ORIGINAL RESEARCH
The learning process of students in practical activities of residency in obstetric nursing
Jane Márcia ProgiantiI; Juliana Amaral PrataII
I
PhD. Associate Professor. Maternal and Child Department of the School of
Nursing of Universidade do Estado do Rio de Janeiro. Rio de
Janeiro, Brazil. Email: jmprogi@uol.com.br
II
PhD. Assistant Professor. Maternal and Child Department of the School of
Nursing of Universidade do Estado do Rio de Janeiro. Rio de
Janeiro, Brazil. Email: juaprata@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2017.27792
ABSTRACT
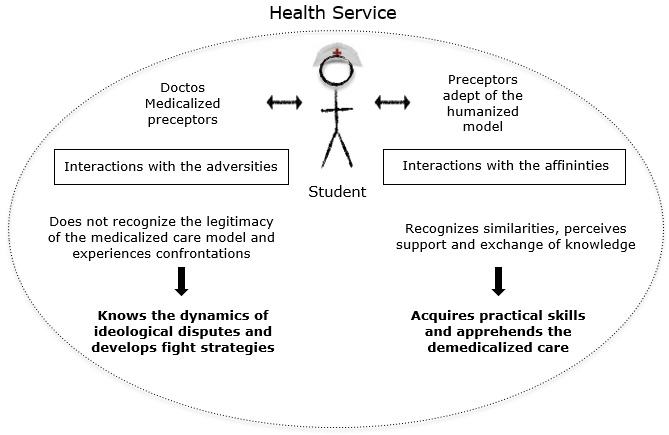
Objective: to examine students' learning process in practical activities of the Residency in Obstetric Nursing at Rio de Janeiro State University. Methodology: qualitative study of 13 obstetric nurses who graduated from this course, now working at municipal maternity hospitals in Rio de Janeiro. Data were collected by interview and interpreted using discourse analysis as a theoretical tool within an analytical framework given by the sociology of Pierre Bourdieu. Results: The learning process occurred on the basis of nurses' interactions with adversities, and the affinities they perceived in health services. In clashes with medicalized personnel, they came to understand the dynamics of ideological disputes, and developed fighting skills. From preceptors who favor humanization, they acquired practical skills and learned demedicalized care. Conclusion: The learning favored the formation of specialists disposed to administer noninvasive practices, to fight for demedicalization and to drive changes in the model of obstetric care.
Keywords: Obstetric nursing; teaching; humanization of assistance; women's health.
INTRODUCTION
In 2004, despite the lack of legislation that supported the training of obstetrical nurses through in-service training, the publication of the Qualification Program for Perinatal Care in the city of Rio de Janeiro, and the insufficient supply of specialists with experience in the care for normal births, resulted in a partnership between the Municipal Health Secretariat of Rio de Janeiro (SMS/RJ) and the School of Nursing of Universidade do Estado do Rio de Janeiro (ENF/UERJ) for the creation of the specialization course in obstetrical nursing in the modality of residency1-2.
This teaching model lasts two years, aiming at the development of skills and expertise based on knowledge and practices that favor the qualified insertion in the Unified Health System (SUS)3. Thus, the political and pedagogical project for the residency in obstetrical nursing of the Universidade do Estado do Rio de Janeiro (UERJ) is structured in 5,760 hours divided into theoretical, practical and theoretical, and practical subjects, where SMS/RJ is responsible for ensuring the teaching spaces in service and the delegation of preceptorship. ENF/UERJ is responsible for issuing the specialist degree, planning and evaluating the training process and providing the theoretical contents1-2,4.
Said course has the ideology of the unmedicated care of women's health as its guiding axis, conceiving nursing care as a shared construction, where obstetrical nurses are guided by the principle of non-invasion 1-2,4-6. From this point of view, the pedagogical work of the residency begins with the teachers, in 1,440 hours of the theoretical block. As for the 4,365 hours of the practical block, the residents are inserted in different obstetrical fields, places of apparent ideological disputes about the model of obstetrical attention (the medicated and the humanized)7.
In this sense, and considering that this professional training happens mainly in these health services, the purpose of this study was to analyze the learning process of the students along the practical block of the residency in obstetrical nursing of UERJ.
This research presents important contributions to the teaching of obstetrical nursing and to the training of human resources within the scope of SUS, since the studied course shows the singular process by which nurses apprehend the production of unmedicated care, capable of driving changes in the obstetrical care model.
THEORETICAL FRAMEWORK
It was used the concepts of field, struggle and symbolic violence developed by Pierre Bourdieu, who considers social fields as hierarchical and relatively autonomous spaces, which have their own values and objects that incite disputes between agents to impose their worldview and legitimize their representations as dominant. Within these places, agents (individuals or groups) are distributed hierarchically according to the volume of their capital, which determines their position and power8.
In this way, agents can be part of a field if they suffer in them or produce effects through symbolic struggles, which are those in which agents develop strategies to maintain themselves or improve their positions in the field9.
In the face of the relations of force established in the fields, those who find themselves in better positions exercise dominance over others by means of violence, usually symbolic, which translates into the imposition, without physical coercion, of the dominant culture, and the effectiveness lies in the recognition of its legitimacy9-10.
METHODOLOGY
This is a study with a qualitative approach11, extracted from the doctoral thesis The constitution of the professional habitus in the Course of Residency in Obstetrical Nursing of Universidade do Estado do Rio de Janeiro , linked to the project The process of implantation of the humanized model of assistance to childbirth and birth: The participation of the School of Nursing of Universidade do Estado do Rio de Janeiro in the reconfiguration of the obstetrical field , of the ENF/UERJ.
The participants were obstetrical nurses, who graduated from the obstetrical nursing residency course at UERJ, who work in municipal maternity hospitals in Rio de Janeiro. Those that develop a professional activity in other administrative spheres, in the private sector and/or in areas other than obstetrics are excluded. The participants' survey considered the period from 2004 to 2013, with a total of 56 graduates. After an initial telephone approach, only 26 met the pre-established criteria, of which 13 became participants in the study. This process took place from November 2014 to May 2015.
As a data collection technique, the interview was adopted, following a semi-structured instrument, which allowed the students' perceptions about the practical block of the residency to be captured. The interviews were recorded in digital audio files. The discourse analysis was used as the theoretical device of interpretation and the sociology of Pierre Bourdieu as an analytical reference. In this perspective, the interpretation and analysis of the interviews happened in stages that made possible the understanding of the meanings concretized in the discourses of each graduate12-13.
Initially, the transcription of verbal production was performed and, in order to preserve the intended meanings at the time of enunciation, the following symbols were inserted in the body of analysis: (Italic )Researcher's Comments, […]Suppression of parts of the statements, … Incomplete thinking, < Interruption of speech by the researcher, / Short pause in speech, // Long pause, ! Emphasis on sentence, - In conclusion of statement, (/) Unfinished statement.
By means of successive readings, the theoretical devices of discourse analysis (ideological forgetfulness, enunciative forgetfulness, paraphrase, interdiscourse, metaphor and polysemy) were identified, which made possible the apprehension of the discursive formations present in the participant's verbal production. Then, associating the discursive formations that presented the same origin, they were found to converge to an ideology, allowing the construction of a concentric model of analysis. Considering the conditions of discourse production, the relationship between discourse and ideology with imaginary formations was discussed, with Bourdieu's theoretical framework as the basis for the analysis of discursive processes.
Respecting Resolution number 466/2012 of the National Health Council 14, symbols were used to represent the authorship of the enunciations, with the letters E and T followed by numbers, which correspond to the order of interviewing and to the class. The research was approved by the Research Ethics Committee of UERJ under protocol number 33497214.8.0000.5282.
RESULTS AND DISCUSSION
Following a concentric model of analysis, it was verified that the learning process happened from the interactions of the students with the adversities and affinities present in the health services, as shown in Figure 1.
Figure 1: Aprendizagens adquiridas no bloco prático do curso de residência em enfermagem obstétrica da Universidade do Estado do Rio de Janeiro
The learning process of students in interactions with the adversities
As adversities found throughout the practical block of residency, the graduates pointed out the professionals who presented conducts and behaviors that did not conform to the guiding principles of the course.
It was a lot of fight! They (doctors) were caught in the middle ... They forced us to open episiotomy! When you put the patient upright, they lay the patient down! Oxytocin, they all had. Zero diet… (E12/T1)
This is very shocking! […] What is said in class is not what you experience! […] The technologies that we could offer depended on each field! We, not always, had the support of our preceptors, obstetrician nurses! (E3/T4)
The analysis of the discourses revealed that, when they entered the obstetrical fields as residents, they perceived the complexity of the health services and the dynamicity of the relationships in these places, which have conflicts involving professionals who are guided by different care models.
This reality is the result of the coexistence of agents formed by different worldviews so that the acquired conceptions generate different attitudes in the attention to the woman15. Thus, the obstetrical fields constitute spaces of ideological struggles where the professionals are engaged in constant disputes by the imposition of the worldview that conducts their obstetrical practices.
In this sense, the adherents of the humanized model develop practices that add new values to care, as they respect female protagonism and understand childbirth as a human event, inserted in the existential context of women. On the other hand, advocates of the medicated model conceive women as passive and childbirth as a pathological event. These differences in conceptions drive the struggles for dominance in the obstetrical fields 16-18.
In the health services that work as internship fields, although the training of obstetrical nurses is a challenge for the articulation between theory and practice2,19-20, it was verified that the present power relations appeared as adversities that provided important learning for the students, which resulted from the confrontations experienced with doctors and some preceptors adept of the medicated model.
The learning from the confrontations with the doctors
In the prolonged contact with the health services, the graduates reported that the practices developed and the instruments used by them generated confrontations with the medical professionals.
We managed to get the balls, they (the medical professionals) pierced them! We still did not have a birthing chair! We still did not have a stool! So what we did with the patients was put them in the tub, but we could not let the babies be born in the tub! So we had to pull them out and take them to the delivery room! (E12/T1)
If you got out of the box and the woman was with eight centimeters, they would already enter the room, lower the cervix, force the birth… (actions developed by the doctors) They did not have any respect for the job that you're doing … < But did you give in? / In most situations, yes! Because, even more when we are residents, we feel kind of / threatened / afraid of creating a confrontation. (E10/T5)
The above statements show some strategies adopted by doctors to interfere in the unmedicated performance of the residents who, through light technologies, contributed to female empowerment and to the parturition process with minimal intervention17-20.
From the perspective of the technologies used in health production, the light ones are based on relational processes so that the predominant option by this type of assistance technology directs the actions of the professionals to a care model that is characterized by the focus on human work and the act of the interaction with the individual and her subjectivities. This way of producing health care opposes the dominant medical model, centered on instrumental work, that is, on hard technologies 21.
From this perspective, the use of light technologies has given new meanings to the obstetrical care provided by the students and has produced representations about the unmedicated care model, which has been giving distinction and power to obstetrical nurses in the delivery and birth care, mainly in the City of Rio de Janeiro7,18,20,22-23.
Considering that in the dynamics of a field, every practice is visible and the agents are able to perceive the spontaneous differences as significant distinctions24, it is noticed that the unmedicated characteristics of the practices of the residents functioned as distinctive signs in the health services since, in those places, the interventions typical of the medicated model still predominate.
These distinctive signs refer to the properties and practices of an agent or group that characterize, classify and express differences, allowing the distancing of other agents. This distinction effect is established in the relation with the logic of a field so that the distinctive signs can confer profits and power to its bearers25-26.
In order to contain this distinction, the doctors reprimanded the attitudes, manifested imposing actions and damaged the instruments, disrespecting the residents' space of action in an attempt to prevent the reproduction of unmedicated care and, thus, preserve the dominant medicated order.
At such times, the dominance exercised by the doctors can be considered an explicit violence that resulted in an intimidation to the students' performance, where they abstained from fighting, avoiding the direct confrontation7. This finding reveals that in these interactions, the main learning for residents was to realize that obstetrical services are spaces for the elaboration of strategies for the symbolic struggle between the agents8-9.
The learning from the confrontations with the medicated preceptors
As part of the adversities perceived in the health services, the students recognized some preceptors who developed, as well as the doctors, interventionist practices in the care of the woman. In these relationships, they pointed out situations in which they felt intimidated to act according to the medicated worldview:
In practice, I learned episiotomy. / There were criteria to open an episiotomy! / There were some criteria that were imposed - I did not believe because I knew they were not true! And / to those people they were a truth, so, I found myself doing things I did not want to! (E3/T4)
It was not allowed in the box: "Is she in the expulsive stage? Let's take her to the delivery room!" / The woman stays horizontal and has to put her leg on the leg holder. […]- "Look, the baby is big! Are you not opening?" (reefers to the performance of the episiotomy) / "Everything will burst and you will have to suture by yourself!". (E13/T6)
In these statements, the participants detail interventionist conducts and behaviors that did not respect the physiology of the parturition process and the women's right to choose. Such obstetrical practices are commonly developed by practitioners adhering to the medicated model, even though official recommendations and scientific evidence consider them harmful or of judicious use23.
Moreover, the preceptors' imposing attitudes are evidences of the position of these agents in relation to the residents and of the exercise of a symbolic violence to legitimize their medicated conceptions. This type of violence is characterized by being soft, insensitive, invisible to its own victims, and its effectiveness will be greater the lesser the awareness of the agents involved is10.
Even if students often acted in disagreement with the principles of the theoretical teaching of the residency, it is interesting to note that they have not always been subordinated to the determinations of the medicated preceptors:
They had a different conduct. / More interventionist! But we did not get carried away by that and / we kept doing it the way we believed in! And they did not stop us! We said that's how we do it. Different! […] The way we learned! (E4/T2)
During residency, we learn a great deal about trusting what you are doing. […]In the theoretical foundation that you have that! So we could put it into practice even when that preceptor / were not really into it (/). (E5/T5)
These words reveal the interest of the students in the confrontations with these preceptors, because during the practical block of the course, what were at stake were spaces to develop unmedicated skills in the childbirth care. In this sense, they perceived the preceptors as closer agents in the hierarchy of the obstetrical fields and used the knowledge acquired in the theoretical block as instruments of struggle to face the attempts of domination and to act in the midst of the adversities of the predominant model in the health services.
The use of unmedicated conceptions and scientific knowledge was a strategy of resistance, which are commonly adopted by agents who contest the relations of force existing in a given field and aspire to legitimize their worldview8-9,27.
As a result of the relationship between a particular interest and a field, the strategies are evidence of the involvement of agents with the game so that when thinking and action schemes are adjusted with the dominant structure of the field, agents participate with conservation strategies. On the other hand, if there is a mismatch with the requirements contained in this place, agents can adopt strategies of subversion or withdrawal 28.
In this case, although the adopted strategy was not interested in the subversion of the medicated order of the obstetrical fields, the students realized that the confrontations with some medicated preceptors were reflected on their conduct:
They criticized, mocked our conducts, but sometimes you even saw them / by osmosis, / doing the same things that we did… The same orientations / non-invasive… […] So, I found it interesting because they / have an interventionist view, but at the same time, that was being absorbed by them! // And in a totally technocratic place… (E11/T6)
The above statement shows that the distinction existing in the unmedicated practices of the residents produced representations about obstetrical attention that contributed to the reconfiguration of the way of thinking and acting of some preceptors.
In this sense, it is possible to infer that, in predominantly medicated fields, the entrance of the students and their struggles for the development of the unmedicated care can favor the change of the assistance model in the health services from the mobilization of the professionals with new ideological conceptions. This effect is likely, since the principle of distinction incites disputes between agents, whether for the preservation or redefinition of dominant values in a field, so that interest in such a game is the condition of its functioning and, at the same time, the origin of its restructurings8,27.
Thus, the analysis of the discourses of the graduates revealed that, in the confrontations experienced with the medicated preceptors, they apprehended the disputes of the obstetrical fields from a different perspective from the ones they had with the doctors, understanding that when there is interest in the game, the participation in it becomes evident and, even in the face of the exercise of symbolic violence, it is necessary to invest in the struggle and to challenge the principles that structure the relations of power through strategies, which can modify the properties that underpin the authority in the field and subvert the dominant logic8,27.
The learning process of the students in the interactions with the affinities
Although the students have encountered adversities in the health services, they also recognized affinities as they interacted with preceptors adept of the humanized model, which allowed a learning process resulting from support and exchange of knowledge.
And we had those preceptors who supported us! […] but she could not put it into practice (humanized practices) because she did not have the support of anyone! […] with our presence there, she felt strengthened to the point of fighting! (E12/T1)
I stayed with a nurse who is a person / who does and / tests. / She did everything we saw there (in the classroom)! […] / Although // we were much criticized / by the doctors… / the nurse stood by our side! (E8/T3)
These statements show that when the preceptors shared the residents' worldview, the health services represented the continuity of the theory in the practice and they were encouraged to apply unmedicated conceptions even in the face of the adversities of the obstetrical fields.
On these occasions, students and preceptors presented similar schemes of thought and actions and manifested a certain homogeneity in obstetrical practices, characterizing agents with homologous dispositions25. Moreover, the mutual recognition of similarities constituted a network of solidarity among them that allowed the appropriation of knowledge, revealing the social capital present in these relations26.
Thus, the preceptors reaffirmed the feeling of belonging to the obstetrical nursing specialty and strengthened their unmedicated conceptions, empowering themselves for the ideological struggles of the obstetrical fields. On the other hand, the students have appropriated the practical knowledge of nurses and developed unmedicated skills for a non-invasive care to the woman during the parturition process.
CONCLUSION
It is concluded that, throughout the practical block of the residency in obstetrical nursing of UERJ, the learning process of the students happened as a result of diversified interactions in the health services, which, often, do not present structures consonant with the ideological principle of the course, the unmedicated care.
However, during interactions with the adversities, the residents perceived the meaning of the game in the obstetrical fields and the need to devise strategies of struggle to be able to gain practical skills. On the other hand, during interactions with the affinities, they apprehended the non-invasive care, which translates into the materialization of unmedicated conceptions.
In view of the above, it is noted that the practical teaching of obstetrical nursing in fields that coexist with ideological disputes of the care model translates into a pedagogical resource to increase the learning possibilities of the students.
REFERENCES
1.Universidade do Estado do Rio de Janeiro. Proposta de criação do curso de especialização em enfermagem obstétrica na modalidade de residência. Rio de Janeiro: Faculdade de Enfermagem; 2005.
2.Pereira ALF, Nicácio MC. Formação e inserção profissional das egressas do curso de residência em enfermagem obstétrica. Rev enferm UERJ[internet] 2014 [cited Jan 30, 2017]. 22(1):50-6. Available on: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/11418/8977
3.Brasil. Ministério da Educação. Resolução CNRMS n° 2 de 13 de abril de 2012. Dispõe sobre diretrizes gerais para os programas de residência multiprofissional e em profissional de saúde. Brasília, DF:2012. [cited Nov 23, 2016]. Available on: http://portal.mec.gov.br/index.php?option=com_docman&view=download&alias=15448-resol-cnrms-n2-13abril-2012&Itemid=30192
4.Universidade do Estado do Rio de Janeiro. Faculdade de Enfermagem. Projeto Político-Pedagógico do Curso de Residência em Enfermagem Obstétrica apresentado à Comissão Nacional de Residência Multiprofissional e em Área Profissional do Ministério da Educação.Rio de Janeiro: Departamento de Enfermagem Materno-Infantil; 2012.
5.Vargens OMC, Progianti JM. O processo de desmedicalização da assistência à mulher no ensino de enfermagem. Rev esc enferm USP[internet] 2004 [cited Dec 15, 2016]. 38(1): 46-50.Available on: http://www.ee.usp.br/reeusp/upload/pdf/92.pdf
6.Progianti JM, Lopes AS, Gomes RCP. A participação da enfermeira obstétrica no processo de desmedicalização do parto. Rev enferm UERJ[internet] 2003 [cited Dec 15, 2016].11: 273-7.Available on: http://www.facenf.uerj.br/v11n3/v11n3a06.pdf
7.Prata JA. A constituição do habitus profissional no Curso de Residência em Enfermagem Obstétrica na Universidade do Estado do Rio de Janeiro [tese de doutorado]. Rio de Janeiro: Universidade do Estado do Rio de Janeiro; 2016.
8.Bourdieu P. Questões de sociologia. Rio de Janeiro: Marco Zero; 1983.
9.Bourdieu P. O poder simbólico. 13 ed. Rio de Janeiro: Bertrand Brasil; 2010.
10.Bourdieu P. Dominação masculina. Rio de Janeiro: Bertrand Brasil; 2002.
11.Minayo MCS, Deslandes SF, Neto OC, Gomes R. Pesquisa social: teoria, método e criatividade. 21ª ed. Rio de Janeiro: Vozes; 2011.
12.Orlandi EP. Análise de discurso: princípios e procedimentos. 11 ed. Campinas (SP): Pontes; 2013.
13.Pêcheux M. Por uma análise automática do discurso. 4 ed. Campinas (SP): Editora Unicamp; 2010.
14.Brasil. Ministério da Saúde. Conselho Nacional de Saúde. Comissão Nacional de Ética em Pesquisa.Resolução n.º 466 de 13 de junho de 2012. Aprova as diretrizes e normas regulamentadoras de pesquisa envolvendo seres humanos. Brasília, DF:2012. [cited Dec 04, 2016].Available on: http://bvsms.saude.gov.br/bvs/saudelegis/cns/2013/res0466_12_12_2012.html
15.Vargens OMC, Progianti JM, Silveira ACF. O significado de desmedicalização da assistência ao parto no hospital: análise das concepções de enfermeiras obstétricas. Rev esc enferm USP[internet] 2008 [cited Dec 15, 2016].42(2): 339-46. Available on: http://www.redalyc.org/articulo.oa?id=361033330018
16.Mendonça SS. Modelos de assistência obstétrica concorrentes e ativismo pela humanização do parto. Civitas[internet]2015 [cited June 30, 2017]. 15(2): 250-71. Available on: http://revistaseletronicas.pucrs.br/ojs/index.php/civitas/article/view/17899
17.Sena AD, Santos TCS, Carvalho CMF, Sá ACM, Paixão GPN. Avanços e retrocessos da enfermagem obstétrica no Brasil. Rev enferm UFSM [internet] 2012 [cited June 28, 2017]. 2(3): 523-29. Available on: https://periodicos.ufsm.br/reufsm/article/view/3365
18.Gomes ML, M MAV. Modelo humanizado de atenção ao parto no Brasil: evidências na produção científica. Rev enferm UERJ [internet] 2012 [cited June 28, 2017]. 20(2): 248-53. Available on: http://www.facenf.uerj.br/v20n2/v20n2a18.pdf
19.Lima GPV, Pereira ALF, Guida NFB, Araújo CLF, Moura MAV. Expectativas, motivações e percepções das enfermeiras sobre a especialização em enfermagem obstétrica. Esc Anna Nery [internet] 2015 [cited June 28, 2017]. 19(4): 593-99. Available on: http://www.scielo.br/pdf/ean/v19n4/1414-8145-ean-19-04-0593.pdf
20.Vieira BDG, Moura MAV, Alves VH, Rodrigues DP. A prática dos enfermeiros obstetras egressos da especialização da Escola de Enfermagem Anna Nery. Rev enferm UERJ [internet] 2012 [cited June 27, 2017]. 20(esp1): 579-84. Available on: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/5802
21.Merhy EE, Franco TB. Por uma composição técnica do trabalho em saúde centrado no campo relacional e nas tecnologias leves: apontando mudanças para os modelos tecno-assistenciais. Saúde debate [internet] 2003 [cited Jan 19, 2017]. 27(65): 316-23. Available on: http://www.uff.br/saudecoletiva/professores/merhy/indexados-14.pdf
22.Vargens OM, Silva AC, Progianti JM. Non-invasive nursing technologies for pain relief during childbirth--the Brazilian nurse midwives' view. Midwifery[internet] 2013[cited 27 jun 2017]. 29(11):99-106. Available on: https://www.ncbi.nlm.nih.gov/pubmed/23481340
23.Gama SGN, Viellas EF, Torres JA, Bastos MH , Brüggemann OM, Theme Filha MM et a. Labor and birth care by nurse with midwifery skills in Brazil. Reprod health[internet] 2016[cited June 27, 2017]. 13(Suppl3): 226-65. Available on: https://reproductive-health-journal.biomedcentral.com/articles/10.1186/s12978-016-0236-7
24.Bourdieu P. Razões e práticas: sobre a teoria da ação. Campinas (SP): Papirus; 1997.
25.Bourdieu P. A distinção: crítica social do julgamento. São Paulo: Edusp; 2007.
26.Bourdieu P.O capital social notas provisórias. IN: Nogueira MA, Catani A, organizadores. Escritosde Educação. 3 ed. Petropólis (RJ): Vozes; 2001. p. 65-9.
27.Bourdieu P. A economia das trocas simbólicas. São Paulo: Perspectiva; 1999.
28.Bourdieu P. Coisas Ditas. São Paulo: Brasiliense; 1990.