Legend: SA=Sensory Abilities; AUT=Autonomy; PPF= Past, Present and Future Activities.
ORIGINAL RESEARCH
Comparing the quality of life of institutionalized and non-institutionalized older adults
Matheus Figueiredo NogueiraI; Anderson Araújo LimaII; Janaína von Söhsten TrigueiroIII; Isolda Maria Barros TorquatoIV; Maria Emília Roméro de Miranda HenriquesV; Maria do Socorro Costa Feitosa AlvesVI
I
PhD Professor in Nursing. Federal University of Campina Grande. Cuité,
Paraíba, Brazil. E-mail:
matheusnogueira.ufcg@gmail.com
II
Graduated in Nursing. Federal University of Campina Grande. Cuité, Paraíba,
Brazil. E-mail: andersondez@gmail.com
III
Master Professor in Nursing. Federal University of Campina Grande. Cuité,
Paraíba, Brazil. E-mail: janavs_23@hotmail.com
IV
Master Professor in Nursing. Federal University of Campina Grande. Cuité,
Paraíba, Brazil. E-mail: isoldatorquato@ig.com.br
V
Professor of the Department of Nursing. Federal University of Paraíba. João
Pessoa, Paraíba, Brazil. E-mail:
mmilahenriques@yahoo.com.br
VI
Professor of the Department of Dentistry. Federal University of Rio Grande
do Norte. Natal, Rio Grande do Norte, Brazil. E-mail: socorrocfa@hotmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2016.28185
ABSTRACT
Objective: to evaluate comparatively the quality of life of institutionalized and non-institutionalized older adults. Method: observational study conducted in Cuité, Paraíba, with a sample of 40 older adults divided equally between the two categories. Data were collected using the World Health Organization Quality of Life Assessment for Older Adults (WHOQOL-Old) questionnaire and analyzed using descriptive statistics, after approval by the Research Ethics Committee (CAAE 09871412.0.0000.5188). Results: the non-institutionalized older adults showed greater satisfaction in five areas: sensory functioning, autonomy, past, present and future activities, social participation, and intimacy; the only exception being in relation to death and dying. Conclusion : it is necessary to implement effective public policies in favor of better levels of quality of life for the elderly, especially those who are institutionalized, particularly in view of rapid growth in Brazil's elderly population, many of whom live in long-stay institutions.
Keywords: Quality of life; aged; institutionalization; environment.
INTRODUCTION
The growth of the elderly population is a worldwide trend, and in Brazil, the elderly are considered those aged 60 or over1. This change of the demographic pattern in this country is responsible for one of the most important transformations in the structure of society, with the consequence of the increase of the population with old age2. This significant growth occurred due to the influence of several factors, including the expansion of access to health care, socioeconomic improvements, basic sanitation and the emergence of new technologies, both in health and in other areas3.
According to the projections of the World Health Organization (WHO), by 2025 Brazil will have the sixth largest population in the world of elderly people, with a quota of more than 30 million, and this will occur mainly due to the decrease in fertility and mortality rates, resulting in an increase in life expectancy4. Accompanying the phenomenon of aging, there has been a set of isolated and collective biopsychosocial modifications, in which the elderly develop specific clinical-functional and socio-family needs, which generates ample demands in the health system, clearly unprepared for a comprehensive care in the old age5.
Aging happens as the individual's age progresses, being an irreversible, natural and diversified process for each individual. This is a universal and progressive phenomenon, with the consequence of reducing the individuals' capacity to respond to environmental stress and to maintain homeostasis6. As a consequence of the advancing years, the old person's health, lifestyle and perspectives change and dependence tends to increase and often has implications for self-care7, which may require daily professional and family support8, thus making aspects of the quality of life vulnerable.
Therefore, increasing the elderly population's life expectation is not enough, there is need to make this increase parallel to the improvement of the quality of life9. The term Quality of Life (QoL) is subjective and complex to be described, but the most consensual definition is that presented by the World Health Organization Quality of Life Group, which defines it as the individual's perception of life, involving culture and value system where the person is inserted, as well as in relation to one's goals, expectations, standards and concerns10.
The evaluation of QOL is complex, subjective and multidimensional11, and among the elderly it is related to the investigation of individual perception of self-esteem and well-being, involving elements such as lifestyle, health status, physical dependence, functional capacity, socioeconomic level, social interaction, emotional status, intellectual activity, family support, satisfaction with activities performed and living environment. Recognizing that the construct QoL adds different variables and that the social environment of the elderly person is not similar to everyone, since they may live at home with their family, with caregivers or alone, or even institutionalized in nursing homes, an important question arises: is there a difference in the QoL of institutionalized and non-institutionalized elderly?
Considering the subjectivity and breadth of the theme QoL, as well as the limitation of studies that show specific knowledge about the quality of life of elderly people living in different social contexts, especially in small cities, the objective was to compare the quality of life of institutionalized and non-institutionalized elderly people in the municipality of Cuité, state of Paraíba.
LITERATURE REVIEW
Aging is a continuous process of life, which begins from birth until death. Throughout this process, the human organism goes through the stages of development, puberty, maturity and old age, which undergo the action of biological markers that generate transactions and transformations between them. The differentiation between maturity and old age is also associated with psychological, social and economic factors, which, together, determine the development and manifestation of signs characteristic of aging, in different chronological ages and levels of intensity12.
In this perspective, for aging to occur as a positive experience for the individual and for longevity to be a reality, it must be monitored with continuous opportunities for health, participation and safety13. Thus, to express the process of achieving this vision, the WHO adopted the term active aging defined as "the process of optimizing health, participation and safety opportunities with the objective of improving the quality of life as people get older"11:13. It is noted, therefore, that QoL in the elderly refers to the maintenance of health in the biopsychosocial and spiritual aspects, and it should be analyzed in a particular way in each subject, since each one has a proper context of life to which one is inserted14.
Globally, the QoL of the elderly has generated a lot of discussion, as there is now a high concern in maintaining the overall health of these people, so that they can age with dignity. Thus, defining QoL in the elderly is a very complex task, since it involves dimensions such as physical, emotional and family well-being, functional capacity, spirituality, social respect, sexuality and occupation. These factors, when integrated, keep one in balance with oneself and with the environment 15, either the senior is institutionalized or not.
METHODOLOGY
This is an observational study of cross-sectional, quantitative design and comparative nature, carried out with institutionalized and non-institutionalized elderly people in the city of Cuité, state of Paraíba. Specific scenarios were used, such as the Social Assistance Reference Center (CRAS in Portuguese), which develops activities with the elderly group entitled Alegria de Viver (Joy of Living); and the Long Stay Institution for the Elderly - LSIE Casa do Idoso Vó Filomena Maria da Conceição – Asilar.
The sample consisted of 40 elderly people selected by convenience and according to the criterion of accessibility. Of these, 20 were part of the Alegria de viver group, being configured as non-institutionalized and 20 were identified as institutionalized, since they lived in the Asilar. The adopted criteria for the selection of the sample were: aged 60 or over; not having cognitive deficiency as evaluated by the Mental State Examination (MMSE); and having at least 2 years of participation in the group or of living in the LSIE.
Data collection took place in February and March 2013 after approval by the Research Ethics Committee of the Health Sciences Center of the Federal University of Paraíba (CEP/CCS/UFPB) under the opinion No. 202.260, respecting the ethical aspects contained in Resolution No. 466/12 of the National Health Council (CNS/MOH), which regulates research involving human beings16.
To obtain the data, two instruments were used: the socioeconomic and demographic characterization form; and the WHOQOL-Old questionnaire for measuring the quality of life of the elderly, composed of 24 questions covering six specific domains for this population group: Sensory Abilities (SA), Autonomy (AUT), Past, Present and Future Activities (PPF), Social Participation (SOP), Death and Dying (DD) and Intimacy (INT)17. It was emphasized that the instruments were self-applied by the participants with the intervention of the researchers regarding the orientation about filling.
After the results were grouped in the Microsoft Office Excel 2010 program, the analysis of the WHOQOL-Old findings was performed according to descriptive statistics and considering the separation by domains. The response of each item of the questionnaire registered on a Likert scale was coded by the respective score (1 = 1, 2 = 2, 3 = 3, 4 = 4 and 5 = 5) and then each score was multiplied by the number of answers. According to the WHOQOL-Old scalar proposal, the variability of the responses range from nothing/very unsatisfied/very poor, corresponding to 1 point, up to fully/extremely/very satisfied/very good that equals 5 points, with the intermediate options 2, 3 and 4. Thus, the higher the score obtained, the better the QoL, except for questions 1, 2, 6, 7, 8, 9, and 10, in which the reverse score was applied (1 = 5, 2 = 4, 3 = 3, 4 = 2 and 5 = 1), indicating a better QoL for the lowest score17. The values found in each domain were summed and the relative frequency (%) was calculated, allowing the comparative evaluation of the quality of life among institutionalized and non-institutionalized elders.
RESULTS AND DISCUSSION
With regard to the socioeconomic and demographic characterization of the participants, a large proportion of institutionalized elderly people were over 80 years of age (40%), male (55%), single (50%), had incomplete primary education (60%) and had income of up to 01 (one) minimum salary (100%). As for the non-institutionalized elderly, the majority were in the age range of 60 to 69 years (65%), were female (85%), married (65%), had incomplete primary education (65%) and had income between 1 and 2 minimum wages (50%).
The elderly, once institutionalized, advance in the age inside the institution, where they receive minimal health care, which can reflect in the increase of life expectancy. On the contrary, older people tend to be active in the participation of groups, as observed in the results. The predominance of the female gender was observed, emphasizing that the non-institutionalized women follow the trend of the feminization of aging, which is equivalent to greater longevity of the female population 18.
In the institutionalized group there was a high number of singles. This fact can be justified by their situation of institutionalization, since many do not have children or close relatives to take care of them. Regarding the marital status of the non-institutionalized elderly, the married ones stood out, revealing the importance of formalizing an affective union and having children, which allows inferring that the construction of an integrated family in society reduces the possibility of institutionalization.
In the educational level, the absence and/or low level of education was observed in the majority of the participants, related mainly to the lack of access to schools throughout the life trajectory, given the reality of that time, which consolidates the concern with the educational trajectory of the Brazilian population. These results corroborate data from the Brazilian Institute of Geography and Statistics (2010 Census), whose findings show that 39.2% of the country's non-literate population is from seniors 19. Low levels of education and worse socioeconomic conditions are associated with higher incidence of health problems, greater risks of disability and death13. As a consequence, low levels of education reflect directly and negatively in the quality of life domains of these people.
Considering that the average individual income of the participants was one minimum wage, mainly coming from retirement pension, there is insufficiency to maintain basic human needs, which often deprive them from leisure activities, quality food, clothing, medicines, and treatments, among others, and this has a negative effect on their quality of life. In fact, the value received for the elderly's retirement condition makes part of the family budget, and in some cases, it is the only remuneration, as evidenced by the National Household Sample Survey (PNAD), in which 42.1% of family income in the Northeastern Region came from pensions20.
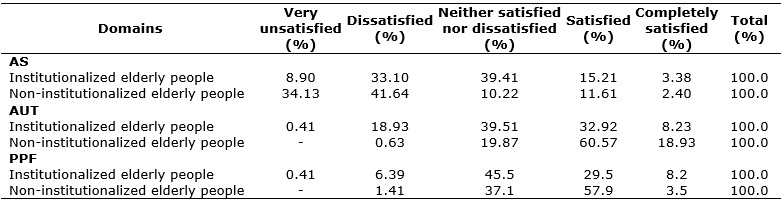
By applying the WHOQOL-Old questionnaire, the results of the QoL assessment according to the domains Sensory Abilities (SA), Autonomy (AUT) and Past, Present and Future Activity (PPF) can be observed in Table 1.
TABLE 1: Percentage distribution of answers associated with the domains SA, AUT
and PPF. Cuité - PB, 2013.
Legend: SA=Sensory Abilities; AUT=Autonomy; PPF= Past, Present and Future
Activities.
In the domain AS, the scores on the answers satisfied and completely satisfied corresponded to a greater impairment of the senses (hearing, sight, taste, smell, touch) and consequently affect negatively in daily life and in the way of interacting with people. Thus, the answers dissatisfied and very dissatisfied obtained the highest percentages by the non-institutionalized elderly, with 41.64% and 34.13%, respectively, while the institutionalized elderly accounted for 33.10% and 8.90% for the same questions.
The high percentage of scores in the answers that indicate greater sensory impairment by the institutionalized elderly may result from the more advanced age of some members of this group, as well as from the prevalence of diseases that affect the senses. These latter may be involved with the institutionalization or due to the aging process itself. The loss of the senses compromises the daily life, the capacity to participate in activities and the social interaction, making the elderly become dependent of care. The QoL of the elderly population includes the maintenance of autonomy and functional capacity. Thus, when an elderly person shows impairment of the senses, there will be a reduction in functional capacity, negatively influencing the quality of life21.
As for the domain AUT, the scores on the answers satisfied and fully satisfied mean the best degree of autonomy. Most of the scores obtained by the non-institutionalized elderly refer to the answersatisfied, corresponding to 60.57%, but only 0.63% answered unsatisfied. For the institutionalized elderly, the highest percentages obtained were in the answersneither satisfied nor dissatisfied with 39.51%, followed by satisfied, with 32.92%. In sum, institutionalized elderly reached higher scores in relation to the answers that represent the worst perceptions about the domain autonomy, revealing that they have greater limitations in carrying out daily activities such as feeding themselves, performing body hygiene and moving to the dormitories.
With advancing age, a gradual increase in the limitations of day-to-day activities occurs, which affects independence and autonomy. Functional independence relates to the ability to do something on one's own. Regular physical activity has been considered imperative for the maintenance of physical conditioning in elderly individuals, as well as to reduce and reverse the loss of muscle mass, contributing to the preservation of functional autonomy, healthy aging and the improvement of QoL22.
Concerning the domain related to perception and perspectives on past, present and future activities, in which the questions involve the degree of satisfaction with the recognition that the elderly have achieved through life and with what to expect from the future, the non-institutionalized elderly achieved a higher percentage of scores with the answer satisfied, corresponding to 57.9%. As for the institutionalized elderly, the maximum percentage was attributed to the answer neither satisfied nor unsatisfied, with 45.50%, and only 29.50% for the answer satisfied. As evidenced, most non-institutionalized elderly reported being satisfied with past, present and future activities. This can be related to the lower age range of the two categories investigated, together with the low degree of dependency, which is a favorable point for them to seek more recognition and assets over time.
For a person who has worked most of their life in order to achieve a better QoL in both social and economic terms, achieving what they intended in senile life is synonymous with full satisfaction and personal fulfillment. Elders who achieve this feat are considered winners, in face of their visions and ambitions throughout their lives. These achievements, associated with the feeling of continuing to reach their goals and objectives, contribute to the formation of a good QoL23.
Table 2 shows the results of the QOL assessment according to the domainsSocial Participation (SOP), Death and Dying (DD) and Intimacy (INT).
TABLE 2: Percentage distribution of answers associated with the domains SOP, DD
and INT. Cuité – PB, 2013.
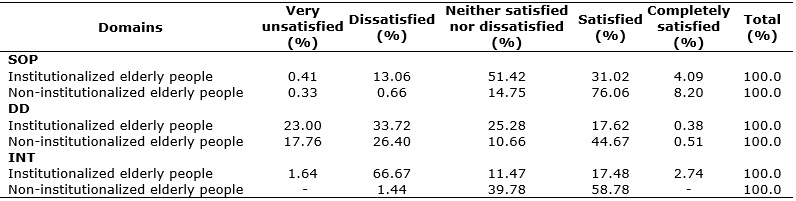
Legend: SOP= Social participation; DD=Death and Dying; INT=Intimacy.
Table 2 shows that the non-institutionalized elderly have higher social participation than the institutionalized ones, with 76.06% for the answer satisfied and 8.20% for completely satisfied, differing from the 31.02% and 4.09%, for the same answers given by the institutionalized elderly. This result may be related to the accomplishment of actions in the social environment by the non-institutionalized elderly because, in addition to living in the community with their relatives and friends, they have the opportunity to experience a schedule that allows the development of work activities, religious activities, volunteer work, physical exercises together in groups, participation in art workshops, poetry workshops and dance groups, among other activities.
In this sense, it is undeniable that social support becomes essential for the elderly to maintain their autonomy and have a satisfactory old age. In addition, elderly people who actively participate in collective activities and who have informal social support, mainly from the family, often have better physical and mental health24. In addition to the family, the multidisciplinary team of the family health strategy - a scenario in which the elderly have been increasingly present - must invest in the development of skills to deal with aging, either in individual or collective care, in the promotion or recovery of health25.
Regarding the results pertinent to the domain death and dying, the questionnaire had questions about the degree of concern of the elderly in the last two weeks with death, regarding the fear of dying, about not being able to control their death and the fear of feeling pain before dying. In this domain, the answers nothing (very dissatisfied) and very little (unsatisfied) are equivalent to the best levels of QoL. Although there was a variation in the answers in both groups because it was a very particular feeling, unlike the other domains, the institutionalized elderly had the best percentages of scores, with 33.72% for the item very little and 23.00% for the item nothing.
This variation may be related to the perception of many elders as to the inevitability of death, being these conformed and not wanting to think about it. Fear of death can interfere negatively with the elderly's QoL, as it generates anxiety and prevents the elderly from performing tasks that previously led to satisfaction. Scientific research shows that spirituality and religiosity provide relationships with the QoL of individuals, since many elderly people seek religion as a form of being comforted in the face of the feeling that they will die some day26.
Death is associated with suffering and its process is divided into five periods. The first is denial, when the individual refuses to accept that they have a fatal condition. They thus reveal anger, negotiation, depression, and the acceptance that death is inevitable. It is noted that the periods do not follow each other exclusively in an orderly way, and may pass through each other, particularly during the negotiation period, when the patient believes that they can change their condition when submitted to a particular treatment. The recognition that negotiation is not possible with death often leads to the fourth stage, which is depression. The last period is acceptance, when the individual recognizes their mortality and the nearness of the end27.
The domain intimacy involves items about partnership, the feeling of love and the ability of the elderly to be loved. When analyzing Table 2, there is a significant divergence of results. While a large proportion of the non-institutionalized elderly showed to be satisfied with intimacy (58.78%), institutionalized patients were the majority in stating that they were dissatisfied (66.67%). For these two equivalent scores ( satisfied and dissatisfied) the results were inversely proportional in both groups. The highest score regarding the best degree of intimacy on the part of the non-institutionalized elderly can be related to the fact that 65% of the participants in this group are married, favoring bonds of affectivity28, while among the institutionalized group, most of the elderly are single, married or widowed, which considerably diminishes the sense of partnership of these people.
Elderly people with good relations of intimacy, feelings of partnership, as well as expressions of love and sexuality, have optimized health in its various aspects, mainly in physical and psychological aspects, which ends up reflecting in a better QoL.
CONCLUSION
Recognizing QoL as a subjective and particular theme, which encompasses intrinsic factors such as health conditions and decisions about how life events are faced; and extrinsic factors, such as financial and environmental resources that surround individuals, the present study showed that those non-institutionalized had a better QoL, compared to the institutionalized ones.
The results of this study specifically propose the need to develop actions aimed at the reintegration of the institutionalized elderly into society. In addition, it raises the effective implementation of public policies aimed at this public, in order to promote better levels of QoL.
According to the questionnaire, elderly people living with their families fear death more than those institutionalized, which is one of the important findings. This reinforces the importance of the family for the elderly and confirms that the premature separation from the family anticipates their psychological death, lacking the accomplishment of other investigations that will ratify this phenomenon, once the sample size of this study is recognized as an important limitation.
REFERENCES
1.Câmara dos Deputados (Br). Lei no 10.741, de 1º de outubro de 2003. Dispõe sobre o Estatuto do Idoso e dá outras providências. Brasília (DF): Centro de Documentação e Informação; 2003.
2.Instituto Brasileiro de Geografia e Estatística. A Dinâmica Demográfica Brasileira e os Impactos nas Políticas Públicas [Internet]. 2009 [cited 2016 Mar 18].
3.Almeida AK, Maia EMC. Amizade, idoso e qualidade de vida: revisão bibliográfica. Psicol estud. (Maringá) 2010 [cited 2016 Mar 5]; 15(4):743-50.
4.Araújo LF, Coelho CG, Mendonça ET, Vaz AVM, Batista RS, Cotta RMM. Evidências da contribuição dos programas de assistência ao idoso na promoção do envelhecimento saudável no Brasil. Rev Panam Salud Publica, 2011 [cited 2016 Mar 11]; 30(1):80-6.
5.Veras RP. A urgente e imperiosa modificação no cuidado à saúde da pessoa idosa. Rev Bras Geriatr Gerontol, 2015 [cited 2016 Mar 6]; 18(1):5-6.
6.Camarano AA, Kanso S. Envelhecimento da população brasileira: uma contribuição demográfica. In: Freitas EVF, Py L, (Organizadores). Tratado de Geriatria e Gerontologia. 3ª ed. Rio de Janeiro: Guanabara Koogan; 2011.
7.Neri AL, Yassuda MS. Velhice bem-sucedida: aspectos afetivos e cognitivos. Campinas: Papirus; 2004.
8.Souza LM, Lautert L, Hilleshein. Qualidade de Vida e Trabalho voluntário em Idosos. Rev esc enferm USP, São Paulo, 2011 [cited 2016 Mar 6]; 45(3):665-71.
9.Reis LA, Torres GV, Silva JPA, Sampaio LS, Reis LA. Perfil epidemiológico de idosos institucionalizados no Município de Jequié/BA. Rev Enferm Atual, 2008; 46:19-23.
10.The Whoqol Group. The World Health Organization Quality of Life Assessment (whoqol): position paper from the World Health Organization. Soc Sci Med. 1995; 41(10):1403-9.
11.Torres GV, Balduino LSC, Costa IKF, Mendes FRP, Vasconcelos QLDAQ. Comparação dos domínios da qualidade de vida de clientes com úlcera venosa. Rev enferm UERJ, Rio de Janeiro, 2014 [cited 2016 Mar 11]; 22(1):57-64.
12.Papaléo Netto M. O estudo da velhice: histórico, definição de campo e termos básicos. In: Freitas EVF, Py L (Org.). Tratado de Geriatria e Gerontologia. 3ª ed. Rio de Janeiro: Guanabara Koogan; 2011.
13.Organização Mundial de Saúde. Envelhecimento ativo: uma política de saúde. Brasília (DF): Organização Pan-Americana da Saúde; 2005.
14.Martins JJ, Schneider DG, Coelho FL, Nascimento ERP, Albuquerque GL, Erdman AL, Gama FO. Avaliação da qualidade de vida de idosos que recebem cuidados domiciliares. Acta Paul Enferm., 2009 [cited 2016 Mar 8]; 22(3):265-71.
15.Heinonen H, Aro AR, Aalto AM, Uutela A. Is the evaluation of the global quality of life determined by emotional status? Qual Life Res. 2004; 13(8):1347-56.
16.Ministério da Saúde (Br). Conselho Nacional de Saúde. Resolução n. 466 de 12 de dezembro de 2012. Diretrizes e Normas Regulamentadoras de Pesquisa Envolvendo Seres Humanos. Brasília; 2012.
17.Organização Mundial de Saúde. Whoqol-Old Manual. 2005 [cited 2016 Mar 22].
18.Spinelli RB, Zanardo VPS, Schneider RH. Avaliação nutricional pela miniavaliação nutricional de idosos independentes institucionalizados e não institucionalizados em uma cidade da região Norte do Rio Grande do Sul. RBCEH, Passo Fundo, 2010 [cited 2016 Mar 18]; 7(1):47-57.
19.Instituto Brasileiro de Geografia e Estatística. Censo demográfico 2010 [Internet]. 2010. [cited 2016 Mar 28].
20.Torres GV, Reis LA, Reis LA, Fernandes MH. Qualidade de vida e fatores associados em idosos dependentes em uma cidade do interior do Nordeste. J Bras Psiquiatr., Rio de Janeiro, 2009 [cited 2016 Mar 17]; 58(1):39-44.
21.Vitorino LM, Paskulin LMG, Vianna LAC. Qualidade de vida de idosos em instituição de longa permanência. Rev Latino-Am Enfermagem, 2012 [cited 2016 Mar 4]; 20(6): [09 telas].
22.Fiedler MM, Peres KG. Capacidade funcional e fatores associados em idosos do Sul do Brasil: um estudo de base populacional. Cad Saúde Pública, 2008 [cited 2016 Mar 10]; 24(2):409-15.
23.Pereira RJ, Cotta RMM, Franceschini SCC, Ribeiro RCL, Sampaio RF, Priore SE. et al. Contribuição dos domínios físico, social, psicológico e ambiental para a qualidade de vida global de idosos. Rev Psiquiatr.; 2006 [cited 2016 Mar 11]; 28(1):27-38.
24.Areosa SVC, Benitez LB, Wichmann FMA. Relações familiares e o convívio social entre idosos. Textos & Contextos, Porto Alegre, 2012 [cited 2016 Mar 11]; 11(1):184-92.
25.Oliveira MAS, Menezes TMO. A enfermeira no cuidado ao idoso na estratégia saúde da família: sentidos do vivido. Rev enferm UERJ, Rio de Janeiro, 2014 [citado em 12 mar 2016]; 22(4):513-8.
26.Panzini RG, Rocha ND, Bandeira D, Fleck MDA. Espiritualidade/Religiosidade e Qualidade de Vida. In: Fleck MP, Lima AFB, Polanczyk CA, Trentini CM, Bandeira D, Patrick DL. et al. A avaliação da qualidade de vida: guia para profissionais de saúde. Porto Alegre: Artmed; 2008, p. 178-96.
27.Kübler-Ross E. Sobre a morte e o morrer. 9th ed. São Paulo: WMF Martins Fontes; 2008.
28.Rodrigues LR, Silva ATM, Ferreira PCS, Dias FA, Tavares DMS. Qualidade de vida de idosos com indicativo de depressão: implicações para a enfermagem. Rev enferm UERJ, Rio de Janeiro, 2012 [cited 2016 Mar 15]; 20(esp.2):777-83.