ORIGINAL RESEARCH
Occupational stress and burnout in nurses of an emergency service: the organization of work
Elias Barbosa de OliveiraI; Cristiane H GallaschII; Pedro Paulo Alves da Silva JuniorIII; Alexia Vidal Rodrigues OliveiraIV; Raphael Lopes ValérioV; Lucas Barbosa Santos DiasVI
I
Nurse. PhD. Associate Professor. Universidade do Estado do Rio de Janeiro.
Brazil. E-mail: eliaBSo@oi.com.br
II
Nurse. PhD. Assistant Professor. Universidade do Estado do Rio de Janeiro.
Brazil. E-mail:
cristiane.gallasch@gmail.com
III
Nurse. Professor. Santa Marta Nursing Course. Rio de Janeiro. Brazil.
E-mail:apedropaulo@hotmail.com
IV
Nurse. Intensive Care Specialist. Álvaro Ramos Municipal Health Center. Rio
de Janeiro. Brazil. E-mail: lekinha_bella@hotmail.com
V
Nurse. Resident of Cardiology Nursing. University Hospital Pedro Ernesto.
Universidade do Estado do Rio de Janeiro. Brazil. E-mail: raphael_rlv@hotmail.com
VI
Nurse. Resident of Mental Health Nursing. State Health Secretary.
Universidade do Estado do Rio de Janeiro. Brazil. E-mail: lucaBSsantos94@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2017.28842
ABSTRACT
Objective: to analyze the dimensions of Burnout Syndrome in nurses of an emergency service. Methods: a descriptive cross-sectional survey was performed with 37 nurses of an emergency service in Rio de Janeiro city in 2014. The sample was characterized using a structured form, and Burnout Syndrome was investigated against the Maslach Burnout Inventory (MBI). The project was approved by the research ethics committee (CAAE: 26913114.0.0000). Results: the sample was primarily female, single, in more than one employment relationship, and working shifts. Suspected burnout was identified by high scores on the emotional exhaustion subscale (19; 51.3%) on the depersonalization subscale (24; 64.9%). On the professional achievement subscale the predominant scores were moderate to high. Conclusion: it is important to evaluate the dimensions of Burnout Syndrome, because its appearance means illness, and declining productivity and quality of care provided.
Keywords: Professional exhaustion; nursing team; worker's health; emergency service.
INTRODUCTION
There is a growing concern regarding the inadequate working conditions of nursing in hospitals, which attracts the attention of researchers due to the risks that this environment offers, together with the performance of special care activities for patients with different health problems.
These professionals should continuously participate in the identification of existing problems in the occupational environment, as well as recognize the stressors of the profession1. Dealing with patient pain, suffering and death is an inherent part of the professional experience of caring, which implies constant emotional tension, attention and great responsibility to each gesture, which can affect the health of the workers and allow the emergence of the Burnout Syndrome (BS)2.
As for the work in the emergency service, there is the possibility of the development of the BS in nurses, due to the existence of psychosocial risk factors that compromise the health and well-being of this portion of workers, among them: overcrowding, labor violence, caring for patients at risk of death, inadequate working conditions in terms of human and material resources, inadequate facilities conditions and the intensification of the pace of work3. Studies that seek to establish the relationship between occupational stress and the worker's health in the emergency services are of great importance, since they help in the planning and in adopting preventive measures that minimize health risks and contribute to the prevention of the BS4.
In order to subsidize the study about the BS with nursing workers who work in the emergency services, a survey of the state of the art in the Virtual Health Library (VHL) has been carried out in an integrated manner with the Nursing Database (NDTB), Latin American and Caribbean Literature in Health Sciences (LACLHS), Medical Literature Analysis and Retrieval System Online (MEDLARSO) and Cumulative Index to Nursing and Allied Health Literature (CINAHL). In the selection of the material, we have worked with the temporal cut from 2012 to 2016, selecting articles published in full and in the native language from the following keywords: emotional exhaustion and nursing; professional exhaustion and nursing; occupational stress and nursing; burnout and nursing.
It was evidenced that, although there is a significant production on Burnout regarding health and education workers, there is a shortage of Burnout studies with nurses who work in emergency situations. It is important to highlight the relevance of the choice of this field, in view of the importance of investigating the labor aspects that may compromise the health of the professional, mainly due to the fact that the nurse is more exposed to the BS due to the demands of care and management.
From what has been mentioned above, in order to contribute to the knowledge about the BS in nursing and to reflect on the aspects related to the prevention of occupational stress and health promotion of workers, the present study had as objective to analyze the dimensions of the Burnout Syndrome in nurses who work in the emergency service.
LITERATURE REVIEW
The professionals who work in emergency services, due to the fact that they take care of serious or potentially serious patients, need a physical, technological and skills structure that favors effective communication between the members of the health team and the solubility of the specific demands of the sector. However, the reality experienced in the emergency sectors of the public hospitals with inadequate working conditions may compromise the nurses' ability to manage conflicts and assist the user 5. This context, the exposure to potentially stressful conditions, the accumulation of functions, and the specificities of the work, can trigger states of stress and, consequently, interfere in the work, health and quality of life of the professional6.
Stress is termed as a state of tension that causes a rupture in the internal balance of the organism, being identified, in its initial phase, through a series of psychosomatic signs and symptoms such as: tachycardia, gastritis, cardiovascular alterations, insomnia and others. By nature, the body always strives for balance, automatically, making a special effort or an adaptive response to establish the anterior homeostasis, thus requiring considerable wear and the use of physical and mental energy reserves 7.
In the work environment, stress is one of the great psychosocial problems that affect the quality of life of the professionals, causing social and economic costs to the organization due to the sickness of the worker, to absenteeism and to the leaves of absence for health treatment1. Workers undergoing high intensity and duration stress and who do not have sufficient adaptive energy to react to stressors, trigger feelings of emotional exhaustion and become vulnerable to the development of the BS 8.
The BS is a prolonged state of stress, which produces many different consequences for the person, such as alienation, indifference, and demotivation. The syndrome involves three dimensions: emotional exhaustion - wear or loss of the emotional resources; depersonalization - development of negative feelings and attitudes at work; decrease in personal achievement at work with a tendency towards negative self-evaluation 9,10.
In the development of the BS, the combination of organizational factors (physical and social environment of organizations, institutional norms, communication, autonomy, rewards, safety, type of occupation, profession duration and institution, work shift, overload, and the type of clientele attended), and sociodemographic characteristics that, although not considered as triggers of the BS, can act as facilitators or inhibitors of stressors2.
METHODOLOGY
This is a descriptive quantitative cross-sectional study that aims at describing the dimensions involved in the BS in nurses within a certain period of time, for an initial diagnosis of the situation. The field of study was an emergency service of a large federal public hospital with 296 beds, located in Rio de Janeiro (RJ). The physical facilities of the emergency service (adult and child) are divided into 12 service areas; the nursing service being composed of 47 nurses and 188 nursing technicians working on a shifts regimen (day and night), and on a part-time regimen (morning or afternoon).
The study began after the approval of the project by the ethics committee (CAAE: 26913114.0.0000), in compliance with the provisions of the Resolution No. 466/2012 of the National Health Council for research involving human beings.
The sample, structured by convenience or spontaneous demand, consisted of nurses with statutory and/or contractual type of employment, and who have been practicing their work activities in the emergency room for at least one year, time considered relevant in terms of knowledge, skills and construction of mechanisms to cope with labor stressors. Nurses on vacation, leave of absence (health, maternity, and others), and those who worked for less than a year in the service have been excluded. Those who agreed to participate in the study have signed the free and informed consent form, after the invitation and explanations about the objectives and methodological procedures.
According to the eligibility criteria of the study, the data collection occurred in the workplace from August to September 2014, according to the availability of the participants. The self-administered questionnaire consisted of two parts, the first with questions for the survey of some sociodemographic and occupational variables, and the second comprised the questions of the Maslach Burnout Inventory (MBI) version Human Services Survey (HSS) elaborated by Cristina Maslach and Susan Jackson in 1981. This instrument is used for the healthcare or human-social service areas, having been translated and validated into the Portuguese language, obtaining an internal consistency of 0.90 in emotional exhaustion, 0.79 in depersonalization and 0.71 in professional achievement through the Cronbach's Alpha and convergent validation9.
The MBI-HSS consists of 22 items, distributed in three domains in the form of statements to be answered on a Likert-type scale, with an extension of six possibilities, going from never (0) to every day (5), and that assess three dimensions: emotional exhaustion (nine affirmations), depersonalization (five affirmations) and professional achievement (eight affirmations).
The scoring in each sub-scale was obtained by summing the values of the respective sub-scales. For this, the cut-off points of another study have been used, in which the authors considered that, in the emotional wear (EW) sub-scale, a score greater than 21 is indicative of a high level of wear; the range from 11 to 21 would correspond to average values; values that are equal to or less than 10 would indicate a low level. In the sub-scale depersonalization (DE), score greater than 8 would be indicative of a high level; between 3 and 8, moderate; less than or equal to 2, a low level of depersonalization. The sub-scale professional achievement (PA) also presents three measures, so the high level corresponds to values equal to or higher than 27, the average level is from 21 to 27, and values as low as 20 indicate a low level of professional achievement9. This sub-scale expresses inverse evaluation meanings for the others, that is, the higher the PR, the lower the EW and the DE scores.
The information from the instruments answered was coded, typed and processed on a Microsoft Excel® spreadsheet. All the results have been analyzed through the descriptive statistics of the data (relative and absolute frequencies), and presented in the form of tables.
RESULTS E DISCUSSION
Sample profile
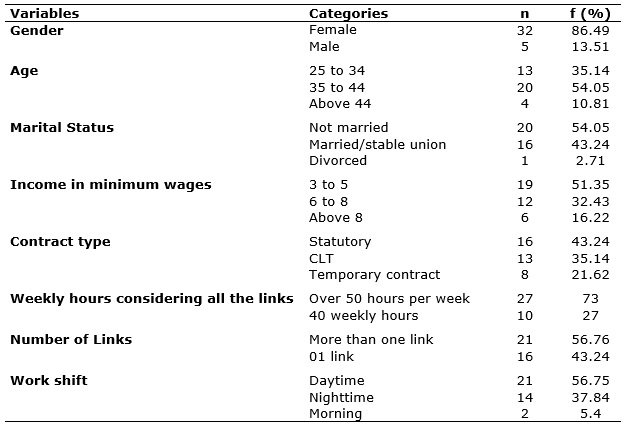
Of the 47 nurses allocated at the emergency room, 37 (78.7%) accepted spontaneous participation in the study. The sociodemographic and labor characteristics of these professionals are described in Table 1.
TABLE 1:
Socio-demographic and work characteristics of emergency service nurses. Rio
de Janeiro, 2014. (N=37)
The nurses are mostly female - 32 (86.49%). According to the survey, which outlined the profile of nursing in Brazil, 85.1% of the professionals are female, being increasing the number of men in the area, who account for 14.4% of the total11. The women, because they have to reconcile the work day with the domestic tasks, are the ones that present greater commitment in relation to the sleep, leisure and rest, being more exposed to the chronic fatigue12.
The highest concentration of professionals - a total of 20 (54.05%) - in the age range of 35 to 44 is in line with the research carried out in nursing, which has shown that it is a category composed mainly of young adults, who are at their productive and reproductive power1. However, young adults are more likely to develop the BS because of risk factors such as insecurity, poor work experience and performance charges, which contribute to increased stress in decision-making situations. On the other hand, it is postulated that the more experienced the professional, the more self-confidence they have and the less their physical and emotional exhaustion will be before the stressors2,7,8.
Regarding their marital status, it was evidenced that 20 (54.06%) nurses were single and 16 (43.2%) were married, according to Table 1. The single individual is more likely to develop the BS, unlike married couples who, although they also experience the same stress situations, have greater resistance to the syndrome, obtained in the family because it is an important support network in coping with stressful situations 2,12. However, single people have a lower incidence of emotional exhaustion than married couples, who have to reconcile work with family life, commitment to child raising and other social activities2,8 .
Concerning the family income, 19 (51.35%) nurses have reported receiving three to five minimum wages in force when the data was collected, due to the fact that 21 (56.76%) workers reported having more than one job. Given the low salaries received by the health professionals in the country, and considering the right of nurses to accumulate up to 62.5 hours per week, the problem of double employment and the resultant work of the night shift, long hours and little time for entertainment, self-care and coexistence with the family continue12,13.
A survey with 2279 nurses, who worked in 18 public hospitals in the country, showed that the female group presented more extensive work hours due to domestic activities when compared to the male group. The results highlight the need for actions to promote health and the importance of evaluating the impact of long hours on workers' health14. Nurses perform weekly work that is longer than 44 hours a week, undergoing different workloads that generate processes of attrition and illness, compromising their health and the quality of care15.
Regarding the type of contract, 16 (43.24%) nurses are statutory, 13 (35.14%) are CLT and 8 (21.62%) are temporary, as shown in Table 1. These results reinforce the process of precariousness of the nursing workforce due to the lack of public tenders to make up the permanent staff in the country's health institutions, and the BS is more incident in the personnel that have a CLT and a temporary type contract, due to insecurity, loss of labor rights and fear of unemployment2.
More than one million (58.9%) of nursing workers work in the public sector with various employment relationships. In the municipal sphere, the majority (42%) is composed of statutory, 18.5% are CLT, and 7.2% are temporary, showing the scenario of precarious work in the health sector 12. As a consequence, there are damages to the health of the worker and to the organization, due to the turnover of personnel and the absence of intellectual capital with interference in the quality of the assistance13. Gradually, the difficulty of reconciling two jobs becomes evident, since, in the hospital context where nursing is the largest work force, activities are often complex, in addition to a rigid hierarchical structure for meeting schedules, routines, norms and regulations1,11,14.
Regarding the working hours, considering the two links, it was evidenced that 27 (72.97%) workers have a work load of more than 50 hours per week, being the physical and mental intensification due to displacements, night shifts and difficult conciliation with the domestic activities, leisure and healthcare. The emergency work, by its own characteristics, requires a quick decision making and a higher level of concentration, due to the care given to patients at risk of complications and death, with a greater possibility of the worker experiencing emotional exhaustion2,4,5 .
Due to the fact that the emergency service operates uninterruptedly, one of the characteristics of the organization is shift work, as shown in Table 1, in which 14 (37.84%) nurses are allocated to the nighttime service and 21 (56.76%) are assigned to the daytime service. The nighttime work, by reversing the circadian cycle, causes health problems, restricts leisure activities and care for one's own health1,11,14. In the general hospital, the emergency sector is the work environment where there is a higher incidence of nurses' leave of absence due to health problems, since it is an occupational environment characterized by stress situations - due to the coexistence with pain, suffering, death and accidents; marked by long journeys, repetitive work and a reduced number of workers16 .
Verification of the BS suspicion in the sample: analysis of the scores/MBI-HSS
Nursing is a profession considered as a vital and indispensable component in the healthcare services, because it provides continuous care to patients, with varying degrees of complexity, which requires technical and relational knowledge. However, the professional activity, depending on the workload and the risk factors involved, can contribute to the development of the BS, and it is important to study the stress levels that affect nurses in order to identify and/or prevent illness2,8,13,15. It is assumed that the existence of an expressive number of suffering nurses, when not characterized as a result of the work activity, can contribute to the depreciation of the activity, since these workers can be identified by the clientele and other colleagues as bad professionals, cold, and indifferent to the human suffering17,18.
The results obtained with the application of the MBI-HSS instrument in the sample showed that 19 (51.3%) individuals presented high emotional wear, with scores ranging from 22 to 40; 12 (32.4%) with average wear, with scores that ranged from 11 to 20; and 6 (16.2%) with low wear, with scores ranging from 4 to 10, as described in Table 2.
TABLE 2:
Distribution of sub-scale sample scores according to the MBI-HSS. Rio de
Janeiro, 2014. (n=37)
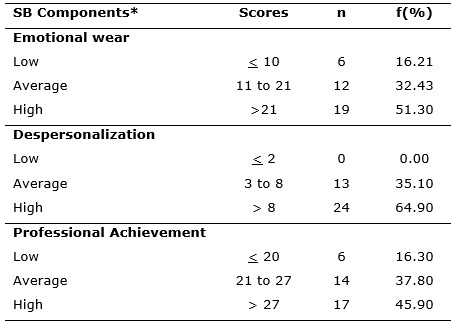
*SB = Burnout Sindrome
Regarding the depersonalization, it has been observed that 24 (64.9%) individuals presented high scores for this event, 13 (35.1%) had an average level for the event, and low scores were not found, as verified in Table 2.
It is possible to infer that the high and average scores for emotional wear and depersonalization can have causal nexus with some stressors or risk factors, since nurses, in most of the cases 27 (73%), have reported having a double employment relationship, working over 50 hours a week with little spare time for rest. The emotional wear is considered the initial trait of the BS, and its manifestation may be physical, psychic, or a combination of both. The syndrome affects health and education workers who develop relationships or provide continuous care to people, and the professional can be unmotivated, not understanding, with distant and dehumanized treatment, blaming those who need their attention/care for their own problems2,8,9,10.
The depersonalization occurs in the circumstances in which the professional presents a negative behavior, being accompanied by anxiety, irritability, demotivation, reduction of the work goals, conflicts with the team and leadership. One of the coping mechanisms used by the individuals affected in this dimension is the detachment of their clientele and denial of feelings1.
A survey with 130 nursing professionals working in the intensive care unit and coronary care unit showed average values for emotional wear (24.5 points), depersonalization (9.0 points) and high professional achievement (30.3 points), due to the reverse score. The BS suspicion was significant in 53 (72%) workers, which revealed the influence of the organization and the nature of the work on these results19. In another study with high-complexity hospital nurses, in the high emotional wear category there are 22.4% (quartile) and 33.3% (tertile)20.
As for emergency work, this has the following characteristics: the unpredictability of the clinical picture of patients under the care of the team; to be an open service and there is the problem of overcrowding. Other risk factors should be considered in the genesis of stress, such as violence at work and role ambiguity, in which the nurse has to expand to meet a number of technical and managerial demands3.
Regarding the professional achievement, Table 2 shows that 17 (45.9%) individuals presented high scores ranging from 28 to 35, with an average of 31; 14 (37.8%) had an average score ranging from 21 to 27, with an average of 24; and 6 (16.3%) had low scores, with scores ranging from 1 to 15, and an average of 13. Considering that most of the sample showed predictive symptoms of emotional wear and depersonalization, special attention should be given to the fact that 6 (16.3%) professionals had low scores in this sub-scale that, because of the reverse, there is a suspicion of Burnout in this group of workers. For the suspected BS, it is necessary to obtain superior cut-off points, at least for two dimensions that characterize it. In isolation, each domain also presents valuable information about the situation of the sample studied9.
As verified, 17 (45.9) nurses presented high scores in the professional achievement sub-scale. This result may be anchored in the professional's perception regarding the usefulness of their work, which is invaluable for their self-esteem18. On the other hand, feelings of low self-esteem, dissatisfaction with their activities and lack of motivation often cause the desire to leave the profession, being the low accomplishment with work a predictor symptom of great relevance in terms of the BS suspicion2.
Some symbolic rewards at work can contribute to the professional achievement and act as minimizing factors for the BS development, such as the fact that professionals feel personally and professionally gratified. The professionals also voiced the proud feeling of working in the hospital due to the positive image of the institution, in addition to being an international reference in the treatment of childhood cancer21. Therefore, the professional achievement is a protective factor, which can contribute to a greater involvement of the professional with the work and have a positive impact on the decrease of the absenteeism index, improvement of productivity and quality of the service offered8.
CONCLUSION
Although the study did not aim at verifying the prevalence of the BS and the statistical association with the characteristics of the sample, the influence of stressors in the emergency department should be considered in the development of the Syndrome, the socio-demographic and professional variables of the participants. The sample consisted mostly of female professionals who accumulate two employment relationships, who work on shifts, work more than 50 hours a week, with time restriction for rest, self-care, leisure and coexistence with the family, and domestic work is an aggravating factor of stress.
There were high scores for the sub-scales emotional wear and depersonalization in a significant portion of the sample. Therefore, the BS is suspected in the group, considering the characteristics of the participants and the exposure to stressors in the emergency department. As the Burnout Syndrome results from chronic stress at work, it is suggested to adopt preventive measures and health promotion, considering the impact of the BS on the health of the worker due to the wear and diseases. Investing in such measures can minimize problems such as absenteeism, declining productivity and quality of the service.
REFERENCES
1.Meneghini F, Paz AA, Lautert L. Fatores ocupacionais associados aos componentes da Síndrome de Burnout em trabalhadores de enfermagem. Rev Texto Contexto Enfermagem [serial on the internet] 2011 [cited on Feb 02, 2017]; 20(2): 225-33. Available on: http://www.redalyc.org/articulo.oa?id=71419104002
2.França FM, Ferrari R. Síndrome de Burnout e os aspectos sociodemográficos em profissionais de enfermagem. Acta paul enferm [serial on the internet] 2012 [cited on Apr 14, 2017]; 25(5):743-8. Available on: http://www.scielo.br/scielo.php?pid=S0103-21002012000500015&script=sci_arttext
3.Oliveira EB, Andrade JB, Pinel JS, Diniz DB. Trabalho de Enfermagem em emergência hospitalar - riscos psicossociais: pesquisa descritiva. Online Brazilian Journal of Nursing [serial on the internet] 2013 [cited on Feb 02, 2017]; 12(1):73-88. Available on: http://www.objnursing.uff.br/index.php/nursing/article/view/4046/html_2
4.Fernandes MA, Sousa FK, Santos JS, Rodrigues JA, Marziale MHP. Burnout syndrome in nursing professional of emergency medical care service. R pesq cuid fundam online [serial on the internet] 2012 [cited on Jan 12, 2017]; 4(4):3125-35. Available on: http://www.seer.unirio.br/index.php/cuidadofundamental/article/view/1900
5.Pereira DS, Araújo TSSL, Gois CFL, Gois Junior JP, Rodriguez EOL, Santos V. Estressores laborais entre enfermeiros que trabalham em unidades de emergência. Rev Gaúcha Enferm [serial on the internet] 2013 [cited on Feb 02, 2017]; 34(4):55-61 Available on: http://www.scielo.br/pdf/rgenf/v35n1/pt_1983-1447-rgenf-35-01-00055.pdf
6.Martins JT, Bobroff MCC, Andrade NA. Equipe de enfermagem de emergência: riscos ocupacionais e medidas de autoproteção. Revenferm UERJ [serial on the internet] 2014 [cited on Feb 14, 2017]; 22(3):334-40. Available on: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/13690
7.Lipp MEN. Manual do Inventário de Sintomas de Stress para Adultos de Lipp (ISSL). 3ª ed. São Paulo: Casa do Psicólogo; 2005.
8.Galindo RH, Feliciano KVO, Lima RAS, Souza AI. Burnout Syndrome among General Hospital Nurses in Recife. Revescenferm USP [serial on the internet] 2012 [cited on Nov 03, 2016]; 46(2): 420-7. Available on: http://www.scielo.br/pdf/reeusp/v46n2/a21v46n2.pdf
9.Benevides-Pereira AMT. Burnout: quando o trabalho ameaça a vida do trabalhador. 3ª Ed. São Paulo (SP): Casa do Psicólogo; 2010.
10.Moreira DS, Magnago RF, Sakaê TM, Magajeswki FRL. Prevalência da Síndrome de Burnout em trabalhadores de enfermagem de um hospital de grande porte da Região Sul do Brasil.Cad Saúde Pública [serial on the internet] 2009 [cited on Jan 02, 2017]; 25(7): 1559-68. Available on: http://www.scielosp.org/pdf/csp/v25n7/14.pdf
11.Machado MH, Oliveira E, Lemos W, Lacerda WF, Filho Wilson A, Wermelinger M et al. Mercado de trabalho da enfermagem: aspectos gerais.Enferm Foco [serial on the internet] 2016 [cited on Jan 02, 2017]; 7(esp):35-62. Available on: http://revista.portalcofen.gov.br/index.php/enfermagem/article/view/691/301
12.Narciso FV, Pinto MCR. O trabalhador em turno e noturno na sociedade moderna. In: Mello MT. Trabalhador em Turno: Fadiga. São Paulo: Atheneu, 2013. p. 1-9.
13.Oliveira EB, Barros PM, Perez Junior EF, Granadeiro DS, Xavier T, Rossone FO. Precarização do trabalho em serviço de emergência e dimensionamento de pessoal: um desafio para a gerência de enfermagem e a qualidade do serviço. In: Programa de atualização em enfermagem. Unicovsky MA, Waldman BF, Spezani RS (organizadores). Porto Alegre: Artmed Panamericana Editora; 2016.
14.Fernandes JC, Portela LF, Rotenberg L, Griep RH. Jornada de trabalho e comportamentos de saúde entre enfermeiros de hospitais públicos. Rev Latino-Am Enfermagem [serial on the internet] 2013 [cited on Jan 02, 2017]; 21(5) [08 telas]. Available on: http://www.scielo.br/pdf/rlae/v21n5/pt_0104-1169-rlae-21-05-1104.pdf
15.Martins PF, Sobrinho CLN, Silva MV, Pereira NB, Gonçalves CM, Rebouças BS et al. Afastamento por doença entre trabalhadores de saúde em um hospital público do estado da Bahia. Rev bras Saúde ocup [serial on the internet] 2009 [cited on Feb 22, 2017]; 34(120):172-8. Available on: http://www.scielo.br/pdf/rbso/v34n120/08v34n120.pdf
16.Felli VEA. Condições de trabalho de enfermagem e adoecimento: motivos para a redução da jornada de trabalho para 30 horas. Rev enferm em foco [serial on the internet] 2012 [cited on Feb 22, 2017]; 3(4):178-81. Available on: http://revista.portalcofen.gov.br/index.php/enfermagem/article/viewFile/379/170
17.Lorenz VR, Benatti MCC, Sabino MO. Burnout e estresse em enfermeiros de um hospital universitário de alta complexidade. Rev Latino-amenferm [serial on the internet] 2012 [cited on Feb 08, 2017]; 18(6): 8 telas. Available on: http://www.scielo.br/pdf/rlae/v18n6/pt_07
18.Kestenberg CCF, Felipe ICV, Rossone FO, Delphim LM, Teotonio MC. O estresse do trabalhador de enfermagem: estudo em diferentes unidades de um hospital universitário. Rev enferm UERJ [serial on the internet] 2015 [cited on Jan 13, 2017]; 23(1): 45-51. Available on: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/11487/12326
19.França FM, Ferrari R, Ferrari DC, Alves ED.Burnout e os aspectos laborais na equipe de enfermagem de dois hospitais de médio porte. Rev Latino-amenferm [serial on the internet] 2012 [cited on Jan 13, 2017]; 20(5):8 telas. Available on: http://www.scielo.br/pdf/rlae/v20n5/pt_19.pdf
20.Silva JLL, Soares RS, Costa FS, Ramos DS, Lima FB, Teixeira LR. Fatores psicossociais e prevalência da Síndrome de Burnout entre trabalhadores de enfermagem intensivistas. Rev Bras Ter Intensiva [serial on the internet] 2015 [cited on Jan 17, 2017]; 27(2):125-33. Available on: http://www.scielo.br/pdf/rbti/v27n2/0103-507X-rbti-27-02-0125.pdf
21.Zanatta AB, Lucca SR. Prevalência da Síndrome de Burnout em profissionais da saúde de um hospital oncohematológico infantil. Rev Enferm USP [serial on the internet] 2015 [cited on Jan 04, 2017]; 49(2):253-60. Available on: http://www.scielo.br/pdf/reeusp/v49n2/pt_0080-6234-reeusp-49-02-0253.pdf