NW = notified withdrawal; NNW = non-notified withdrawal; IA = irregular adherence
ORIGINAL RESEARCH
Adherence to antiretroviral therapy by HIV/AIDS patients with lipodystrophy
Dalva Francês CostaI; Ana Sofia Resque GonçalvesII; José Ricardo dos Santos VieiraIII; João Farias GuerreiroIV
I
Nurse. João de Barros Barreto University Hospital. PhD student in Tropical
Diseases. Federal University of Pará. Brazil. Email: dalvafrances@ufpa.br
II
Nurse. Federal University of Santa Catarina. Associate Professor, Federal
University of Pará. Brazil. Email: sofiaresque@gmail.com
III
Pharmacist. PhD in Genetics and Biology. Adjunct Professor, Federal
University of Pará. Brazil. E-mail: jrvieira@ufpa.br
IV
Physician. PhD in Biological Sciences. Full Professor, Federal University
of Pará. Brazil. E-mail: joaofg@ufpa.br
DOI: https://doi.org/10.12957/reuerj.2018.31156
ABSTRACT
Objective: to profile adherence to antiretroviral therapy (ART) by patients with human immunodeficiency virus lipodystrophy syndrome (HIVLS) at a specialized unit in Pará, Brazil. Method: this quali-quantitative study, involving a questionnaire and medical records of 124 patients, was conducted from February to March 2013, after research ethics approval. In the analysis, statistical tests were related by variance (p<0.05), and data were presented in table form. Results: the difficulties of understanding and knowing the therapeutic regimen, mellitus diabetes and changes in lipodystrophy were significant in the interference of ART adherence. The irregular adherence group is at risk for treatment efficacy. The others have the possibility of migrating from one group to another at any time. Conclusion: the profile of adherence to ART is not defined by socioeconomic data. Participation in membership groups should be encouraged as a factor in reversing the pattern of abandonment.
Descriptors: HIV; SIDA; lipodystrophy; adherence to medication.
INTRODUCTION
Acquired Immunodeficiency Syndrome (AIDS) has been one of the most important pandemics and one of the most serious public health problems in the world. According to the World Health Organization, the agent causing AIDS, the Human Immunodeficiency Virus, has played a significant role, mainly because it has affected 34 million people. Of these, 3.3 million are children under the age of 15. Among the 30.7 million adults, 14.0 million are men and 16.7 million are women, reflecting the continued feminization of the epidemiological distribution, reversing the situation of past decades1,2.
Since 1996, Brazil has adopted universal access to highly active antiretroviral therapy (ART) with great benefits for people living with HIV/AIDS. Since 2013, the Ministry of Health (MOH) has recommended the immediate start of ART in all people living with HIV/AIDS, considering the motivation of the patient3. Despite the efficacy of ART, adverse drug reactions may be reasons for decreased adherence to treatment, which is a complicating factor for public health programs4. This is the case of lipodystrophy, an important side effect with usually progressive development of physical signs, increasing severity, which lasts for a period of 18 to 24 months and stabilizes after about two years5. The main risk factors for lipodystrophy are time of HIV infection, age and time of ART. The process is slow and can take years to be perceived and cause discomfort to the patient6.
To date, there is no definitive and curative treatment for lipodystrophy, and the various strategies used in the treatment have a variable degree of success which is mainly related to physical exercise, minimal and/or delayed exposure to ART, surgical treatment and nutritional guidance 6,7. Further research on this subject is needed. Research on adherence of patients living with AIDS and lipodystrophy is still insufficient. It s also important to improve the records and follow-up of these patients in order to build a more solid database for the further research.
Although ART is essential in the treatment of HIV/AIDS/lipodystrophy and has worked well, there are still problems in adherence. Therefore, the objective of this study was to describe the profile of adherence to antiretroviral therapy in patients with diagnosis or clinical signs of lipodystrophy. Regardless of the time of treatment, it is needed to analyze.
LITERATURE REVIEW
The emergence of the first AIDS cases in Brazil in the 1980s coincided with the installation of a serious economic, social and political crisis in the country. The fact provoked intense social mobilization that served to stimulate the first political actions in favor of the creation of the Unified Health System and definition of the first steps to establish governmental responses to the epidemic8,9.
The epidemiological situation of AIDS presents a development cycle characterized by an increase in the incidence rate and maintenance of high levels throughout the world. This has been the case in different regions of Brazil, markedly in populations of greater vulnerability10. Because it is a public health problem, it is the responsibility of health managers and health professionals to develop effective prevention and treatment strategies for people living with the syndrome11.
In this perspective, it is the responsibility of the academies, through the exercise of teaching activities, to train professionals with a view to strengthen and intensify the relationship between health professionals and users of the health system, generating satisfaction of all the segments involved in the teaching-learning process and guaranteeing quality in the provision of services to the community12.
The World Health Organization (WHO) annual report points out that from the beginning of the epidemic to June 2017, 76 million people had been infected with HIV, and approximately 21 million people had access to ART 13.
With the introduction of this therapy and its different forms of action on the HIV cycle in the human body, there was a great positive impact on the indicators of morbidity, mortality and quality of life of individuals living with HIV/AIDS. In fact, the status of this disease changed from terminal to chronic4,15. However, despite the effectiveness of ART, this therapy is responsible for a number of important side effects, including lipodystrophy.
Lipodystrophy consists in the redistribution of body fat and changes in the lipid and glycemic profile. The most common physical alterations are lipid accumulation in the abdomen, back, neck, neck, submental and pubic regions, besides gynecomastia in men and breast enlargement in women. Lipid loss in the arms, legs, gluteal region and face may result in relative prominence of the musculature and venous circulation16,17.
The body changes that affect the user's self-image and compromise the patient's physical and psychic health significantly influence the process of therapeutic adherence18-21.
METHODOLOGY
This is a descriptive, cross-sectional, uncontrolled study with a qualitative approach. The study was developed in the ambulatory of the service of the Special Reference Unit for Special Infectious and Parasitic Diseases of the State Secretariat of Public Health of Pará (URE/DIP) in Belém, in the year 2013.
The study was approved under number 267.224 of 04/30/2013, by the Ethics and Research Committee of the João de Barros Barreto University Hospital. The ethical-legal precepts of research procedures involving human beings were obeyed and respected.
The sample consisted of 124 participants who attended the unit from February to March 2013. The selection was based on the following criteria: individuals with HIV/AIDS of both sexes, aged between 20 and 70 years (mean of 42.4 ± 10.5 years), and who presented clinical signs or diagnosis of HIV-associated lipodystrophy, following the guidelines of the Ministry of Health17. We excluded from the study the individuals who did not meet the established diagnostic criteria and who presented metabolic disorders and/or lipodystrophy prior to the diagnosis of HIV infection, as well as pregnant and breastfeeding women.
Data were collected by consulting the medical records of the enrolled patients, who were also interviewed. The sample was obtained through the non-probabilistic method. A questionnaire was used to collect data, including items on socioeconomic informatiom (sex; age; marital status; address; profession; family income; schooling; smoking habit; and regular alcohol consumption); items to evaluate the understanding of important factors for ART adherence (understanding of the therapeutic scheme; side effects of ART; regular practice of physical exercises; attendance to consultations with nutritionists; adherence to dietary guidelines); and items on the pathological condition of patients (lipodystrophy interferes with ART adherence; the importance of adherence to treatment and clinical evolution; the importance of participation in the adherence group ). Anthropometric, clinical and laboratory data were also collected to identify the presence of dyslipidemia, obesity and Diabetes Mellitus (DM).
Based on the information on ART suspension, four adherence/withdrawal groups were created, as established in Technical Note Nº 208/09 prepared and published by the Health Surveillance Secretariat (SVS) of the Ministry of Health (MOH), namely: regular adherence (RA): patients who maintained regular adherence to ART; (IA): all patients whose interval of time to return to medical consultations was less than 6 months, or who had irregular schedules for medication intake, or who missed doses (1 day or more), and who suspended therapy at weekends; notified withdrawal (NW): all cases of withdrawal duly notified to the Ministry of Health; and non-notified withdrawal (NNW): patients who discontinued ART and whose withdrawal was not officially notified.
The analysis of variance of the correlation between the responses provided in the questionnaire regarding adherence/abandonment groups was made using the Kruskal-Wallis test, to investigate to which extent the differences between the responses in each group were discriminant for the differentiation of the groups. To compare variables of patients with regular adherence in relation to the other groups, discriminant analysis, canonical discriminant determination, the Student's t- test, Chi Square, G and Fisher Exact tests were performed, according to the variable, using the program Bioestat5.0®. In all the analyses, the level of significance of p -value < 0.05 was adopted. The information obtained was stored in a database plotted in MS Office Excel spreadsheets (2007 version) and presented in tables.
RESULTS
A total of 124 HIV/AIDS patients with lipodystrophy participated in the study; the majority were men (n = 85/67%) and the minority women (n = 39/32%), occurring in a ratio of 2.2 men to every woman. Sixty-eight (55%) participants were single; 69 (55.70%) lived in the city of Belém; 82 (66%) had a family income of up to one minimum wage; 97 (78%) had attended the complete Elementary School. There was a predominance of patients who did not consume alcoholic beverages (89, 72%), and were non-smokers, 110 (89%). It was found that 26 (21%) participants knew the concept of lipodystrophy, 12 (46.2%) learned the concept in the unit itself, 8 (30.8%) in the Internet and 6 (23.0%) in other sources.
It was evidenced that 75 (60.48%) patients attributed some type of adverse reaction to ART; among them, 17 (22.70%) reported that lipodystrophy was the effect that bothered them the most. Information on dyslipidemias was provided in the medical records of only 78 (100%) patients, and 44 (56.40%) of those records listed laboratory abnormalities.
Regarding adherence to treatment, 100 (80.60%) patients confirmed to be aware of its importance. Among these, 44% pointed to increased survival and improved health as the main benefits of the correct use of ART (22% for each variable). Improved quality of life was pointed out as the greatest benefit obtained by 18 (18%) patients.
Although physical activity is one of the recommendations for the control and treatment of changes caused by lipodystrophy, 111 (89.52%) patients were did not practice them. Likewise, 112 (90.30%) patients did not attend the service for dietary control and guidance. Among the reasons for the latter behavior, 74 (66.10%) of the 112 patients claimed disinterest or found it unnecessary to seek such guidance; 21 (18.70%) claimed ignorance or lack of time for it; 7 (6.3%) did not seek information because they were not referred to this service; and 10 (8.9%) reported other reasons.
Thirty-eight (30.70%) patients had difficulty understanding the therapeutic scheme; of these, 21 (16.90%) because of the hours for medication intake, and 17 (17.80%) because of the adjustment of the doses with the hours. Eighty-nine patients had suspended the medication on their own at some point (71.80%).
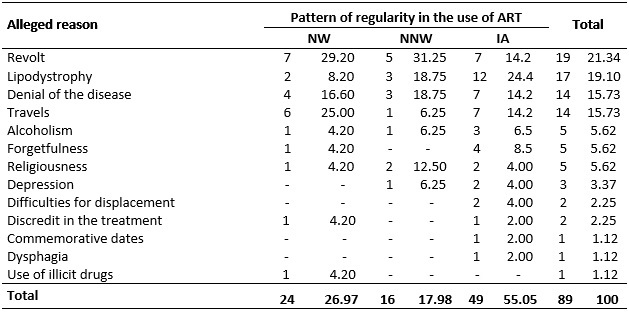
The feeling of revolt was reported by 19 (21.34%) patients as a reason for withdrawal; 17 (19.10%) cited the presence of lipodystrophy; and other reasons were mentioned by the patients, ranging from the denial of the disease to travels and use of illicit drugs, as shown in Table 1.
TABLE 1:
Reasons mentioned by HIV/AIDS patients with diagnosis or signs suggestive
of lipodystrophy regarding the pattern of regularity in the use of ART
(abandonment or irregular adherence). Belém, Pará, Brazil, 2013.
NW = notified withdrawal; NNW = non-notified withdrawal; IA = irregular
adherence
Conventional sign used equal to zero not resulting from approximation.
As for the adherence group, 106 (85.47%) patients did not attend the meetings, 78 (62.90%) claimed to be unaware of the purpose and existence of this group. Quality of life was not affected by lipodystrophy in the case of 71 (57.26%) of the respondents. It is worth mentioning that 50 (40.32%) claimed that lipodystrophy caused several interferences, ranging from embarrassment to discrimination, according to Table 2.
TABLE 2:
Interference of changes caused by lipodystrophy in activities of daily
living in HIV/AIDS patients with diagnosis or signs suggestive of
lipodystrophy. Belém, Pará, Brazil, 2013.
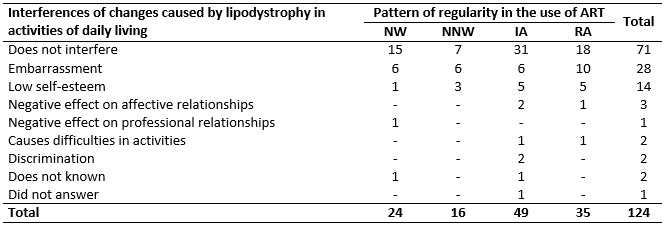
NW = notified withdrawal; NNW = non-notified withdrawal; IA = irregular
adherence; RA = regular adherence. Conventional sign used equal to zero not
resulting from approximation.
The responses among the patients in the adherence/withdrawal groups were varied. Only four responses showed significant differences (p-value < 0.05) discriminating each group of adherence/withdrawal and were considered crucial to define the profile of irregular or regular withdrawal or adherence to ART. These responses are distributed in four groups according to Table 3.
TABLE 3:
Responses on the items considered discriminant for the types of adherence
and withdrawal from antiretroviral therapy in HIV/AIDS patients with
lipodystrophy. Belém, Pará, Brazil, 2013.
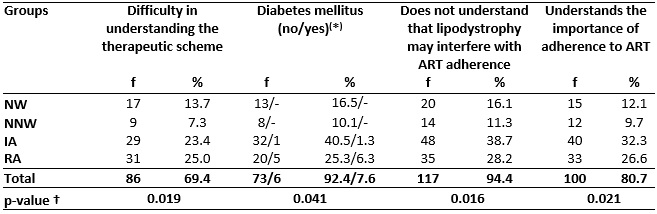
(
*) Data calculated from 79 medical records; † Kruskal-Wallis
test.
NW = notified withdrawal; NNW = non-notified withdrawal; IA = irregular
adherence; RA = regular adherence. Conventional sign used equal to zero not
resulting from approximation.
Considering the pattern of ART regularity, 24 (19.40%) cases were classified as notified withdrawal (NW), 16 (12.90%) as non-notified withdrawal (NNW), 49 (39.50%) as irregular adherence (IA) and 35 (28.20%) as regular adherence (RA). In the NNW group, the one with the highest index, 50% were classified correctly and met the inherent characteristics of NNW. Among the cases of IA, only 22% were correctly classified; and 46% of the RA cases were correctly classified.
The canonical discriminant function analysis was performed to evaluate the grouping pattern of the four adherence/abandonment groups; the analysis discriminates the dispersion of the groups among themselves and gives centroid values of each group which representthe mean of the results. The centroids of the four groups appear very close to each other, with an intense and significant dispersion of the elements that make up the four groups, where the patients had their profiles distributed, according to the characteristics of each group. The ideal variation would be that the centroids were dispersed among themselves and the components (individuals) were as close as possible to the centroid representative of their group.
DISCUSSION
The results showed that socioeconomic data (gender, age, marital status, occupation, family income, schooling, smoking and regular alcohol consumption) were not significant in the adherence process, nor did they discriminate for abandonment of antiretroviral therapy, in line with several studies5,20,21.
The same was observed as to variables that have a direct relationship with lipodystrophy (adverse reaction that causes greater discomfort; presence of dyslipidemia and practice of physical exercises; nutritional monitoring and food control measures; knowledge about lipodystrophy; adherence group and participation of meetings), which did not present statistical significance when related to adherence and withdrawal from ART, which is contrary to other studies6.
Despite the predominance of negative responses to the practice of physical exercises, in the present study there was no significant statistical association between practice of physical activities and the adherence/withdrawal from therapy. Regular physical exercise may be beneficial for metabolic changes and probably also for redistribution of central and intramyocellular fats; physical exercise should, therefore, be considered a recommendation for all HIV-infected patients6.
Sedentary lifestyle associated with dyslipidemias did not present a significant relation with the adherence/withdrawal pattern. This result, a priori, does not seem justifiable, considering that physical activities play an important role in reduction of weight and body fat, increase of lean body mass, decrease of blood pressure and increase of insulin sensitivity6. This lack of connection is an indication that the individuals did not correlate these factors with the onset of lipodystrophy and/or with the complication of their clinical condition, indicated by the high rate of non-attendance to the meetings of theadherence group and to consultations with nutritionists7.
Four variables presented a statistically significant association: difficulties in understanding the therapeutic scheme; presence of DM; understanding that lipodystrophy may interfere with ART adherence; and knowledge about the importance of ART adherence. These results are similar to those reported in other studies that indicate times and number of doses, amount, taste and size of the tablets7.
The difficulty in understanding the therapeutic scheme is an important fact, as it reflects the quality of the service offered by the healthcare unit responsible for the care and, above all, it indicates an urgent need to review the way information about medication intake is being passed on. The taste, size, form of storage, amount of tablets and other factors may conflict with the routines and the lifestyle of the patients, causing them to present certain difficulty to understand the therapeutic scheme 7. Results reported in of divergent researches22 indicate that the issues related to knowledge acquired in the health unit by patients had reached a satisfactory level (78.7% to 95.7%), indicating that there was an adequate satisfaction regarding the importance of adherence to treatment22.
The presence of diabetes was a discriminant variable for adherence. However, of the 124 investigated patients, only in 79 had medical records with clinical-laboratory confirmation of diabetic and non-diabetic patients, which may bring a bias to the analysis, visualized in a p-value threshold cut-off value of 0.05. However, it was observed that among the six diabetic patients in the sample, five had regular adherence and only one had irregular adherence to ART. Ingestion of a greater number of drugs/day, typical of diabetic patients, may improve adherence because a routine of administering medications at fixed times is seen with more naturalness. Discordant results are shown in studies where, on the contrary, the combined intake of several drugs for comorbidities impairs adherence to ART22.
Regarding the understanding that lipodystrophy may interfere with ART adherence, this is a discriminant factor of the adherence group; the majority of individuals who understood the importance of lipodystrophy were in the group of regular adherence (38.7%), and irregular adherence (28.2%). Likewise, knowledge about the importance of adherence to ART was confirmed by 26.6% (RA) and 32.3% (IA). However, when it comes to side effects, it was observed that lipodystrophy was discriminant in the process of withdrawal and adherence to treatment with antiretrovirals (p-value = 0.016); it is worth noting that body changes impair the patient's self-image, leading to a reduced quality of life, and, consequently, decreased treatment adherence, often resulting in therapeutic failure23.
Even when patients with regular adherence were asked about the psychological impact and effects on daily life activities, although all had lipodystrophy, only 10 (47.6%) of them reported a profound impact on daily life. This, however, did not lead them to interrupt treatment on their own, but made it much harder to accept these modifications of the body. The reasons identified were: negative self-image perception; avoidance of social contact; reduction of self-confidence; changes in mood states; feelings of frustration at the absence of satisfactory results and negative perception of self-esteem.
The magnitude of the problem can be seen in the patients' own speech, when they consider the possibility of abandoning ART to search a more harmonic body, because of the body changes that are perceived by other people and that lead them to avoid leaving home, for fear of the recognition by people of the stigmatized appearance of AIDS24.25.
It was observed that there was no standard grouping behavior of the regular adherence groups to ART compared to those who withdraw from treatment; there is no guarantee that someone with regular adherence to treatment will not abandon it, and those who already withdrew from treatment, may resume regular treatment.
CONCLUSION
Socioeconomic data do not define the profile of adherence/withdrawal to ART; however, the majority of individuals with irregular adherence to this therapy are at risk of treatment inefficiency. Data such as temporary suspension of treatment on weekends and holidays to use alcohol should be monitored as an important factor for irregular adherence, which may be characterized by temporary suspension, ranging from one to 72 months, indicating that temporary suspension is very frequent and the time of suspension may be very long.
Psychological follow-up is important in this group of individuals, as indicated by the fact that revolt and the presence of lipodystrophy were identified by most patients as the main determinants of treatment irregularity.
There is a clear need to improve the role of the group among patients. Group meetings are of paramount importance for the patients' adherence to the treatment, besides being recommended by the Ministry of Health. Understanding the therapeutic scheme is decisive for defining the adherence process, because it contributes to an easier management of doses and schemes of treatment by the patient. The professionals responsible for guiding the use of the therapeutic regimen must make sure that patients understand the prescribed drugs, the schedule, the doses, and even the visual aspect of each medication in order to facilitate their understanding and minimize medication errors, and increase the quality of adherence.
Among the limitations of the study, the patient's lack of understanding of the problem, lack of support on the part of the professionals, and lack of information in the medical records stood out. These facts hampered the consistent evaluation of the findings and limited the generalization of the results.
Further studies may show actions implemented to improve the understanding of the problem by the patients and the support team, reviewing the pattern of regular adherence to ART, as well as compare other strategies adopted by different treatment centers to improve adherence to this therapy.
REFERENCES
1.Ministry of Health (Br). AIDS in Brazil: epidemic concentrated and stabilized in populations of greater vulnerability. Epidemiological Bulletin. 2012; 43 (1): 8-10.
2.Ministry of Health (Br). STD and AIDS. Epidemiological Bulletin. 2014; 3(1): 80.
3.Dye C. After 2015: infectious diseases in a new era of health and development. Phil. Trans. R. Soc. B 369: 20130426. 2014; 369(1645): 20130426. doi: 10.1098/rstb.2013.0426.
4.Prosperi MC, Fabbiani M, Fanti I, Zaccarelli M, Colafigli M, Mondi A et al. Predictors of first-line antiretroviral therapy discontinuation dueto drug-related adverse events in HIV-infected patients: a retrospective cohort study. BMC. Infect. Dis. 2012; 12(12):296.
5. Araújo MNR, Mendes PR, Silveira APP, Seidl EMF. Lipodystrophy and prejudice in the new face of AIDS: dialogue with intervention bioethics. Revista Bioética, 2011. [cited in March 15, 2017]; 19 (2): 441-56. Available from: http://revistabioetica.cfm.org.br/index.php.
6. Signorini DJHP, Monteiro MCM, Andrade MFC, Signorini DH, Eyer-Silva WA. What should we know about metabolic syndrome and lipodystrophy in AIDS? Rev. Assoc. Med. Bras. 2012; 58 (1): 70-5.
7. Galvão MTG, Gouveia AS, Fiúza MLT, Costa E. Reflections of HIV/AIDS patients about antiretroviral therapy. Rev. Rene 2011; 12 (br): 966-72.
8.Maliska ICA, Padilha MICS, Andrade SR. AIDS and the first responses to the epidemic: contributions from health professionals. Rev. enferm. UERJ. 2015; 23 (1): 15-20.
9. Leadebal ODCP, Medeiros LB, Lins KSM, Chaves RB, Monroe AA, Nogueira JA. Care for people living with AIDS: focus on health education actions. Rev. enferm. UERJ. 2017; 25: e9524.
10. Ministry of Health (Br). Department of STD, AIDS and Viral Hepatitis. Brazilian policy on coping with AIDS: results, advances and perspectives. [Internet]. 2012 [cited in August 18, 2017]. Available from: https://www.academia.edu/7891408/Politica_brasiLeira_confronamento_aids_2012_2.
11. Silva RAR, Costa RHS, Nelson ARC, Duarte FHS, Prado NCC, Rodrigues EHF. Predictive factors of nursing diagnoses in people living with acquired immunodeficiency syndrome. Rev. latinoam. enferm. (Online). 2016 [cited in June 15, 2017]; 24: e2712. Available from: http://www.eerp.usp.br/rlae.
12.Gonçalves ASR, Pires DEP. The work of university teachers in the health area: situations that generate pleasure and suffering. Rev. enferm. UERJ. 2015; 23(2): 266-71.
13. World Health Organization. UNAIDS Report 2017. [internet]. 2017. [cited in November 10, 2017]. Available from: https://unaids.org.br/tag/relatório-unaids-2017/.
14.Giralt M, Domingo P, Villarroya F. Adipose tissue biologyand hiv-infections. Best Pract. Res. Clin. Endocrinol. Metab. 2011; 25(3): 487-99.
15.Feleke Y, Fekade D, Mezegebu Y. Prevalence of highly active antiretroviral therapy associated metabolic abnormalities and lipodystrophy in HIV infected patients. Ethiop. Med. J. 2012; 50(3): 221-30.
16.Lartey M, Asante-Quashie A, Essel A, Kenu E, Ganu V, Neequaye A. Adverse drug reactions to antiretroviral therapy during the early art period at a tertiary hospital in Ghana. Pan. Afr. Med. J. 2014; 7(18):25.
17. Ministry of Health (Br): Health Surveillance Secretariat. STD and AIDS national program. Lipodystrophic syndrome in HIV. Brasília (DF): MOH; 2011 [cited in November 18, 2017]. Available from: http://docplayer.com.br/1993038-Ministerio-da-saude-sindrome-lipodistrofica-em-hiv.html.
18. Knowing how to Live Communication. Understanding lipodystrophy better. Special Editions. [Internet], 2015. [cited in November 18, 2017] Available from: http://saberviver.org.br/publicacoes/entenda-melhor-a-lipodistrofia/.
19.Finkelstein JL, Gala P, Rochford R, Glesby MJ, Mehta S. HIV/AIDS and lipodystrophy: implications for clinical management in resource-limited settings. J. Int. AIDS Soc. 2015; 18(1):19033. doi: 10.7448/IAS.18.1.19033. eCollection 2015.
20.Zambrini H. Study of clinical and laboratory data of patients with AIDS and lipodystrophy treated in the lipodystrophy program of the Heliópolis Hospital [master's thesis]. São Paulo: University of São Paulo; 2011.
21.Schilkowsky LB, Portela MC, SÁ MC. Factors Associated with Withdrawal from Ambulatory Care in a Care Service Specialized in HIV/AIDS in the City of Rio de Janeiro. Rev. Bras. Epidemiol. 2011; 14 (2): 187-97.
22.Wilson G, Wollf M. A decade of antiretroviral therapy: a profile of patients with 10 years of highly effective triple therapy. Rev. Chilena de Infectol. 2012; 29(3): 337-43.
23.Souza Junior PRB, Szwarcwald CL, Castilho EA. Self-ratedhealthby HIV-infected individual sunder going antiretroviral therapy in Brazil. Cad. Saúde Pública (Online). 2011 [Internet]; 27(supl.1). [cited 2015 Mar 12]. Available from: http://dx.doi.org/10.1590/S0102.
24. Fiuza MLT, Lopes EM, Alexandre HO, Dantas PB, Galvão MTG, Pinheiro AKB. Adherence to antiretroviral treatment: comprehensive care based on the model of attention to chronic conditions. Esc. Anna Nery. Enferm. 2013; 17(4): 740-8.
25.Aragonés C, Sánchez L, Campos JR, Pérez J. Antiretroviral therapy adherence in persons with HIV/AIDS in Cuba. MEDICC Rev. 2011; 13(2): 17-23.