 10.5935/0034-7167.20140040.
26.Silva JLL, Teixeira LR, Soares RS, Costa FS, Aranha JDS, Teixeira ER. Stress and psychosocial factors in the work of intensive care nurses. Enferm. Glob. 2017; 16(48):80-120. Doi: http://dx.doi.org/10.6018/eglobal.16.4.249321 .
27.Karino ME Felli VEA, Sarquis LMM, Santana LL, Silva SR, Teixeira RC. Workloads and strain processes of nursing workers at teaching hospital. Cienc cuid saúde. 2015; 14(2):1011-8. DOI: http://www.dx.doi.org/10.4025/cienccuidsaude.v14i2.21603
28.Felli VEA. Nursing work conditions and sickness: reasons to reduce the workday to 30 hours. Enferm foco [Internet]. 2012 [cited in Dec, 10 2016]; 3(4):178-81. Available from: http://revista.portalcofen.gov.br/index.php/enfermagem/article/view/379/170
29.Yasobant S; Rajkumar P. Work-related musculoskeletal disorders among health care professionals: A cross-sectional assessment of risk factors in a tertiary hospital. Indian J Occup Environ Med. 2014; 18(2):75-8. DOI: http://dx.doi.org/10.4103/0019-5278.146896
30.Falavigna A, Carlotto MS. Temporal trend of absenteeism from word due to mental and behavioral disorders in nurses (1998-2008). Rev psicol organ Trab[Internet]. 2013[cited in Dec 15, 2016]; 13(3):363-71. Available from: DOI: http://pepsic.bvsalud.org/pdf/rpot/v13n3/v13n3a12.pdf
31.Rocha SH, Bussinguer ECA. The invisibility of occupational mental illnesses in the contemporary world of work. Pensar[Internet]. 2016 [cited in June 10, 2016]; 21(3):1104-22. Available from: http://periodicos.unifor.br/rpen/article/download/4470/pdf_1
32.Fakih FT, Tanaka LH, Carmagnani MIS. Nursing staff absences in the emergency room of a university hospital. Acta paul enferm. 2012; 25(3):378-85. DOI: http://dx.doi.org/10.1590/S0103-21002012000300010 .
33.Cacciari P, Haddad MCL, Vannuchi MTO, Dalmas JC. Health status of nursing workers in functional retraining and re-adaptation. Rev bras enferm. 2013; 66(6):860-5. DOI: http://dx.doi.org/10.1590/S0034-71672013000600008 .
34. Souza NVDO, Gonçalves FGA, Pires AS, David HMSL. Influence of neoliberalism on the organization and nursing hospital work process. Rev bras enferm. 2017, 70(5):961-9. DOI: http://dx.doi.org/10.1590/0034-7167-2016-0092 .