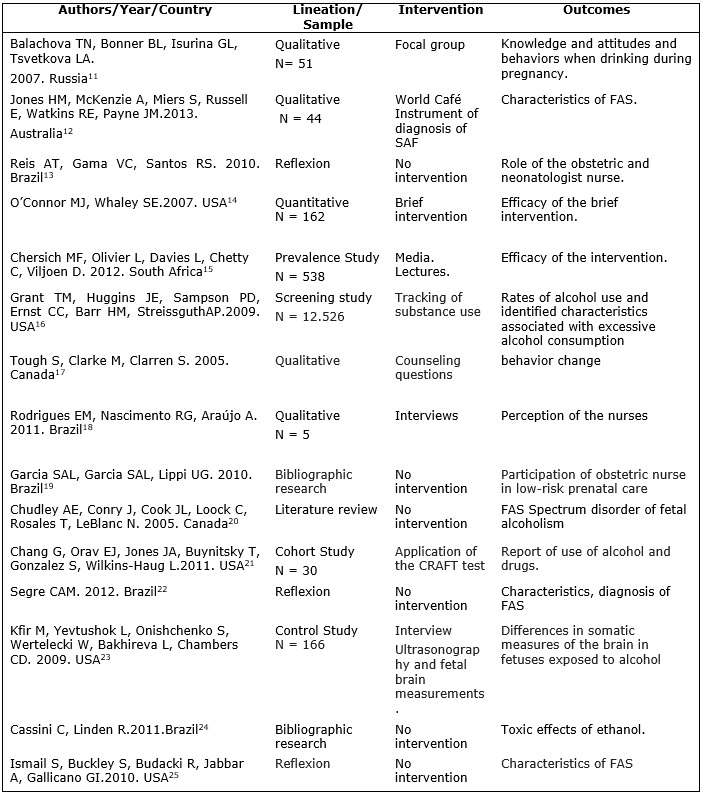
FIGURE 1: Studies included in the integrative review, according to title, country of origin, year of publication, lineation, interventions and outcomes. Rio de Janeiro, Brazil, from 2005 to 2013.
Source: The authors
REVIEW ARTICLE
Prevention of fetal alcohol syndrome: input to obstetrical nurses' practice
Rosângela da Silva SantosI; Marselle Pimenta Estefanio II; Raissa Muniz FigueiredoIII
I
Nurse. PhD. Assistant Professor. Universidade do Estado do Rio
de Janeiro, Rio de Janeiro, Brazil. E-mail: rosangelaufrj@gmail.com
II
Nurse. Specialist in Neonatology. Fundação Oswaldo Cruz.
Rio de Janeiro, Brazil. E-mail: marsellepe@hotmail.com
III
Nurse. Viva Rio Company. Paulino Werneck Municipal Health Center. E-mail: raissa.muniz26@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2017.27793
ABSTRACT
Objective: to discuss the prevention of Fetal Alcohol Syndrome by health personnel. Method: integrative literature review, using articles indexed in Portuguese and English, published from 2005 to 2013. Data collection, in February 2014 in the Virtual Health Library in three databases, identified 653 articles, of which 638 were excluded and 15 selected. Content analysis was used. Results: information on attitudes to, and knowledge and use of, alcohol in pregnancy, information to women and pregnant women, the effectiveness of brief intervention, information conveyed by radio, television or nurses, and knowledge transmission by health personnel making risks known to young women before they become pregnant. Conclusion: the difficulty of diagnosing Fetal Alcohol Syndrome reveals the need to broaden the discussion of preventive policymaking. Health personnel work to prevent the syndrome and should intensify that endeavor at various levels: primary, secondary, educational and parental.
Keywords: Obstetric nursing; primary prevention; ethanol; pregnant.
INTRODUCTION
Among the possible sequels caused by alcohol consumption during pregnancy are Fetal Alcohol Syndrome (FAS) and its incomplete forms; alcohol-related congenital defects (ARCD) and alcohol-related neurodevelopmental disorders (ARND). FAS is the most serious picture represented by fetal alcohol spectrum disorders (FASD). Its clinical manifestations are determined by a complex group of signs and symptoms that vary according to the amount of alcohol ingested and the period of gestation, in addition to other factors1.
FAS is a group of manifestations that occurred during pregnancy, resulting from the adverse effects of ethanol consumption, which causes restriction of intrauterine and postnatal ponderosoestatural growth, central nervous system dysfunctions, microcephaly and characteristic facial changes1. It affects around 33% of children born from mothers who have used more than 150g of ethanol per day and it is present in 1 out of 1,000 newborns2,3.
The effects of maternal exposure to alcohol affect approximately 1 to 3% of live births in the United States3. In Brazil, there are still no data on the incidence in neonates, since the diagnosis of the syndrome is difficult. Because alcoholism is a disease of denial, there is a strong possibility that its users will omit or deny their daily use, especially, pregnant women.
In prenatal consultations, pregnant women are questioned by nurses and/or obstetricians regarding this issue. The professional is limited to inquire whether the woman consumes alcoholic beverage. If it is positive, one drinks socially, which induces the woman to respond tacitly. The ingested dose and frequency are not correctly obtained and the abusive use of alcoholic beverages is not diagnosed.
Prenatal care should be provided by a multiprofessional health team, which needs to use clinical knowledge related to their professional competence to provide quality care to the mother/child binomial. To this end, it is necessary to include actions to promote health and prevent damages caused by the use of alcohol during pregnancy4,5.
The obstetrician nurse can perform an empathetic intervention and provide confidence to the pregnant woman in order to assist her in decision making, with a view to reducing or even stopping the abusive use of alcohol6.
It has been delimited as a guiding question: How do health professionals promote FAS prevention?
This integrative literature review is justified due to the lack of knowledge of the fetal alcohol syndrome by some health professionals4, difficulty in establishing early diagnosis and high incidence3. The health professional, when assisting the woman during the prenatal care, and not performing an effective approach, misses the opportunity to guarantee: outpatient follow-up from the beginning of pregnancy; maternal and neonatal quality of life; the reduction of the incidence of intercurrences and pathological conditions to the newborn4.
The relevance lies in the serious sequelae caused in the fetus and newborn, which have no cure and remain, throughout life, impairing the individual's handicap.
This study aimed at discussing the prevention of FAS by health professionals, based on the literature reviewed.
METHODOLOGY
The integrative review of the literature consists of synthesizing different data on a specific theme, to deepen the knowledge in a systematic and orderly way7. The bibliographic survey was carried out by means of consultation in the Virtual Health Library, indexed in the databases: Medical Literature Analysis and Retrieval System Online (MEDLINE), Latin American and Caribbean Literature in Health Sciences (LILACS) and Database in Nursing (BDENF).
The six phases of the integrative literature review process have been elaborated: guiding questions, search or sampling in the literature, data collection, critical analysis of the included studies, discussion of the results and presentation of the integrative review8.
The research on the base took place in February of 2014. The inclusion criteria were: articles available in Portuguese and in English, published between the years 2004 and 2013. Temporal cutback justified by the launch, in 2004, of the National Policy of Integral Attention to Women's Health 9.
The following keywords have been used: prenatal; nurse obstetrician; doctor; alcoholism and fetal alcohol syndrome . Abstracts, duplicate articles, those that were not accessed by the Internet and those that were not related to the topic have been excluded.
The data has been collected by instrument made by the authors, addressing: title; year/country; lineation/sample; interventions; outcome.
The data analysis considered the characteristics of each study, its similar or different results and methodological rigor8. The distribution and specialty were presented according to statistics in absolute frequency and percentage. The content analysis of Bardin has been used, it is a thematic-categorical modality, which systematizes content based on inference, while the analysis technique searches for elements that can give unity to a certain type of message or theme10.
RESULTS
A total of 653 articles were identified and 638 were excluded for the following reasons: repetition in the databases (49), not meeting the objective of the integrative review (553) and not having access to the entire article (36). Thus, 15 articles11-25 constituted the study sample, 10 studies in the MEDLINE database, four in LILACS and one in BDENF.
No publications were found on the subject in 2004, 2006 and 2008. The largest number of studies was published in 2010 and 2011 ‒ three publications in each year (20%) ‒, two articles in the years 2005, 2007, 2009 and 2012 (13%), and only one in the year 2013 (7%). Of these, nine articles were medical publications (60%), three nursing (20%), two from other areas of health (pharmacy and psychology) (13%), and one did not identify the authors' education. Two articles resulted from quantitative research; three from experimental studies; five of qualitative researches, two of bibliographical researches and only three reflection articles.
The result contributed to the reconfiguration of obstetric nurse practice, offering subsidies for adequate prenatal care, with a view to the prevention of FAS and early identification of pregnant women who consume alcoholic beverages, according to Figure 1.
FIGURE 1: Studies included in the integrative review, according to title, country
of origin, year of publication, lineation, interventions and outcomes. Rio
de Janeiro, Brazil, from 2005 to 2013.
Source: The authors
DISCUSSION
The studies were grouped into two categories: Prevention of alcohol consumption during pregnancy and Detection of alcohol consumption and diagnosis of FAS. The first category consisted of seven articles11-17, totaling 47% of the studies; the second, by 8 18-25, totaling 53%.
Prevention of alcohol consumption during pregnancy
It discusses the knowledge and practices of pregnant women and health professionals about the use of alcohol during pregnancy and strategies for their prevention11-17.
The first article of this category discussed a strategy adopted as FAS prevention and used focus groups to obtain information from pregnant Russian women and their partners, non-pregnant women and physicians about their attitudes, beliefs and knowledge about alcohol use during pregnancy 11.
The importance of the dissemination of information to women and pregnant women was emphasized. The women reported that during childhood they received misinformation about the harm of alcohol by their family and friends. This fact contributed to the ignorance of the harmful effects of alcohol, since the information was not adequately provided by doctors and women's clinics. The doctors justified lack of time, information and resources. Most women and pregnant women were unaware of the harmful effects or discredited a possible association of alcohol use with birth defects and mental retardation11.
The doctors had limited knowledge about FAS or the effects of alcohol use during pregnancy. Some were unaware of the manifestations of the syndrome or were not aware of the specific risks of consumption during pregnancy11.
The participants reported ambivalence about maternal alcohol consumption, with responses ranging from abstinence, the acceptability of drinking small amounts, and the consumption of red wine, considered to be beneficial for health12. Few participants identified FAS-related problems as a consequence of consumption.
As for the dissemination of information, participants in a survey believed that it should be socialized, including with men, through national campaigns, using communication vehicles, television, radio, social networks, posters, among others, as well as the implementation of warning labels on bottles of alcoholic beverages12.
It is recommended the approach of the community by the FAS researchers through meetings and specific questionnaires, in order to observe the perception of the community and to discover how to improve the assistance. Based on this information, messages from health professionals should be consistent and accurate regarding alcohol withdrawal and the need to seek care, even though FAS is incurable, since early diagnosis provides strategies for children and their families for improvement of the quality of life12.
When approaching the consumption of alcoholic beverages during the consultation, one should ask about diet and lifestyle. These need to be clear, easy to understand and not resemble an interrogation. They should be held in a reserved place and in the absence of partners or family members. The professional should be free from judgments and prepared to deal with guilt, defense, fear, shame and panic. For this, it is necessary to build trust between the health professional and the woman12.
A cartesian attitude of health professionals to detect gestational problems and act on them can disregard the social context, since the relationships and environments that lead to alcohol consumption are not always contemplated. The role of the nurse before the FAS is to establish a relationship of help to the alcoholic pregnant woman. It is necessary to establish bonds, to aid in the difficulties and treatment, since the bonds between the mother and her child will be shaken. The professional must be prepared and adopt therapeutic positions such as: empathy, unconditional acceptance or respect, coherence, confrontation, immediacy and concreticity 13.
Among the prevention strategies for alcohol consumption during pregnancy, an article discussed the effectiveness of using a brief intervention as a technique to help pregnant women to maintain alcohol withdrawal. The intervention uses a 10 to 15-minute approach to counseling by people not specialized in the treatment of alcohol abuse and addiction. The proposal includes awareness of the negative consequences of consumption, counseling focused on identifying situations and actions aimed at reducing the risk of alcoholic beverages and assisting with setting targets for alcohol reduction14.
In South Africa, the high incidence of FAS stimulated the development of strategies to modify the social determinants of alcohol intake in pregnancy. The strategies used involved: actions of community health agents trained to address the harm of alcohol consumption during pregnancy; distribution of posters and pamphlets in the prenatal consultations, shops, bars, government departments and prisons; publication of articles focusing on newspaper prevention; regular radio announcements on the subject; and local theatrical productions on FAS. These interventions were effective in reducing alcohol consumption and ineffective in the incidence of FAS, although the information was transmitted by radio, television or by nurses 15.
The transmission of knowledge to pregnant women by health professionals was also discussed in another article as a prevention strategy, considering the lack of knowledge of pregnancy, period of organogenesis, and quantity and exposure to alcohol16. Likewise, this article highlights the importance of disseminating knowledge to the community in a simple and direct way. One of the issues raised is to reflect on how family doctors can better prevent alcohol exposure during pregnancy. The most effective way is to expose the risks of alcohol consumption during pregnancy. The risk disclosure should preferably take place before the woman becomes pregnant, so that there is a drastic reduction in the damage17.
Detection of alcohol consumption and diagnosis of FAS
This category analyzed the issue of alcohol consumption and FAS diagnosis during the prenatal care18-25.
The nurses' perception of their role in the prenatal care and the validity of the use of protocols in the actions of health professionals in the Family Health Strategy (FHS) were investigated. The historiographical survey of the prenatal care evidenced advances such as the Humanization of Childbirth and Birth Program and the Information System of the Prenatal and Birth Humanization Program. The difficulties for prenatal care without discussing the risks of alcohol intake during pregnancy by professionals were discussed. The activities of the professional have been emphasized, with the identification and correction of maternal or fetal abnormalities, but without relation to the FAS18.
A study that advocated the participation of obstetrician nurses at the primary level of attention to women's health, also, did not focus on the early identification of the syndrome. The discussion of conflicts between the different health professionals was prioritized, considering the need for a broad reorganization in these areas, with an increase in the number of obstetrician nurses in primary care to clarify the health activities of women and neonates19.
Another article, considered one of the first guides in Canada on the diagnosis of diseases associated with alcohol consumption and pregnancy, emphasized the importance of multiprofessional groups in the diagnosis of FAS, with the use of questionnaires, survey of maternal alcohol consumption and search for neurological signs. It was emphasized that screening tests should be validated and they could not be dissociated from the culture conception, economic and educational situation of individuals20.
Other strategies considered effective were: structured clinical interview according to the criteria of the Manual of Statistical Diagnosis of Mental Disorders; followed by estimates of daily alcohol consumption in an earlier period of six months to the date of the interview; the evaluation of the alcohol intake pattern in three contexts: in celebrations, at home and in dealing with negative emotions; T-ACE questionnaire, based on alcohol screening during gestation and evaluation of the ability to modify related behaviors, such as drinking, smoking, diet, exercise, among others, as well as the review of records for the verification of findings on the alcohol use21.
Another article discussed the motivations that led the pregnant woman to drink. It highlighted depression, affective deficiency, unwanted pregnancy, misinformation about drug effects and compromised nutritional status. The risk factors for alcohol use or abuse were: adolescence, low level of schooling, low socioeconomic level, cohabitation with alcoholics, smoking, illicit drug use, unplanned pregnancy and absence of prenatal care22.
For accurate diagnosis and control over the clinical effects of the syndrome, we use ultrasound signals or markers to measure the exposure to alcohol and specific biomarkers. The ultrasonography can detect FAS, but it still needs to be improved23. Biomarkers, on the other hand, have a higher degree of sensitivity, revealing the intensity of alcohol exposure through meconium or the child's hair24.
The questionnaire was considered the best means of mapping FAS, but it has, as a limitation, the dependence on patients' honest answers, since some have difficulty admitting alcohol use and some doctors are reluctant to approach this subject during the consultations25.
Markers such as blood and urine, too, are used to detect alcohol consumption by the expectant mother. They limit themselves to measuring only the alcohol intake, and it is not possible to diagnose FAS. This syndrome causes changes in genes related to cell division, apoptosis, and neural connections, and it is incumbent on future studies to find more efficient markers that act to verify such changes25.
Among the FAS prevention strategies, it is possible to infer that the T-ACE questionnaire is one of the most effective for tracking the conditions of the pregnant woman, although it is very difficult to obtain totally reliable information26. The use of the brief intervention can make the pregnant woman motivated to deal with her alcohol-related problems and prevent the potential complications of alcohol consumption for the woman and her baby26. When approaching the pregnant woman without judgments, the nurse can make her rethink how the consumption of alcoholic beverages may be interfering with her life and help her develop strategies to deal with this problem27.
Nurses are more likely to detect high alcohol consumption, FAS-associated facial abnormalities, and diagnostic criteria when instructed beforehand by training sessions on the subject. It is recommended the inclusion of more developed training programs for nursing students and nurses, in order to prepare professionals in this area. It is also advisable that all forms of interview and questionnaire continue to improve, in the hope that health teams will be able to act properly and in advance28.
A research performed by Korean professionals showed that the schooling of pregnant women and the fact of the pregnancy being desired or not also influenced the use of alcohol29.
Another study, carried out with Swedish pregnant women, reinforced the importance of schooling: almost all those interviewed said they had obtained sufficient information about the relationship between alcohol and risks for the baby from the country's investment in health and education. However, information prior to the discovery of pregnancy still needs to be improved30.
CONCLUSION
The two categories that emerged from the study - Prevention of alcohol consumption during pregnancy and detection of alcohol use and diagnosis of FAS - made it possible to reach the goal and explained the FAS prevention by health professionals.
It is essential to invest in education and awareness programs to publicize the problem and guide pregnant women to not drink alcohol. The offer of treatment to those, evidently, alcoholics, must also be a priority action, in the sense of minimizing the effects of alcohol on their children.
Interventions should be implemented at several levels: primary, secondary, educational and parental. The obstetrician nurse has a fundamental role in prevention, in the narrowing of the bond and in the early screening of FAS. And they must be imbued with communication tools such as the interview, the questionnaire, and the empathic approach to addressing prenatal alcohol problems. It is necessary to broaden the discussion at the level of preventive public policies that can reach and alert women about the deleterious effects of alcohol on pregnancy.
It is necessary to include this discussion in the curricula of undergraduate courses in the health area, considering the results discussed here, which revealed a lack of knowledge of the syndrome by medical professionals, obstetricians and nurses, and debate on the subject in Brazilian obstetric nursing forums.
As a limitation of this study, we can cite the non-discussion of the methodological rigor and probable biases of the articles selected and analyzed.
REFERENCES
1.Mesquita MA, Segre CAM. Malformações congênitas em recém-nascidos de gestantes consumidoras de álcool. Einstein 2010[cited in 2016 Jun 20]. 8(4 Pt 1):461-6. Available from: https://www.researchgate.net/profile/Conceicao_Segre2/publication/49596691_Congenital_malformations_in_newborns_of_alcoholic_mothers/links/0046351548cc2a68ad000000.pdf
2.Oliveira TR, Simões SMF. O consumo de bebida alcóolica pelas gestantes: um estudo exploratório. Esc Anna Nery. 2007. [cited in 2016 Jun 24].11(4):632-8. Available from: http://dx.doi.org/10.1590/S1414-81452007000400012
3.Costa LJS, Costa FS, Santos EC, Carvalho ACA, Pereira ES, Guimarães JA. Repercussões fetais do consumo materno de álcool. Femina . 2008. [cited in 2016 Jun 24]. 36(11):703-7. Available from: http://www.febrasgo.org.br/site/wp-content/uploads/2013/05/Femina_novembro2008-703.pdf
4.Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Pré-natal e puerpério. Atenção qualificada e humanizada: manual técnico. Brasília (DF): Ministério da Saúde; 2006.
5.Figueiredo PP, Lunardi Filho WD, Lunardi VL, Pimpão FD. Infant mortality and prenatal care: contributions of the clinic in the light of Canguilhem and Foucault. Rev Latino-Am Enfermagem. 2012. [cited in 2016 Jun 20]. 20(1):201-10. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-11692012000100026
6.Jomar RT, Abreu AMM. Intervenções breves para uso problemático de álcool: potencial de aplicação na prática do enfermeiro. Rev enfermUERJ. 2012; 20(3):386-90.
7.Mendes KDS, Silveira RCCP, Galvão CM. Revisão integrativa: método de pesquisa para a incorporação de evidências na saúde e na enfermagem. Texto Contexto-Enferm. 2008. [cited in 2016 Jun 24].17(4):758-64. Available from: http://www.producao.usp.br/handle/BDPI/3509
8.Souza MT, Silva MD, Carvalho R. Revisão integrativa: o que é e como fazer. Einstein. 2010;8(1Pt1):102-6.
9.Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Política nacional de atenção integral à saúde da mulher: plano de ação 2004-2007. Brasília (DF): Ministério da Saúde; 2004.
10.Bardin L. Analise de conteúdo. Lisboa (Pt): Edições 70; 2015.
11.Balachova TN, Bonner BL, Isurina GL, Tsvetkova LA. Use of focus groups in developing FAS/FASD prevention in Russia. Subs Use Misuse. [MEDLINE - Literatura Latino-Americana e do Caribe em Ciências da Saúde] 2007. [cited in 2016 jun 20]. 42(5):881-94. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2265734/
12.Jones HM, McKenzie A, Miers S, Russell E, Watkins RE, Payne JM. Involving consumers and the community in the development of a diagnostic instrument for fetal alcohol spectrum disorders in Australia. Health Research Policy and Systems. [MEDLINE- Literatura Latino-Americana e do Caribe em Ciências da Saúde]2013 [cited in 2016 jun 20]. 11:26. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23898969
13.Reis AT, Gama VC, Santos RS. Síndrome Alcoólica Fetal: reflexões para a prática de enfermagem obstétrica e neonatal. Revista de Pesquisa: Cuidado é Fundamental Online. 2010 [cited in 2016 Jun 20]. 2(4):1488-94. Available from: http://www.seer.unirio.br/index.php/cuidadofundamental/article/viewFile/972/pdf_
14.O'Connor MJ, Whaley SE. Brief intervention for alcohol use by pregnant woman. American Journal of Public Health. [MEDLINE- Literatura Latino-Americana e do Caribe em Ciências da Saúde]. 2007 [cited in 2016 jun 20]. 97(2):252-8. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1781394/
15.Chersich MF, Olivier L, Davies L, Chetty C, Viljoen D. Universal prevention is associated with lower prevalence of Fetal Alcohol Spectrum Disorders in Northen Cape, South Africa: a multicenter before-after study. Alcohol and Alcoholism. [MEDLINE- Literatura Latino-Americana e do Caribe em Ciências da Saúde]. 2012 [cited in 2016 jun 20].47(1):67-74. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22037537
16.Grant TM, Huggins JE, Sampson PD, Ernst CC, Barr HM, Streissguth AP . Alcohol use prior to and during pregnancy in Western Washington, 1989-2004: implications for preventing Fetal Alcohol Spectrum Disorders. Am J Obstet Gynecol. [LILACS- Literatura Latino-Americana e do Caribe em Ciências da Saúde] 2009 [cited in 2016 jun 20]. 200(3): 278.e1–278.e8. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2724985/
17.Tough S, Clarke M, Clarren S. Preventing fetal alcohol spectrum disorders. Canadian Family Physician. [MEDLINE- Literatura Latino-Americana e do Caribe em Ciências da Saúde]. 2005 [cited in 2016 jun 206]. 51:199-201. Available from: file:///D:/Ano%202016/artigos/Raissa/Artigos/5.5%2020Preventing%20fetal%20alcohol%20spectrum%20disorders(1).pdf
18.Rodrigues EM, Nascimento RG, Araújo A. Protocolo na assistência pré-natal: ações, facilidades e dificuldades dos enfermeiros da Estratégia de Saúde da Família. Rev Esc Enferm USP. [MEDLINE- Literatura Latino-Americana e do Caribe em Ciências da Saúde].2011 [cited in 2016 Jun 24]. 45(5):1041-7. Available from: http://www.scielo.br/pdf/reeusp/v45n5/v45n5a02
19.Garcia SAL, Garcia SAL, Lippi UG. A necessidade de inserção do enfermeiro obstetra na realização de consultas de pré-natal na rede pública. Einstein. [LILACS- Literatura Latino-Americana e do Caribe em Ciências da Saúde]. 2010 [cited in 2016 Jun 24]. (2):241-7. Available from: http://www.scielo.br/pdf/eins/v8n2/pt_1679-4508-eins-8-2-0241.pdf
20.Chudley AE, Conry J, Cook JL, Loock C, Rosales T, LeBlanc N. Fetal alcohol spectrum disorder: Canadian guidelines for diagnosis. CMAJ [MEDLINE - Literatura Latino-Americana e do Caribe em Ciências da Saúde]. 2005 [cited in 2016 jun 20]. 172 (5 supply): S1-S21. Available from: http://D:/Ano%202016/artigos/Raissa/Artigos/1.1%2020Fetal%20alcohol%20spectrum%20disorder%20Canadian%20guidelines%20for%20diagnosis(1).pdf
21.Chang G, Orav EJ, Jones JA, Buynitsky T, Gonzalez S, Wilkins-Haug L. Self-reported alcohol and drug use in pregnant young woman: a piloty study of prevalence and associated factors. J Addict Med. [MEDLINE- Literatura Latino-Americana e do Caribe em Ciências da Saúde] 2011[cited in 2016 jun 20] 5(3):221–6. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3157047/
22.Segre CAM. Síndrome Alcoólica Fetal. Pediatria Moderna. [LILACS- Literatura Latino-Americana e do Caribe em Ciências da Saúde]. 2012 [cited in 2016 Jun 24] 48(7):261-70. Available from: http://www.moreirajr.com.br/revistas.asp?fase=r003&id_materia=5091
23.Kfir M, Yevtushok L, Onishchenko S, Wertelecki W, Bakhireva L, Chambers CD. Can prenatal ultrasound detect the effects of in-utero alcohol exposure? A pilot study. Ultrasound Obstet Gynecol.[MEDLINE- Literatura Latino-Americana e do Caribe em Ciências da Saúde]2009[cited in 2016 jun 20] 33(6):683–9. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3746738/
24.Cassini C, Linden R. Exposição pré-natal ao etanol: toxicidade, biomarcadores e métodos de detecção. Rev Psiq Clín. [LILACS- Literatura Latino-Americana e do Caribe em Ciências da Saúde]. 2011 [cited in 2016 Jun 24] 38(3):116-2. Available from: http://biblioteca.versila.com/?q=exposi%C3%A7%C3%A3o+pr%C3%A9+natal+ao+etanol
25.Ismail S, Buckley S, Budacki R, Jabbar A, Gallicano GI. Screening, diagnosing and prevention of Fetal Alcohol Syndrome: is this syndrome treatable? Dev Neurosci. [MEDLINE- Literatura Latino-Americana e do Caribe em Ciências da Saúde] 2010 [cited in 2016 Jun 20] 32:91–100. Available from: http://www.karger.com/Article/Pdf/313339
26.Dias RD, Souza RM, Rodrigues DP, Alvez VH, Marchiori GR, Silva LA. O consumo de álcool e outras drogas na gestação: revisão integrativa. Rev Enferm UFPE on line [internet]. 2013[cited in 2014 Feb 12];7(12):7188-99. Available from: http://www.revista.ufpe.br/revistaenfermagem/index.php/revista/article/view/5395/pdf
27.Keough VA, Jennrich JA. Including a screening and brief alcohol intervention program in the care of the obstetric patient. JOGNN. 2009 [cited in 2016 Jun 20] 38:715-22. Available from: https://www.researchgate.net/publication/40023735_Including_a_Screening_and_Brief_Alcohol_Intervention_Program_in_the_Care_of_the_Obstetric_Patient
28.Zoorob RJ, Durkin KM, Gonzalez SJ, Adams S. Training nurses and nursing students about prevention, diagnoses, and treatment of fetal alcohol spectrum disorders. Nurse Educ Pract. 2014 [cited in 2016 jun 20] 14(4):338-44. Available from: http://www.nurseeducationinpractice.com/article/S1471-5953(13)00214-X/pdf
29.Lee SH, Shin SJ, Won SD, Kim EJ, Oh DY. Alcohol use during pregnancy and related risk factors in Korea. Psychiatry investig. 2010[cited in 2016 jun 20] 7(2):86–92. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2890873/
30. Holmqvist M , Nilsen P . Approaches to assessment of alcohol intake during pregnancy in Swedish maternity care--a national-based investigation into midwives' alcohol-related education, knowledge and practice. Midwifery. 2010[cited in 2016 jun 20] 26(4):430-4. Available from: http://www.midwiferyjournal.com/article/S0266-6138(08)00102-2/pdf