ORIGINAL RESEARCH
Chronic psychiatric client: socio-cognitive reconstruction in the institutional care process
Leandro Andrade da SilvaI; Antonio Marcos Tosoli GomesII; Iraci dos SantosIII; Maria das Graças Gazel
de SouzaIV; Adriana Loureiro da CunhaV; Leonor
Coelho da SilvaVI
I
Nurse. Post-Doctor. Professor at Veiga de Almeida University. Rio de
Janeiro, Brazil. E- mail: proflandrade@gmail.com
II
Nurse. Post-Doctor. Professor at Universidade do Estado do Rio de Janeiro.
Brazil. E-mail: mtosoli@gmail.com
III
Nurse. Post-Doctor. Professor at Universidade do Estado do Rio de Janeiro.
Brazil. E-mail: iraci.s@terra.com.br
IV
Nurse. PhD. Technologist nurse at the National Cancer Institute Jose
Alencar Gomes da Silva. Rio de Janeiro, Brazil. E-mail: mariagazel@hotmail.com
V
Nurse. Master in Nursing at EEAN / UFRJ. PhD student at PPGENF / UERJ. Rio
de janeiro Brazil. E-mail: adrianaloureiro1@gmail.com
VI
Nurse. Captain-Lieutenant of the Marine health Service of Brazil. Master in
Nursing (PPGENF / UERJ). Rio de janeiro Brazil. E-mail: lecos80@icloud.com
VII
Thanks to Coordenação de Aperfeiçoamento do Nível Superior (CAPES) for the
master's and post-doctoral scholarship.
DOI:
http://dx.doi.org/10.12957/reuerj.2017.31073
ABSTRACT
Objective:
to analyze health personnel's socio-cognitive reconstruction about chronic
psychiatric clients, contextualizing it with their time in the institution
and the care process. Method: qualitative study conducted
in 2013 with 159 participants at two hospitals in Rio de Janeiro, Brazil,
applying a structural approach to social representations, using the free
evocations technique and the software Group of Programs for the Analysis of
Evoked Responses (Ensemble de Programmes Permettant L'analyze des
Évocations, EVOC). Approved by the research ethics committee (opinions
13/2009 and 53/2010). Results: 795 words were evoked, the
minimum frequency was 9, the mean was 17. The ranking of mean orders of
evocation was 2.99. Five dimensions were constructed: imagery; positive
affectivity; institutional care; mixed affectivity; and need. Conclusion: the study afforded an understanding of mental
health personnel's social representations about clients who have aged in
asylum spaces, victims of stigmatizing, exclusionary care.
Keywords: Aging; long-term care; mental health; pychiatric nursing.
INTRODUCTION
Approximately 30 years ago, Brazil was influenced by a social movement
referring to the human rights and deinstitutionalization of the people in
psychological distress (PD). Known as Brazilian Psychiatric Reform (BPR).
Influenced by events generated after World War II, it was present in
different continents, with America Central and Europe standing out, where
the first proposals of attempts to change mental health (MH) care appeared
and were motivated especially by complaints of acts of violence,
abandonment and isolation, considered as favoring the chronification of
mental illnesses1. The inability to treat people in PD in the
asylum environment was revealed2.
For this emerging psychiatry, clients in a chronicity stage represented a
problem, and the solution proposed for more than a century was the
reclusion in psychiatric colonies. Throughout the years, it was found that
this did not provide the desired therapeutic effects and the colonies
served to occupy the idleness of these subjects, to exclude them and to
chronify them3. By historicizing the social, academic and
cultural practices that favored the institutionalization of mental
suffering as an imperative for care, it is possible to understand the
current situation of care in MH, as well as its emergent processes and
constructors of a theoretical-practical knowledge, aiming at strategies to
overcome the past and transform the future4.
This article aimed to analyze the socio-cognitive reconstruction of MH
professionals about the
chronic psychiatric client, contextualizing with their institutional
permanence and the welfare process.
THEORETICAL FRAMEWORK
Considering that the specific theme is little explored and includes MH
professionals who assist people with mental disorders who aged hospitalized
in psychiatric institutions with asylum characteristics, the structural
approach of the Theory of Social Representations (TSR) has been used to
support this study.
According to this Theory, the social representations (SR) are important in
the everyday life, because they guide people to nominate and to jointly
define the different aspects of the reality, whether in the way individuals
interpret, make decisions, or even position themselves. The SR allows
phenomena to become directly observable or reconstructed by scientific work5.
The central nucleus is the only complementary approach that was constituted
as a theory, allowing the SR to become more heuristic for the social
practice and research6. It focuses on studying the cognitive
contents of representations, conceiving them as a structured, organized set
and not as a mere collection of ideas and values. Around the central
nucleus (CN) the peripheral elements are organized, they are the essential
constituents of the contents of the representations, the more accessible,
the more alive and the more concrete. They have three primary functions:
concretization, regulation and defense functions7.
The TSR was more suitable to understand the question of chronicity in
psychiatry, which runs through the specialties of MH, questioning its
epistemological foundations and its care structures. Chronicity in
psychiatry refers to the evolution of a disease and its duration and
persistence, but also to a social situation that establishes the forms of
care8.
It is emphasized that the care provided in MH advanced the substitutive
devices of the hospital-centered model, and made possible a great
transformation in the national scenario allied to governmental proposals.
However, many clients could not be reinserted in their families and linked
to psychosocial care centers (CAPs - Centros de Atenção Psicossociais),
remaining hospitalized in psychiatric hospitals9.
Silence seems to be the hallmark of chronification, about what little was
said and/or written on subjects with mental disorders who lived or still
live in psychiatric institutions with asylum characteristics2.
The development of this work was important and necessary for a better
understanding of the perspective of the professionals regarding the care
destined to the clientele that has aged in the hospital environment.
METHODOLOGY
It is a scientific research concerning the SR of MH professionals about
people in PD, which are called psychiatric patients. For the construction
of the methodological design, the methodological contributions of the TSR,
in its structural approach, have been used.
The research was carried out in 2013 in two public psychiatric hospitals in
the city of Rio de Janeiro - Brazil. Such a choice was made by the fact
that both scenarios were created at the beginning of the last century to
receive the so-called chronic, which, at that time, were presented as an
impasse to emerging psychiatry. For ethical reasons, their names were kept
confidential. The participants of the research were 159 health
professionals, working in the MH hospital network. The total number of
participants was defined by the following criteria: intentional convenience
sample and minimum parameters adopted for statistical analysis.
Through the technique of free evocations, we sought to apprehend the
perception of reality from a pre-existing semantic composition, a
composition that is usually not only concrete but also imagistic, organized
around some simple symbolic elements. In this sense, the practical
application of the test consisted in asking the participants to associate
other words, freely and quickly, from the hearing or visualization of
inductive words7 or expressions, which, in the present study,
was a chronic psychiatric patient. Then, they were asked to give
an order to the words that have been evoked. This allowed us to analyze the
correlations between the enunciations. It is important to highlight that
the adoption of the expression chronic psychiatric patient, was
only used because it is part of common sense. In view of the efforts of
different MH actors in not classifying as patients the people in PD.
In the treatment of the data produced, the software Ensemble de Programmes Permettant L'analyse des Évocations (EVOC),
version 2003 was used, which makes it possible to organize the words
produced as a function of the implicit hierarchy to the combination of
frequency and the natural order of evocation. The technique of analysis
consists in the construction of a four-house table, through which the
evoked words are distributed, considering the criteria of higher
frequencies and Average Evocation Order (AEO)2.
In addition to the analysis performed by the four-house table, the
similarity analysis8, was also performed, from the co-occurrence
of the words produced by the participants, with the quantification of their
frequencies, generating an index of similarity. The result of this sequence
is the construction of a similarity matrix, through which one obtains the
similarity indexes for each pair of words, indicating the strength of the
connections established between them.
The strength of the links between the categories is expressed by a graphic
image, called tree of similitude, which reveals the links between all the
categories produced based on EVOC. The tree was constructed from the words
that had, among themselves, the highest indexes of similarity. It is
emphasized that a maximum tree cannot, according to the graph theory, form
a cycle, and if this occurs during its construction, the relation should be
ignored, and the next connection should be found7,8.
Thus, all the precepts and guidelines of the study period, defined by the
Resolution number 466/2012 of the National Health Council, were followed.
The project was approved by the Research Ethics Committee- Human Councils
of the Municipal Institute Philippe Pinel, under the Opinion No. 53/2010,
and by the Research Ethics Committee of the Municipal Institute of Health
Care Juliano Moreira, under the Opinion No. 13/2009, both linked to the
Superintendence of Municipal Institutes of the Sub-Secretariat of Hospital
Support, Urgency and Emergency. All the participants signed a Free and
Informed Consent Form.
RESULTS AND DISCUSSION
The results were organized to explain the socio-cognitive reconstruction of
the chronic psychiatric patient through the related inductive
expression that is the proper representational object of the study. For a
better understanding of the representational structure, five dimensions
have been created that relate to each other, understood by imaginary,
positive affectivity, institutional care, mixed affection and need.
The results highlighted the SR structure of the health professionals
participating in the study, generated from the evocations referring to the
inductive expression. Thus, 795 words were evoked, of which 276 were
different. The minimum frequency was 9, and the words evoked in smaller
numbers were excluded from the composition of the four house-table. Then,
the average frequency was calculated, resulting in a value of 17. The rang, also called AEO, was of 2.99. The four-house table was
elaborated from these parameters. See Figure 1.
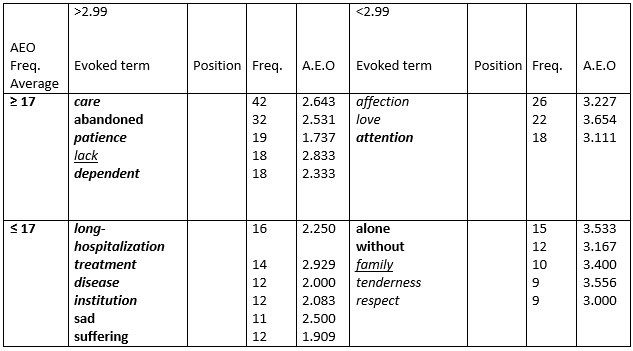
Caption: imagery (Bold); positive affectivity (italics); institutional care
(Bold and italic); mixed affectivity (Underline); need (Underline and
italics).
FIGURE 1: Four-house table referring to the evocation to the inducer term chronic
psychiatric patient. Rio de Janeiro, 2010.
In the upper left quadrant are grouped the words forming the possible
central nucleus (CN)10, composed by the words care, abandoned, patience, lack, and dependent that make
up the imaginary, institutional care and necessity dimensions. It
is notable that the SR of health professionals about the chronic psychiatric patient has in its CN normative and
functional elements. The normative elements are expressed through the
words: lack, dependent and abandoned. These elements are
directly related to the value systems of individuals and their ideologies,
and are related to the social character of the CN of the social
representation5,7. In the specific case of this study, these
elements include the dimensions of institutional care, needs and imaginary.
The results revealed elements of this SR that reinforced the chronicity of
these patients. Aging is an inherent condition of the human nature, but
when this happens in a reclusive way, while hospitalized in institutions
with asylum characteristics, it becomes a disastrous experience when
compared to a regular aging process, in which there are dynamic changes in
the biological, psychological and social environment. Studies indicate that
the institutionalization favors pathological aging, also known as senility,
and it includes senile dementias11,12. The discrimination and
stigmatization, intrinsic to mental disorders, are related to psychological
distress and disability13.
As for the functional elements, they refer to the words patience and care, grouped in the institutional care dimension,
see Figure 1. These elements are related to the descriptive characteristics
and to the insertion of the object in social or operative practices, which
are determinant in the conduct related to the object14. It is
inferred that the words that form the possible CN present, in their
majority, characteristics of negative positions and only two of positive
character. The word care with the highest frequency in the CN,
with AEO of 2, 773 should be highlighted; both indicated a positive
evaluation in the SR of the professionals of MH. The term patience
appeared with low frequency in the CN, AEO of 1,773; both indicated a
positive evaluation in the SR of the MH professionals. Such lexicons
maintain an intimate connection with the clientele that, due to the
advanced age, need care that is consistent with the characteristics of the
elderly person.
Such findings require reflection on what kind of care has been provided to
the elderly population suffering from mental disorders in the current
context of BPR. This is necessary, emphasizing that the reintegration of
people who have gone through long years of hospitalization should not be
tied to charitable or welfare actions. This is not a recent problem
because, since the 1970s, official documents have been elaborated, with
several critiques of the hospital-centered model with asylum
characteristics, which institutions still portray a sad reality in all the
states of the country8.
The lexicon lack obtained AEO of 2.833, having the enunciation lacking, according to Figure 1. The word lack would
express, for mental health professionals, the affective and sentimental
losses that patients had over the years of hospitalization in comprehensive
institutions. In this sense, it is emphasized that, in the care proposals
of the past, the hospitalization was valued and, in parallel, it generated
the stigma on the subject in psychological suffering. In this process, upon
being admitted to a comprehensive institution, the individual was stripped
of their usual appearance, as well as the equipment and services with which
they kept bonds promoting what was called a personal disfigurement15.
As for the institutional care dimension expressed in the CN, which has the
highest number of evoked words, namely dependent (frequency 18 and
AEO 2.333), patience (frequency 19 and AEO 1.737) e care
(frequency 42 and AEO 2.643), see Figure 1. They indicate the care
practices aimed at the chronic psychiatric patient. The long years of
hospitalization generated in this clientele a high degree of institutional
dependence that sometimes interferes in a decisive way with the
deinstitutionalization process.
With the presence of the element dependence in the CN, it can be
inferred that it is closely related to the SR of the MH professional on
this type of client, that is, that of dependence on the services offered ,
which substantially reduces the implementation of actions that can generate
(greater) autonomy and freedom in the institutional everyday life, as well
as the possibility of living outside this environment. At this
moment, it should be questioned if the professional action does not tend to
resemble a charitable and pious act in several situations, in which their
care practices may privilege the stay of the hospitalized patient. Going
back in history is a way of understanding a person's mental production,
which anchors the history of medical practices in psychiatry that privilege
the institutionalization of madness, reinforcing it, even to the detriment
of the autonomy and freedom of the person8.
Contrary to the evocations already described, the word care is
highlighted, belonging to the institutional care dimension, present in the
CN with AEO of 2.64. This word had the highest frequency (42) and is imbued
with values. For the health professionals, there are different forms of
expressing care and to care, and for nursing, they are considered as the
essence of the profession and a genuine and peculiar act16.
Mental health care should be an attitude of accountability1.
Therefore, to take an act like their own is to take responsibility for the
care of the other in an act of mutual surrender. Caring should be
understood as an attitude that goes beyond a moment of attention, zeal, and
care, representing an attitude of occupation, concern, responsibility and
affective involvement with the other17. Broadening this
discussion about care, there is a great tension between care and lack of
care that opposes, on the one hand, the care provided by mental health
professionals, and, on the other hand, the singular demand presented by the
individual in psychic suffering, resulting in two different conceptions of
life and care18.
The imaging dimension of the chronic psychiatric patient is filled
with negative evocations, being highlighted the word disease
linked to the negative character of the dimension. For part of the research
participants, the chronic psychiatric patient would reveal an
image anchored in negative aspects, in accordance with past care proposals,
which privileged the institutionalization and the illness, especially when
valuing the pathology to the detriment of the person in psychic suffering.
In this imaginary, the years of chronifying and exclusionary mental health
care would be present, strongly linked not only to the biological nature of
madness but also to political perspectives of the last century.
Present in the contrast element, the institutional care dimension reflects
the words institution, treatment and long hospitalization
. Negative elements predominate and there is a tenuous relationship with
the imaginary dimension. The word long hospitalization has
revealed a negative and stigmatizing representation. Such evocations could
evidence the lack of perspective on the part of the professionals
concerning the resocialization of these subjects, which configures a
serious impasse to the process of psychosocial rehabilitation. The
evocation treatment points out an ambivalence in relation to the
previous word, meaning an welfare possibility for this clientele, because
it is anchored in the word care, present in the CN.
In the first periphery, the institutional care dimensions (comprising the
word attention) and the affective-positive word (sheltering the
words love and affection), more prevalent in this
upper-right quadrant. In the lower right quadrant, the positive elements of
this SR are recorded. Regarding the second periphery, less frequent and
less readily evoked elements are shown, but, like the CN, which has three
dimensions, namely, positive-affectivity represented by the wordsregard and respect; imaginary with the words without and alone; and the dimension of mixed affectivity
with the word family.
For a more in-depth understanding of the SR structure of the chronic psychiatric patient for mental health professionals, the
maximum tree generated by the similitude analysis is represented next. See
Figure 2.
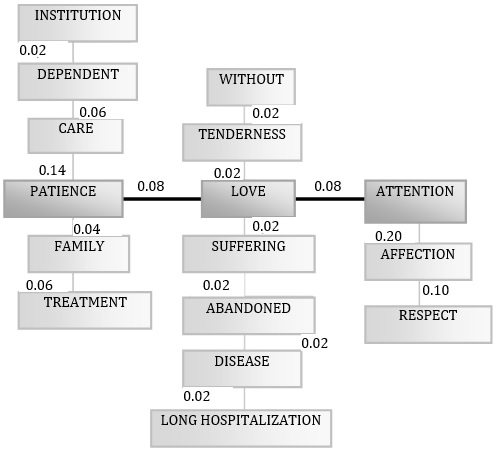
FIGURE 2:
Tree of similarity referring to the inducer term chronic psychiatric
patient.
As it can be seen, the lexicons that are connected horizontally by the
indexes generated by the graphs about the chronic psychiatric patient are patience, love e attention, all of them with indices of similitude
of 0.08, that, from now on, will only be indicated with the placement of
the respective numbers. From these words come out connections of meaning
that will serve as the basis for the understanding of the representational
structure. The strongest link, in its quantitative aspect, was constituted
between the words attention and affection (0.20) and
between affection and respect (0.10). An interesting fact
that should be highlighted is that all these lexicons are present in the
peripheries of the four-house table. This fact seems to indicate that the
peripheral elements have the normative character of the representation
studied, that is, what was politically correct and expected for this group.
See Figure 2.
The words attention, affection and respect express the
sensitivity of the immediate context for the group studied referring to the
chronic psychiatric patient. All these lexicons are present in the
dimension of positive affectivity. Possibly, this representation is
influenced by the physical limitations that the old age and the time of
institutionalization entailed to this clientele, whereas these evocations
express actions that the care proposals of the past did not allow. In an
exclusionary perspective, tempered by the asylum proposals, the client in
psychic suffering was deprived of attention, of affection and of respect.
The paradigm that understands madness as synonymous with incapacity and
danger, justifying tutelage and exclusion must be broken. The rupture with
a paradigm that does not recognize the singularities and therefore does not
tolerate the autonomy and, thus being, stigmatizes and excludes different
positions19.
It is observed that the lexicon love possesses the largest number
of connections (6), however, it does not express high similarity indexes
(0.02). Is possible to infer that love is in the center of a first
line of irradiation of meaning and defense of this possible nucleus. This
lexicon is part of the dimension of positive affectivity and is present in
the first periphery of the quadrant of four houses. Although love
is a positive element, it is possible to observe, in the tree of
similarity, that the graphs derived from it have negative traits, such as suffering, abandoned, disease and long hospitalization.
The practices of hospitalization in the past have designated a new
relationship of the man with that which may be inhuman in his existence.
The sense of hospitalization ended up in an obscure social purpose,
excluding all those who disagree with socially acceptable behavior in
comprehensive institutions3. Such institutions generate in their
inmates a variety of negative feelings. For there is a violation of the
reservation of information about the self, generated in the act of
admission to the institution, followed by the family and affective
abandonment over the years, a fact that further accentuated this deficiency20.
It is interesting to point out the load of meaning existing between these
words, that are almost chained, revealing a representation linked to the
collective image that these professionals have of the chronic psychiatric
patient. The only word with a positive characteristic is tenderness, but then it is linked to a lexicon with a negative
characteristic, without, which aggregates a quantitative of
negative words and expressions, as described above. Also worthy of note is
the lexicon patience, presenting the CN, which, then, is linked to
the word care, which reached the highest frequency (42), also present in
the CN and pointing to a centrality of this term. There are links between
some words present in the CN, such as patience and care,
which was already highlighted and had a strong similarity index (0.14),
followed by dependence (0.06) and institution (0.02).
The lexicon patience forms a triad with the words treatment, present in the contrast elements, and family,
located in the second periphery. Due to the institutionalization and the
serious institutional dependence, this is a clientele that requires more
professional care and consequently requires patience to offer a more
singular care. Precisely, it is the patience that is lacking to many
families that abandoned their relatives in the hospital. Such family
abandonment was justified by past care proposals, which encouraged the
hospitalization and the consequent loss of social bonds and affection.
CONCLUSION
Aspects that would indicate that institutionalized aging could contribute
to chronicity and senility were evidenced, increasing the stigma in
relation to the people. It would justify, in part, the negative and
pejorative character of the SR revealed by the MH professionals, besides
the welfare losses and affective implications implicit therein.
Through the socio-cognitive reconstruction of the MH professionals,
concerning the person in PD, there was a need to reflect on the care
provided to these clients in the context of BPR, since chronicity in
psychiatry has historically been considered as an obstacle to different
care proposals. Madness has haunted the imagination of men due to the fear
of the unknown, the uncontrolled, the foolish and the different.
However, not only the negative aspects made the SR. It revealed that the
professionals' discourse also had positive and affective elements, which
denoted care, a charitable look, which could try to improve the quality of
life of the patients in the everyday life. However, it could not
materialize a daily work towards the deinstitutionalization of this
clientele who have been long hospitalized.
This work did not aim to end the discussion on this topic. In order to
overcome the limitations of this study, it is necessary to replicate the
research in different scenarios of the Brazilian reality, with the
respective health professionals, aiming at the generalization of the
findings. This subject must be discussed in the different environments of
interlocution in MH. Several researches are necessary, and the situation of
the chronic patients must appear in the mental health discussion tables.
REFERENCES
1.Silva LA, Santos I dos, Tavares CMM. Nursing students' imaginary
regarding people with psychological distress: a socio-poetic study. Rev.
enferm. UERJ [online]. 2015 [cited in 2017 Jan 29] 23(4):468-74. Available
from:
http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/18917
2.Silva LA, Gomes AMT, Oliveira DC, Souza MGG. Social representations of
aging in institutionalized psychiatric patients. Esc. Anna Nery Rev.
Enferm. [online]. 2015 [cited in 2017 Jan 29]; 15(1): 124-31. Available
from:
http://dx.doi.org/10.1590/S1414-81452011000100018
3.Foucault M. História da loucura. 8ª ed, São Paulo: Perspectiva; 2008.
4.Silva LA. Perspectiva estética e sociopoética ao cuidar junto com as
pessoas com sofrimento psíquico aplicando a Teoria Tidal Model
[PhD thesis]. Rio de Janeiro: Universidade do Estado do Rio de Janeiro;
2015.
5.Paschoal EP, Santo CCE, Gomes AMT, Santos ÉI, Oliveira DC, Pontes APM.
Adesão à terapia antirretroviral e suas representações para pessoas vivendo
com HIV/AIDS. Esc. Anna Nery Rev. Enferm. [online]. 2014 [cited in 2017 Jan
29]; 18 (1):32-40. Available from:
http://dx.doi.org/10.5935/1414-8145.20140005
6 Jodelet D. Loucuras e representações sociais. Petrópolis (RJ): Vozes;
2005.
7.Costa TL, Oliveira DC, Formozo GA. The health sector in social
representations of HIV/Aids and quality of life of seropositive people.
Esc. Anna Nery Rev. Enferm. [online]. 2015 set [cited in 2017 Jan 29]; 19
(3): 475-83. Available from:
http://dx.doi.org/10.5935/1414-8145.20150063
8.Silva LA. As representações sociais de profissionais de saúde acerca do
paciente psiquiátrico: aspectos descritivos e de zona muda [master degree].
Rio de Janeiro: Universidade do Estado do Rio de Janeiro; 2011.
9.Santos I, Silva LA. Vulnerability of HIV/AIDS in patients with mental
disorders: an integrative review. Online braz.j. nurs [Internet]. 2013
[cited in 2017 Jan 29]; 12 (2): 393-410. Available from:
http://dx.doi.org/10.5935/1676-4285.20133868
10. Sá CP. Núcleo central das representações sociais. Petrópolis (RJ):
Vozes;1996.
11.Falcao DVS, Carvalho IS. Idosos e saúde mental: demandas e desafios. In:
Falcao DVS, Araujo LF, (organizadores.). Idosos e saúde mental. Campinas
(SP): Papirus; 2010. p. 11-32.
12.Santos I, Guerra R, Silva LA. Individuals and clinics characteristics of
elderly people with diabetes: thematic research in sociopoetic workshop.
Rev.enferm. UERJ. [Internet] 2013 [cited in 2017 Jan 30]; 21(1). Available
from:
http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/6344
3.Santos I, Guerra R, Silva LA. Categories of self-care among older adults
with diabetes: a sociopoetic study. Rev. enferm. UERJ. [Internet] 2015.
[cited in 2017 Jan 30]; 23(2):216-21. Available from:
http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/16498
.
14.Abric JC. A zona muda das representações sociais. In: Oliveira DC,
Campos PHF. Representações sociais: uma teoria sem fronteiras. Rio de
Janeiro: Museu da República; 2005. p. 23-34.
15.Goffman E. Manicômios, prisões e conventos. São Paulo : Perspectiva;
2015.
16.Brandão ES, Santos I, Lanzillotti RS, Ferreira AM, Gamba MA,
Azulay-Abulafia L. Nursing diagnoses in patients with immune-bullous
dermatosis. Rev. latino-am enfermagem [Internet]. 2016 [cited in 2017 Jan
29]; 24: e 2766. Available from:
http://dx.doi.org/10.1590/1518-8345.0424.2766
17.Santos-Filho SB, Barros MEB, (organizadores.). Trabalhador da saúde:
muito prazer! Protagonismo dos trabalhadores na gestão do trabalho em
saúde. Ijuí, (RS): Ed. Unijuí; 2007.
18.Loyola CMD. Cuidado continuado. In: Giovanella L, organizadora.
Políticas e sistemas de saúde no Brasil. Rio de Janeiro: Ed. Fiocruz; 2008
p. 1089-110.
19.Boarini ML. O psicólogo e a desinstitucionalização. In: Boarini ML,
organizador. Desafios na atenção à saúde mental. Maringá (PR): Eduem; 2000.
p. 65-78.
20.Delgado PGG. Perspectivas da psiquiatria pós-asilar no Brasil. In:
Tundis AS, Costa NR, organizadores. Cidadania e loucura: políticas de saúde
mental no Brasil. 6th ed., Petrópolis (RJ): Vozes; 2000.
p.171-202.