Source: Yale-m Scale13
FIGURE 1: Modified Yale Preoperative Anxiety Scale - EAPY-m.
ORIGINAL RESEARCH
Pre-operative children's anxiety level: evaluation by the modified Yale Scale
Carlos Eduardo Peres SampaioI, Thayanne Gama de Marins II, Thainá Vieira Fonseca Lira de AraujoIII
I
Nurse. Ph.D. Professor Head of the Veiga de Almeida University, Professor
University of the State of Rio de Janeiro. Brazil. E-mail: carlosedusampa@ig.com.br
II
Nursing student of the University of Rio de Janeiro State. Brazil. E-mail: thaymarins@live.com
III
Nursing student of the University of Rio de Janeiro State. Brazil. E-mail: lirathaina@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2017.28069
ABSTRACT
Objective: to determine the degree of anxiety in hospitalized children by applying the Modified Yale Preoperative Anxiety Scale (YPAS-m). Method: in this quantitative study using descriptive statistical analysis, 42 children on a pediatric surgery ward of a university hospital in Rio de Janeiro were observed in the preoperative period, between June and August 2016. The research project was approved by the research ethics committee of Pedro Ernesto University Hospital (opinion No. 1.587.764). Results: 69.05% of the children presented without anxiety, and 30.95% were anxious; the categories of the Yale-m Scale that displayed most items were vocalization and use of relatives. Conclusion: a minority of children presented with a level of high anxiety, and the domains of the Yale-m Scale that reached highest scores were vocalization and use of relatives.
Keywords: Child; preoperative, nursing; anxiety.
INTRODUCTION
Hospitalization is associated with a circumstance that bothers and interferes with the individual´s daily life since it includes a series of factors such as the decline of the health condition and the distance from the family and social context. With this, it affects the children in greater proportions due to changes in the family routine that can affect their development, bringing consequences, such as anxiety¹.
When the child is submitted to preoperative hospitalization, both the children and the family is affected due to the oscillation of the family life and stay in the hospital environment. The experience of hospitalization can be shocking and exhaustive, which may be related to the inclusion of the child and the family in a different environment from the daily life, and there is often a lack of knowledge and doubts about preoperative treatment, surgery, and prediction of high².
Faced with this fragile moment for the child and for the relatives, it is necessary to perform the nursing team, based on the interventions and care provided to the child, with the accomplishment of the appropriate procedures, clarification and the orientation regarding the surgery, aiming to reduce stress levels, to mitigate the negative consequences of hospitalization and to contribute to the recovery process3.
The concept of a surgical procedure for the patient becomes variable since it arouses different emotions, ranging from relief to success in solving a problem to the fear that some serious event may occur, which can lead to death. When the patient is submitted to preoperative hospitalization, doubts and fear can arise from an invasive treatment4.
The stay and the delay for the accomplishment of a surgery in hospitalized patients can generate stress and anguish. These sensations are expressed by concerns, tension, fear and reactions that can be measured through state scales and anxiety, indicating to the health team the needs of the patient in a surgical situation to be met5.
Anxiety is a common event in children during the period before surgery, which can lead to difficulties in performing the operative procedure, and when associated with hypertension, it can lead to surgical suspension. The American Academy of Pediatrics recommends 95 as a percentile of the normal physiological limit of blood pressure in children, which is given from their chronological age. Several proposals have been used to evaluate the level of anxiety of the pediatric patient, such as the modified Yale Preoperative Anxiety Scale (mYPAS) - an instrument that allows the evaluation of the level of anxiety, based on the observation of the child´s attitudes6.
This study aimed to determine the degree of anxiety of hospitalized children according to the application of the Modified Yale Preoperative Anxiety Scale (EAPY-m).
LITERATURE REVIEW
The preoperative period is subdivided into mediate and immediate. The immediate period corresponds to the 24 hours before the surgical act, extending until its passage to the surgical center. Among the actions and main competencies of nurses, in the immediate preoperative period, the most important is to check the preoperative preparation of the patient, verify the doubts and needs of the patient or family member about the surgery and reduce the patient's anxiety7. The main types of care are aimed at helping parents to adapt to the child's condition, promoting the bond between them, preparing them for the surgical procedure and guiding them to care about hospital discharge8.
Among the most pertinent procedures for the appearance of anxiety, there is the anesthetic induction, an increase in intraoperative consumption of anesthetics, which is characterized as the period that begins with the anesthetic-surgical procedure7, sleep disorders, reinstallation of enuresis, eating disorders, apathy, irritability and continued anxiety, indiscipline and little collaboration with health professionals9 .
Fears cause children to respond adversely to surgical events, due to the effects of preoperative preparation, which also contribute to behavioral problems after hospitalization. Most of them show the first surgical intervention as a strange event, so the stress before the surgical act can increase; but because they are elective surgeries, that is, scheduled, there would be a period of time for the pre-surgical preparation 10.
The immediate preoperative period can be overwhelming for the children and their family, due to the type of surgical procedure and the hospital scenario. The child´s exacerbated discomfort is due to the lack of knowledge and understanding about the surgery, fear of physical damage, being in an unknown environment and its susceptibility11.
Some factors may determine the child's level of anxiety in the preoperative period: their temperament, low levels of sociability, adaptive behavioral difficulties, impulsivity, previous surgical experience, hospitalization, troubled visits to pediatric offices, and elevated anxiety levels. YPAS-m was developed with the purpose of investigating the anxiety levels of children in the immediate pre-anesthetic period and at the time of anesthetic induction9; the measurement of the level of anxiety occurs from the observation of the child´s behavior12-14.
METHODOLOGY
It is a study with a quantitative approach since the data obtained are evaluated through the application of the Modified Yale Scale in children in the preoperative period.
The quantitative research is conceptualized in empirical evidence, based on objective reality and logical thinking, on statistical procedures and on the measurable attributes of human experience15.
The results generated by scientific research contribute to the formation of knowledge, strengthening the nursing profession and enabling the improvement of practice, which is based on theory16. The chosen theme requires greater scientific production to improve the quality of care in pediatrics.
The research project was approved by the Research Ethics Committee of the Pedro Ernesto University Hospital of the State University of Rio de Janeiro, under opinion 1,587,764. The principles of bioethics, such as autonomy, non-maleficence, beneficence, justice, and equity were respected, incorporating the individual and the community, as well as the norms established by Resolution 466 of December 12, 2012.
Being a research involving human beings, the participants were guided by it. Also, the objectives of the study were clarified, ensuring their anonymity, and the subject could interrupt their participation in data collection at any time, without any harm to themselves. The caregivers signed the Informed Consent Term (TCLE). Inclusion criteria were children classified as ASA (American Association of Anesthesiology) and ASA II (American Anesthesiology Association) and exclusion criteria were children 12 years old and over, sleeping, sedated and temporarily unaccompanied).
Fifty-two children participated in this study, but 42 children have included in the inclusion and exclusion method since 10 of them were sleeping at the time of the evaluation. Among those included, the ages range from 2 to 12 years old incomplete, of both genders and all to be submitted to surgical procedures.
The data collection instrument was applied to children, through direct observation, in the pediatric surgery ward of a university hospital, in the city of Rio de Janeiro, from June to August 2016, in the presence of parents or caregivers at that time.
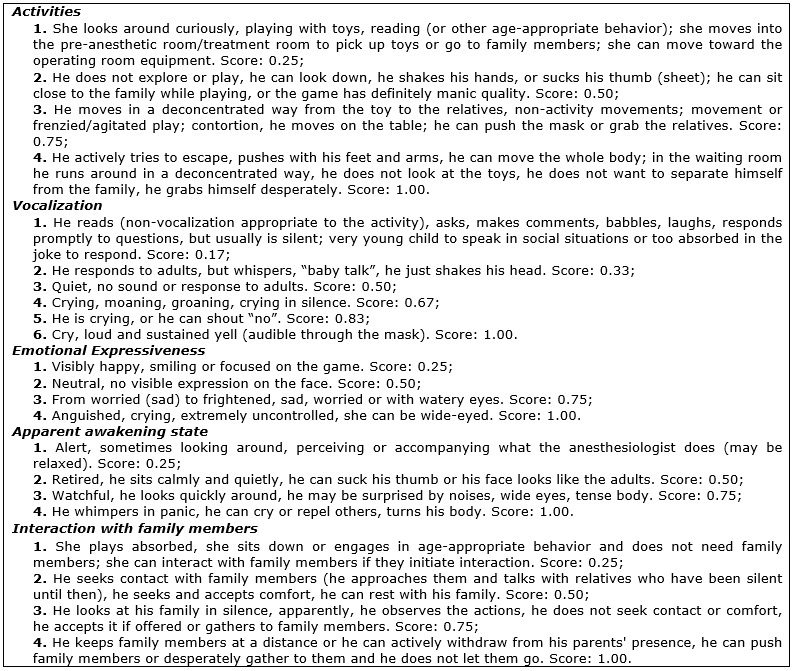
The parameters for the analysis of anxiety were given by the total EAPY-m score. The scale has items distributed in five domains of behavior that contemplate the reaction of the child in the environment where it is, being domain 1- activities (with four categories); 2- vocalization (with gender categories); 3 - emotional expressiveness (with four categories); 4- apparent awakening state (with four categories) and 5- interaction with family members (with four categories). For each domain, a partial score is given based on the observed score divided by the number of categories. The score of each domain is added to the others and then multiplied by 20. The cutoff scores for assessing the patients are no anxiety - 23.4 to 30 and with anxiety - greater than 3017. The EAPY-m is presented in Figure 1.
Source: Yale-m Scale13
FIGURE 1:
Modified Yale Preoperative Anxiety Scale - EAPY-m.
The data were submitted to the descriptive statistics analysis, calculating the absolute frequencies, percentages, and measures of central tendency (mean and median).
RESULTS AND DISCUSSION
The absolute and percentage frequencies obtained by the children, in each domain of the Yale-m Scale, reflect the measurement of the level of anxiety manifested in their attitudes. The domains that presented the most categories involved were vocalization, 30 (71.4%) children had a category 1 score; 7 (16.7%) of category 2; 4 (9.5%) of category 3; 1 (2.4%) of category 4; while none of the children presented behavior compatible with categories 5 and 6, while the apparent wake state domain was reached by most 35 (83.3%) children in category 1, as shown in Table 1.
TABLE 1:
Distribution of children by category of each domain of the Yale-m Scale.
University hospital, Rio de Janeiro, 2016. (N=42)

According to the results, it is important to emphasize that the first categories of each domain presented higher frequencies, which contributes to a low score at the end of the evaluation, leading to classification without anxiety. This is the most frequent classification of the analyzed children, which can be verified through Table 1. The findings show the incidence of lower anxiety levels. The domains that reached the most categories were: vocalization and interaction with family members, showing an important factor - the relationship with the family contributes to the maintenance of children´s emotional balance, especially in moments of high stress, such as in the preoperative period, according to Table 1. The interaction domain with family members shows to be the one that reached higher levels of categories, indicating the need for other investigations in the search for the minimization of stressors for children, during the preoperative period of pediatric surgeries.
Regarding the anxiety scores obtained according to the Yale-m Scale, the study showed that 13 (30.95%) children expressed anxiety with mean scores 42, while 29 (69.05%) children without anxiety had the mean scores 23.7, as shown in Table 2. These data further complement the importance that nursing orientations exert in the emotional state of the children and their companions in the preoperative period, so the perioperative period is the possibility for the children and their family. Thus, it is necessary to intensify the guidelines by the nurses, directed to pre-operative nursing care, such as: not washing the hair on the day of surgery, removing dental prostheses, contact lenses, jewelry and nail polish, fasting from midnight before surgery, among others18. Guiding the child about nursing care, according to their understanding, the nurse is able to reduce their anxiety. When also guiding the caregiver, the nurse can leave the child-caregiver pair more relaxed, since the child's frame will be confident to offer comfort and emotional support19-22.
TABLE 2:
Children's preoperative anxiety scores, according to the Yale-m Scale.
Universitary hospital, Rio de Janeiro, 2016. (N=42)

During the guidance, care to how much the family understands the information they are given is needed. The nurse should use words accessible to each family, according to the individual´s reality, when guiding them about the anesthetic-surgical procedure23. The dialogue will be effective if the caregiver understands the orientation of the professional. To ensure understanding, nurses must consider the social and cultural factors of assisted families and interact with them24, making them aware of what will be done in the surgical center, contributing to the reduction of anxiety levels25 of the child and the family, which also influences his recovery in the postoperative period20.
The data presented in this research, that nurses´ orientation is fundamental for informing, calming and comforting the responsible ones of the children, are proven by other similar and recent studies 26,27. These results highlight the importance of nursing care throughout the perioperative period, both for the children and their caregivers since the guidelines allow mental well-being to the adults and reduce their and the infant's anxieties.
There were 13 children who participated in this study (30.95%) with anxiety symptoms, ranging from dry mouth, sweating, palpitations, tachycardia, hyperventilation to feelings of apprehension, nervousness, restlessness, and sleep-wake cycle alterations28,29. However, 29 (69.05%) had no posture compatible with the anxiety disorder.
These results confirm that most of the children were presented without anxiety, showing that the nursing orientations and activities performed should be maintained. The nursing care provided is able to balance technical and scientific knowledge, ethical values and humanization to provide adequate care. It allows the next step to be an appropriate approach to stimulate physical and psychological care8 for the child and the caregiver.
However, this nursing guidance has not yet reached their maximum efficacy, since there was an incidence of 13 (30.95%) children with anxiety, in the preoperative period. Anxiety is a natural response to the stresses experienced by individuals in situations of risk,30 which makes the presence of this feeling routine in pediatric wards in the preoperative period, since both the procedure and the environment of the operating room are foreign to the child and the caregiver31. Fear of the unknown is the fuel for anxiety and mainly affects the caregivers, who fear that their children will experience complications during surgery and feel postoperative pain32.
If the caregiver is tense, the child becomes more anxious because he is realizing that the adult who provides him with protection, security, and emotional support is unable to trust him22. However, it is interesting to note that nursing orientations can have an impact on the stabilization of anxiety in the child, since, as previously mentioned, 29 (69.05%) children were not anxious and this is more than twice as anxious children, 13 (30.95%).
CONCLUSION
Anxiety in the immediate preoperative period is associated with hospitalization in an unknown environment, with practices different from the daily routine of children, which may contribute to changes in blood pressure beyond the limited percentiles considered. In this way, the surgical procedure could be affected, and even be suspended. In order to avoid this, it is necessary to emphasize the orientation of the children and their caregivers, the specificities of the surgery and the period of hospitalization. Clarifying pertinent doubts assists in better conviviality between the child and the nursing team, reducing the anxiety of waiting for surgery or possible surgical suspensions.
The nurse should be able to accommodate the child and his caregiver in the immediate preoperative period and provide assistance according to the needs of each family. Guidelines should be adapted to the degree of understanding of their recipient, avoiding complicated words and terms if they are not recognized by the child and/or the caregiver, as keeping the child without anxiety is as important as keeping the caregiver quiet.
The Yale-m scale is an assessment tool, based on the rapid observation of child behavior and easy application, which allows measuring the level of anxiety in children, being of high sensitivity and specificity. In this study, the high level of anxiety was presented in most of the studied children and the domains of the Yale-m Scale with more categories were vocalization and interaction with relatives. However, it is imperative to intensify and maintain the nursing guidelines to continue guaranteeing low levels of anxiety of these patients.
REFERENCES
1.Gomes GLL, Fernandes MGM, Nóbrega MML. Anxiety of children hospitalization: conceptual analysis. Rev Bras Enferm. 2016; 69(5):884-9.
2.Gomes GLL, Nóbrega MML. Anxiety of children hospitalization: proposal of a nursing diagnosis. Rev Latino-Am Enfermagem. 2015; 23(5):963-70.
3.Lima de Souza GL, Silva KL, Medeiros ACT, Nóbrega MML. Nursing diagnoses and interventions using ICNP® in hospitalized children. Rev enferm UFPE. 2013; 7(1):111-8.
4.Silva JP, Garanhani ML. The meaning of perioperative care for the surgical child. Rev eletr enferm. 2011;13(2):259-68.
5.Costa TMN, Sampaio CEP. Nursing guidance and its influence on anxiety levels of hospital surgical patients. Rev enferm UERJ. 2015; 23(2):260-5.
6.Barreira AK, Couto GBL, Vasconcelos MMVB, Vianna RBC. High blood pressure in childhood. J Bras Odontopediatr Odontol. 2003; 6(30):131-6.
7. Brazilian Society of Nurses of Surgical Center, Anesthetic Recovery and Material and Sterilization Center. Recommended Practices 6th ed.São Paulo: SOBECC; 2013. p. 176-289.
8.Hockenberry MJ, Wong DW. Fundamentals of pediatric nursing. 9 th ed. Rio de Janeiro: Elsevier; 2014.
9.Guaratini AA, Marcolino JAM, Teixeira AB, Bernardis RC, Passarelli MLB, Mathias, LAST. A cross-sectional study of preoperative anxiety in children: use of the modified Yale scale. Rev Bras Anestesiol. 2006; 56(6):591-601.
10.Broering CV, Crepaldi MA. Preparação e o estresse de crianças submetidas a cirurgia. Psicol estud. 2011; 16(1):15-23.
11.Garanhani ML, Valle ERM. The meaning of surgical experience for the child. Science, Care and Health. 2012; 11(supl):259-66.
12.Kain ZN, Mayes LC, Cicchetti DV, Domenic V, Bagnall AL, Finley JD, Hofstadter MB. The Yale Preoperative Anxiety Scale: as compared to a "gold standard"? Anesth Analg. 1997; 85: 783-8.
13.Mello GE, Gonçalves BV, Novo FN, Moro TE. Relationship between preoperative anxiety at preschool age and the anxiety of their respective caregivers: a cross-sectional study using the modified Yale Scale. Rev Fac Ciênc Méd Sorocaba. 2015; 17 (3):131-4.
14.Lima RL, Macedo AF, Duarte DA, Sannt'Anna GR. Evaluation of predictive anxiety parameters in children aged three to five years old, using videos as a facilitator in pediatric dentistry. Rev Bras Pesq Saúde, Vitória. 2013; 15(1):25-32.
15.Polit DF, Beck CT, Hungler BP. Fundamentals of nursing research: methods, evaluation and use. 5th ed. Porto Alegre (RS): Artmed Editora; 2004. p. 29-172.
16.Ponte KMA, Borges MCLA, Barreto FA, Moreira TMM, Silva LF, Fialho AVM. Scientific production in surgical nursing: analysis of the quantitative studies performed between 2005 and 2009. Rev RENE. 2012; 13(1):231-41.
17.Cumino DO, Cagno G, Gonçalves VFZ, Wajman DS, Mathias LAST. Impact of the type of pre-anesthetic information on parental and child anxiety. Rev Bras Anestesiol. 2013; 63(6):473-82.
18.Sena ACD, Nascimento ERPD, Maia ARCR. Nursing practice in patient care in the immediate preoperative period of elective surgery. Rev Gaúcha de Enferm. 2013; 34(3):132-7.
19.Howe J, Scipien GM. The hospitalization of a child. In:Scipien GM, Chard MA, Howe J, Barnard MU, editors. Pediatric nursing care. St. Louis (USA): Mosby; 1990.
20.Whaley LF, Wong DL. Nursing care of infants and children. 4th ed. St Louis (USA): Mosby; 1991.
21.Eyres P. The role of the nurse in the family-centered care. Nurs Clin North Amer. 1972; 7(1):27-39.
22.Sampaio CEP, Ventura DSO, Batista IF, Antunes TCS. Feelings of the caregivers of children submitted to surgical procedures: experiences in the perioperative period. Rev Min Enferm. 2009; 13(4):558-64.
23.Castellanos BEP, Jouclas UMG. Perioperative nursing care: a conceptual model. Rev esc enferm USP. 1990;24(3):359-70.
24.Santos, RM, Cassapula, RL, Hellberguer, TMS. Preoperative orientation program in pediatric surgery - experience report. Cogitare enferm. 2000; 5(1):61-5.
25.Barreto RASS, Araújo ACO, Suzuki K, Freitas VC. The need for client information in preoperative cholecystectomy. Rev Min Enferm. 2010; 14(3):369-75.
26.Frias TFP, Costa CMA, Sampaio CEP. The Impact of the preoperative nursing visit on the level of anxiety in surgical patients. Rev Min Enferm. 2010; 14(3):345-54.
27.Sampaio CEP, Silva RV, Comino LBS, Romano RAT. Anxiety level of children's attendants in outpatient surgery: contributions of the nursing consultation. Rev enferm UERJ. 2014; 22 (2):233-8.
28.Flório MCS, Galvão CM. Outpatient surgery: identification of nursing diagnoses in the perioperative period. Rev Latino-Am Enfermagem. 2003; 11(5):630-7.
29.Garbossa A, Maldaner E, Mortari DM, Biasi J, Leguisamo CP. Effects of physiotherapeutic guidelines on the anxiety of patients undergoing myocardial revascularization surgery. Rev Bras Cir Cardiovasc. 2009; 24(3): 359-66.
30.Potter PA, Perry AG. Great treatise on nursing practice - clinic and hospital practice. São Paulo: Livraria Santo Editora; 2005.
31.Melo WA, Marcon SS, Uchimura TT. Hospitalization of children from the perspective of their caregivers. Rev enferm UERJ. 2010; 18(4):565-71.
32.Sampaio CEP, Ribeiro DA, Marta CB, Seabra Junior HC, Francisco MTR. Determining factors of anxiety and coping mechanisms in general surgical procedures. R Pesq: cuidado fundam online. 2013; 5(4):547-55.