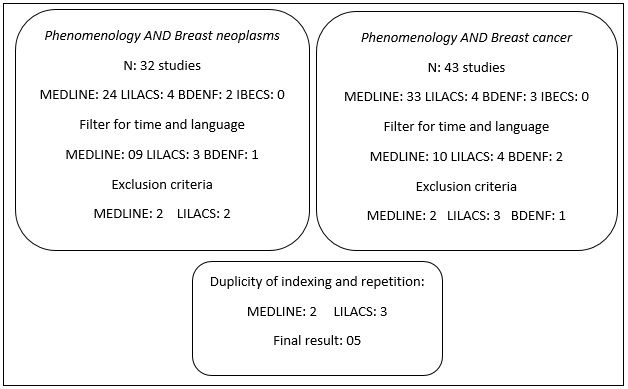
FIGURE 1: Result of the search with the descriptors Phenomenology AND Breast neoplasms and Phenomenology AND Breast cancer.
ORIGINAL RESEARCH
Contributions by phenomenological research into breast cancer: an integrative review
Marlise Barros de MedeirosI; Rose Mary Costa Rosa Andrade SilvaII; Eliane Ramos PereiraIII; Sérgio Henrique Silva MeloIV; Fabiana Lopes JoaquimV
I
Nurse. Master student of the Graduate Program of the Aurora Afonso Costa
Nursing School. Niterói, Rio de Janeiro, Brazil. E-mail: marlisemedeiros@gmail.com
II
Full Professor at the Aurora Afonso Costa Nursing School, Fluminense
Federal University. Niterói, Rio de Janeiro, Brazil. E-mail: roserosa.uff@gmail.com
III
Full Professor at the Aurora Afonso Costa Nursing School, Fluminense
Federal University. Niterói, Rio de Janeiro, Brazil. E-mail: elianeramos.uff@gmail.com
IV
Nurse. Master student of the Graduate Program of the Aurora Afonso Costa
Nursing School. Niterói, Rio de Janeiro, Brazil. E-mail: shsmelo@gmail.com
V
Nurse. PhD student of the Graduate Program of the Aurora Afonso Costa
Nursing School. Niterói, Rio de Janeiro, Brazil. E-mail: fabykim_enf@yahoo.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2018.26486
ABSTRACT
Objective: to examine the production of knowledge about breast cancer from the phenomenological perspective. Methods: integrative review of publications in the MEDLINE, LILACS, IBESC and BDENF databases. Results: the study reviewed eight articles discussing the experiences of women and their families, contributing to the humanization of care, secondary prevention and early detection of breast cancer. This underlines the need to understand the subjectivities involved in this process in order to develop more effective care programs. Conclusion: knowledge production on breast cancer from a phenomenological perspective is important, and contributes both to nursing care and to guiding public policies for breast cancer control.
Descriptors: Oncology nursing; women›s health; breast neoplasms; phenomenology.
INTRODUCTION
Breast cancer is the most frequent neoplasm in women in Brazil and in the world, presenting a high mortality rate and constituting a public health problem and one of the priorities for the development of research in Brazil 1,2. As the cancer affects many areas in the life of women, the treatment of breast cancer takes place in a multidisciplinary way, with the need for services of mastology, oncology, radiology, nursing, nutrition, physiotherapy, psychology and social service. Treatment approaches include surgery, chemotherapy, radiotherapy, hormone therapy, use of molecular targeted and supportive drugs3,4.
The surgical modality for treatment of breast cancer is often considered as a mutilator, responsible for triggering negative impacts on women's self-image because the breasts are related to femininity, sexuality and maternity, and this loss affects both physical and psycho-emotional aspects. Chemotherapy, a dreaded treatment step, causes alopecia, fatigue, gastrointestinal disorders and other symptoms that also affect women's lives5. In this context, care plays a role in the control of signs and symptoms and, above all, as an aid to meet the needs of women in a humanized and individualized way, enabling the achievement of quality life.
Phenomenology, as a methodological proposal, seeks to ground, in new requirements, the conditions of science, with the intention to know where the scientific knowledge of a concrete or empirical science gains support, starting from the immediate data of consciousness. It is understood as the study of a given phenomenon, what corresponds to what is present in the consciousness, in order to explore it, to unveil the meaning and to achieve what the thing is, that is, the essence6.
It is a philosophy that emerged in Germany with Edmund Husserl in the late nineteenth century and was established as an important philosophical current in the twentieth century. Husserl had as influences the thought of Plato, Descartes and Brentano. The thinkers Martin Heidegger, Alfred Schütz, Jean Paul Sartre and Maurice Merleau-Ponty had the influence of Husserl's thought6.
The phenomenological approach has as its guiding principle the existentialist philosophy, having as starting point the experience of the subject who is being-in-the-world. It is a methodology that requires the rigorous description of the experience; it seeks neutrality through the reduction of assumptions, but values the subjectivity and singularity of each narrative that are inherent to the human being seeking to understand it7.
Phenomenology has been used in the health area as a theoretical and methodological support in researches that seek the comprehensive analysis of the human being, providing subsidies for care improvements, deepening of ontological and ethical issues and various aspects of the humanization of care7.
Thus, it is relevant to know the scientific production regarding breast cancer in the phenomenological perspective, because the care of women in the context of breast cancer requires humanization. In this context, the objective of this study was to analyze the production of knowledge about breast cancer from a phenomenological perspective.
METHODOLOGY
This is an integrative review of literature that allowed an approximation of the problem to be studied, drawing a overview about its scientific production and allowing to know the evolution of the theme over time and thus identifying possible research opportunities8.
The following steps were taken: identification of the theme and selection of the research question; establishment of criteria for inclusion and exclusion of articles (sample selection); identification of pre-selected and selected studies; categorization; analysis and interpretation of results; presentation of the review8. The question chosen to guide the study was: What is the scientific production about breast cancer from a phenomenological perspective?
The search was carried out in the portal of the Virtual Health Library (VHL) and the chosen databases were:Medical Literature Analysis and Online Retrieval System (MEDLINE), Latin American and Caribbean Literature in Health Sciences (LILACS), Spanish Bibliographical Index of Health Sciences (IBESC) and Nursing Database (BDENF).
The descriptors breast neoplasms, phenomenology and qualitative research and nursing care identified through the Health Sciences Descriptors (DeCSs) and the Medical Subject Headings (MEHS) were used. The use of the descriptor breast cancer was identified in the literature and this was used to cover the research. We used the Boolean operator AND and the intersection of the descriptors. The search took place from July to August 2016.
Inclusion criteria were articles on breast cancer developed from a phenomenological perspective, indexed in the selected databases, published in Portuguese, English and Spanish, available online in full length and published in the period from 2010 to 2015 aiming at an updated review. As exclusion criteria, theses, dissertations, monographs, reviews and reflection articles were not considered; texts non-available online in full length and articles not available for free were not considered.
For the previous evaluation of the studies, the abstracts and articles were read in full legnth. A data collection instrument was used, containing the identification of the article (title, objective, method, journal, country and year).
RESULTS AND DISCUSSION
Crossing the descriptors phenomenology AND breast neoplasms resulted in the retrieving of four articles. When the descriptors phenomenology AND breast cancer were crossed, we obtained five articles, four of which had already been identified in the previous search, as shown in Figure 1.
FIGURE 1: Result of the search with the descriptors Phenomenology AND Breast
neoplasms and Phenomenology AND Breast cancer.
Crossing the descriptors qualitative research AND breast neoplasms and nursing care resulted in four articles. With the descriptors qualitative research AND breast cancer and nursing care, six texts were identified. After the analysis of duplicity of indexation and repetition, the search resulted in four publications, according to Figure 2.
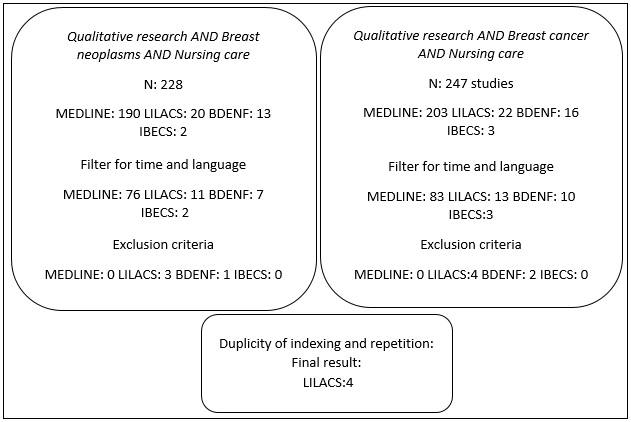
FIGURA 2: Result of the search with the descriptors Qualitative research AND Breast neoplasms AND Nursing care
and Qualitative research AND Breast cancer AND Nursing care.
The evaluation of the findings of Figure 1 and Figure 2 showed that one article was repeated in LILACS, resulting in eight articles, 2 (25%) in MEDLINE and 6 (75%) in LILACS. The publications selected and included in the study9-16 are presented and described in Figure 3, in chronological order of publication.
As for the method, Heidegger was used as theoretical and methodological reference in 4 (50%) articles. As for the country, 6 (75%) studies are Brazilian and 2 (25%) are North American. Regarding the year, 2 (25%) were published in 2011, 2 (25%) in 2012 and 4 (50%) in 2015.
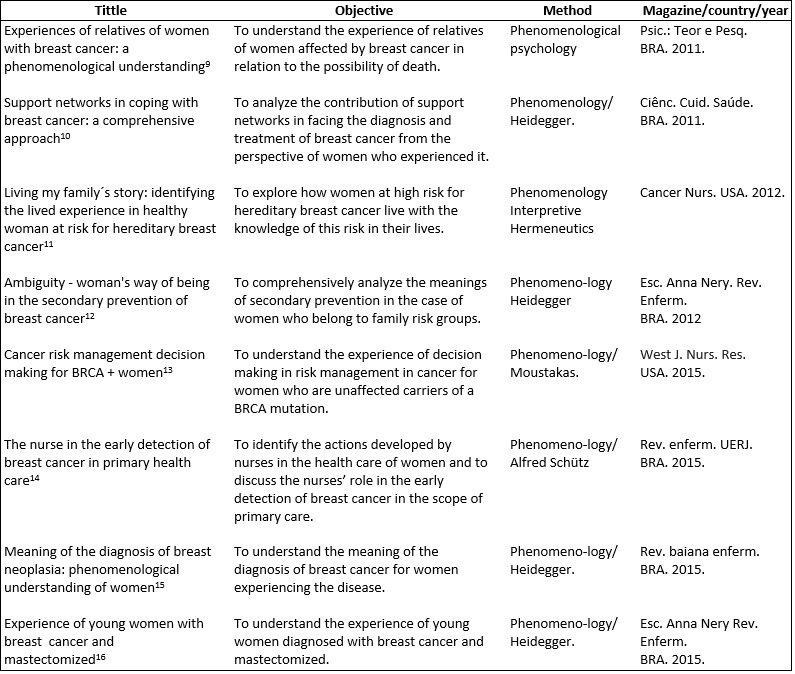
FIGURE 3:
Demonstration of the publications included in the study, in chronological
order of publication. Integrative review held in 2016.
Four categories emerged from the analysis of the data in the selected studies: The experience of women; The experience of family members; Secondary prevention; and Early detection in primary care.
The experience of the woman
The experience of women with breast cancer was discussed in three studies that approached the support network for women with breast cancer, the meaning of the diagnosis and the experience of breast cancer by young women 10, 15, 16.
It was identified that when experiencing the diagnosis and treatment of breast cancer, a support network consisting mainly of family members, friends and health professionals is fundamental. Family and friends are the main contributors to the coping with the disease and are also motivators for adherence to treatment and promoters of feelings of embracement, security and optimism.
The nursing team is recognized as indispensable for the solidification of support networks. However, the study addresses how health professionals can make it difficult for women to assimilate and accept the disease by choosing to condition them to receive the diagnosis as something common to other people, ignoring the particular meaning for each patient, and promoting the inauthenticity of the individual10.
The significance of the diagnosis of breast cancer is particular, but commonly feared. In the intent to understand the significance of the diagnosis of breast cancer for women who experience it under Heidegger's phenomenological approach, feelings and reactions of emotion, fear, rejection of diagnosis or conformism experienced by women were revealed. The inauthentic characteristic of the denial of the diagnosis was identified. Modes of fear, dread, and horror emerged in discourses characterizing impropriety-for-death due to the finitude that becomes evident15. A study that also sought to know the meaning of breast cancer had similar results with respect to denial and fear of death 17.
The issue of inauthenticity is a peculiar part of Heidegger's thought. This thought refers to the mode of being of impersonal occupation, where the human being avoids all personal responsibility by adhering to the talk, the opinion of the masses, in which man understands himself on the basis of that others establish as a way of existing, not in what he is and chooses to be. Inauthentic human beings are dominated by chattiness, ambiguity and curiosity, and these things determine the very mode of being of de-cadence. Based on the contributions of the Heideggerian philosophy in this study, a liberating and promoting care of the women's authenticity is proposed, leading them to recognize themselves as beings of possibilities and protagonists of their history15, 18.
It is considered that a care plan that promotes authenticity is only exercised by professionals who understand the human being in this perspective. Therefore, the Heideggerian philosophy is relevant for the training of health professionals, because knowing and caring for others is closely related to knowing and caring for oneself.
Breast cancer is infrequent in young women, and when it occurs at this stage, it is usually associated with a more aggressive typology, with more negative impacts in life. In the discovery of the disease, there are reactions of denial permeated by despair and sadness, anguish of having been affected by the disease so early, fear of an uncertain future and fear of death, as well as feelings of guilt and failure16. Other studies have shown similar results, evidencing the negative impact caused by the diagnosis15,17,19.
Difficulties related to public health services are experienced, such as bureaucracies and a long waiting time to start the treatment16. Despite the legal guarantee of starting treatment within 60 days after diagnosis, waiting time is still an obstacle in many cases and can cause harm to patients, such as disease progression and decreased survival 20,21.
The side effects of chemotherapy were mentioned as impacting due to nausea and vomiting, fatigue and alopecia, a result similar to other studies 22-24. The experience of alopecia stood out, with reports that its impact is more intense than the experience of mastectomy16. This finding is related to factors related to self-image that is highly valued socially, especially by young women. Alopecia is more evident than mastectomy and women feel more exposed to the perception of the others.
Mastectomy brought about the need for acceptance of a new image. Acceptability of breast loss was greater due to the idea that the disease is eliminated with this procedure16. The impact of mutilation is related to the appreciation of the breast and the way women perceive their own bodies and the disease. At this point, subjectivities are more important than the biophysical notion of the body.
The conception of body is related to the meaning that the individual gives to the body and to influences from social relations. The conception of the body reflects the very identity of the subject; when someone speaks of the own body, speaks of oneself. Therefore, the impact of mastectomy and alopecia affects the woman's identity, her way of seeing herself and of relating to the world25,26.
The overcoming of cancer during the stages of diagnosis and treatment was related to the ability of accepting, overcoming and seeking rehabilitation. The search for support at that time revealed the need for religiosity/spirituality, aiming at self-understanding, tranquility, optimism and motivation to live16. In this sense, Heidegger's hermeneutics collaborates in understanding the anguish as an opening to new possibilities of existence and search for meaning.
The experience of family members
When cancer happens, it has implications for the affected person and his relatives or close circles of relationships. Family members experience the stigma of the disease, fear of pain and suffering, and have to face the possibility of death and loss of the loved one. Because cancer is a dreaded disease and it is associated with small chances of cure, it also generates fear and insecurity on the part of relatives who expressed the need for guidance and support from specialized professionals9.
It is thus important to emphasize that relatives are important references to support cancer patients, but they are often as shaken and fearful as patients, requiring themselves to be supported and welcomed by the multidisciplinary team and, so that they may be promoters of the care they are asked for.
The studies address the importance of health professionals to consolidate the necessary support network for women with breast cancer 9,10, 16. It is relevant that patients and family members be welcomed and heard so that when they understand their representations of the disease and the treatment demands may be identified, encompassing physical, emotional, existential and social aspects. The bond with the relatives allows for a meaningful dialogue that allows flexibility of strategies, opening new existential horizons and a new meaning to life in the search of overcoming this experience and the need for care.
Secondary prevention
Three studies approaching secondary prevention were included in this category11-13. Two studies interviewed women's first-degree relatives of breast cancer patients and one study interviewed women with the genetic mutation, BRCA + that predisposes to breast cancer.
A Brazilian study identified a lack of accurate knowledge about secondary prevention in a group of women at high risk for breast cancer associated with the hereditary factor. Thus, there was no recognition of the condition of high risk for breast cancer neither a decisive attitude before the risk. From the narrated experiences, analyzed according to Heidegger's thought, a condition of inauthenticity, ambiguity and inappropriate condition for death was revealed12.
The North American studies pointed out that the high-risk condition for breast cancer (by hereditary factor or presence of BRCA) influenced the search for self-care measures, early detection and the expression of the need for support from health professionals in the management process of the decision making, in view of the proposed modalities for the prevention/early diagnosis of the disease11,13. Experiences of fear and distress were identified in these studies, but a great difference was observed in relation to the Brazilian study in terms of the search for secondary prevention. A more decisive attitude of search for care was identified, through guidance and support from specialized professionals, management of secondary prevention options, and decision-making about therapeutic options.
The need for creating competence in the area of oncogenetics was evidenced, mainly in Brazil. The support from specialized professionals is a requirement of both patients and family members who seek information and assistance in decision-making, training for care and self-care. The studies show the importance of the performance of the competent nurses not only in the assistance aspect, but also in the educational aspect in the scope of oncology27,28.
Another relevant aspect is the issue of accessibility to genetic testing, specifically the BRCA testing, sold in the United States in pharmacies. In Brazil, the test still has a high cost and is not so accessible to the entire population. The use of new technologies in the health area brings not only advances but new ethical and bioethical implications, being essential the technical and human training of professionals who work with such technologies in the context of cancer, so that they may be able to analyze the favorable and unfavorable aspects and always benefit the life and health of individuals, thus avoiding therapeutic futilities.
Caution is needed in the approach to women in this risk group because the intention is to provide support for decision-making. Decision-making, in turn, is concerned with whether or not to identify the genetic risk and its degree, whether or not to make necessary examinations periodically, maintaining active surveillance and/or subsequently deciding on the necessary secondary prevention modalities, including prophylactic mastectomy and hormonal (surgical or drug) castration. Women may make the decision for not to investigate and refuse any secondary prevention measures, but must, however, be guided to decide freely. This choice must be respected, since active surveillance and intervention on a risk for many women means already living in the pathological condition.
Early detection in primary care
One Brazilian study in the scope of primary care, with nurses' narratives and based on Schultz's thinking, identified the attention to breast care only in the pregnancy and puerperal period. This is an alarming finding because in Brazil there are many cases of late diagnosis of breast cancer that results in lower survival rates and quality of life, with an impact on mortality rates. Early detection is essential to change this profile and the effective performance of primary care professionals is important 14.
The professionals' qualification of the basic health network for the practices of early detection is of extreme importance. This training involves constant updating regarding the ministerial recommendations for the early detection of breast cancer and the evaluation of the degree of conformity of this practice among professionals. In addition to this training, studies point to the need to restructure the current model of the Unified Health System; this structuration is a great challenge to achieve better results in the care of women with breast cancer21,29,30.
CONCLUSION
The approximation of nursing to the phenomenological approach aims at the understanding of the human being, patients, relatives or nurses to subsidize a more humanized, integral and ethical care, because the fragmented vision of the body and the technicality poses a distance between professionals and this perspective and causes deficiencies in care, with serious impacts on the health of the population.
Phenomenology brings possibilities of constructing a new way of thinking the man, proposing to nursing a form of care that aims, firstly, at understanding of the others and, from this, opens the possibility of helping the others to attribute a new meaning to their life in the face of the distress caused by health problems.
In relation to secondary prevention and early detection, the need to understand the subjectivities involved in this process to develop more effective care programs according to the needs of Brazilian public health stood out.
REFERENCES
1. Ministry of Health (Br). José Alencar Gomes da Silva National Cancer Institute. Estimate 2016: incidence of cancer in Brazil [Internet]. Rio de Janeiro; 2015 [cited in Sep 14, 2017]. Available from: http://www.inca.gov.br/estimativa/2016/estimativa-2016-v11.pdf
2. Ministry of Health (Br). National Agenda for Health Research Priorities [Internet]. Brasília; 2011 [cited in Sep 14, 2017]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/agenda_nacional_prioridades_2ed_3imp.pdf
3.Silva CB, Albuquerque V, Leite J. Quality of life in patients with breast cancer undergoing chemotherapy. Rev. Bras. Cancerol. [Internet]. 2010 [cited in Sep 15, 2017]; 56 (2): 227-36. Available from: http://www1.inca.gov.br/rbc/n_56/v02/pdf/08_artigo_quality_vida_carriers_neoplasia_mamaria.pdf
4. Bonassa EMA. Nursing in cancer therapy. 3rd ed. São Paulo: Atheneu; 2012.
5. Nicolussi AC, Sawada NO. Quality of life of breast cancer patients in adjuvant therapy. Rev gaúch enferm. [Internet]. 2011 [cited in Sep 15, 2017]; 32 (4): 759-66. Available from: http://seer.ufrgs.br/index.php/RevistaGauchadeEnfermagem/article/view/20027/1445
6.Oliveira e Silva JM, Lopes RLM, Diniz NMF. Phenomenology. Rev. bras. enferm [Internet]. 2008 [cited in Sep 25, 2017]; 61 (2): 254-7. Available from: http://www.scielo.br/pdf/reben/v61n2/a18v61n2.pdf
7.Gomes AMA, Paiva ES, Valdés MTM, Frota MA, Albuquerque CM. Phenomenology, humanization and health promotion: a proposal for articulation. Health soc. [Internet]. 2008 [cited in Sep 25, 2017]; 17 (1): 143-52. Available from: http://www.scielo.br/pdf/sausoc/v17n1/13.pdf
8.Botelho LLR, Cunha CCA, Macedo M. The method of integrative review in organizational studies. Management and Society. [Internet]. 2011 [cited in Oct 10, 2017]; 5 (11): 121-36. Available from: https://www.gestaoesociedade.org/gestaoesociedade/article/view/1220
9.Ambrósio DCM, Santos MA. Family experiences of women with breast cancer: a phenomenological understanding. Psic .: Content. and Pesq. [Internet]. 2011 [cited in Oct 20, 2017]; 7 (4): 475-84. Available from: http://www.scielo.br/pdf/ptp/v27n4/11.pdf
10.Andrade GN, Panza AR, Vargens OMC. Support networks in coping with breast cancer: a comprehensive approach. Ciênc. Cuid. Saúde. [Internet]. 2011 [cited in Oct 20, 2017]; 10 (1): 82-8. Available from: http://www.periodicos.uem.br/ojs/index.php/CiencCuidSaude/article/view/10609
11.Underhill ML, Lally RM, Kiviniemi MT, Murekeyisoni C, Dickerson SS. Living my family's story: identifying the lived experience in healthy women at risk for hereditary breast cancer. Cancer Nurs. [Internet]. 2012 [cited in Oct 20, 2017]; 35 (6): 493-504. Available from: https://www.ncbi.nlm.nih.gov/pubmed/22544165
12.Melo MCSC, Souza IEO. Ambiguity: woman's way of being in the secondary prevention of breast cancer. Esc Anna Nery Rev. Enferm. [Internet]. 2012 [cited in Oct 20, 2017]; 16 (1): 41-8. Available from: http://www.scielo.br/pdf/ean/v16n1/v16n1a06.pdf
13.Leonarczyk TJ, Mawn BE. Cancer risk management decision making for BRCA + women. West J. Nurs. Res. [Internet]. 2015 [cited 2017 Oct 20]; 37 (1): 66-84. Available from: http://wjn.sagepub.com/content/37/1/66.full
14.ZapponiI ALB, Tocantins FR, Vargens OMC. The nurse in the early detection of breast cancer in primary care. Rev. enferm. UERJ. [Internet]. 2015 [cited in Oct 20, 2017]; 23 (1): 33-8. Available from: http://www.facenf.uerj.br/v23n1/v23n1a06.pdf
15.Paiva ACPC, Salimena AMO, Souza IEO, Melo MCSC. Meaning of the diagnosis of mammary neoplasia: phenomenological understanding of women. Rev. baiana enferm. [Internet]. 2015 [cited in Oct 20, 2017]; 29 (1): 59-67. Available from: https://portalseer.ufba.br/index.php/enfermagem/article/viewFile/12239/9543
16. Almeida TG, Comassetto I, Alves KMC, Santos AAP, Silva JMO, Trezza MCSF. Experience of young woman with breast cancer and mastectomized. Esc. Anna Nery Rev. Enferm. [Internet]. 2015 [cited in Oct 20, 2017]; 19 (3): 432-8. Available from: http://eean.edu.br/detalhe_artigo.asp?id=1318
17.Rosa LM, Radunz V. Meaning of breast cancer in women's perception: from symptom to treatment. Rev. enferm. UERJ. [Internet]. 2012 [cited in Oct 20, 2017]; 20 (4): 445-50. Available from: http://www.facenf.uerj.br/v20n4/v20n4a06.pdf
18.Heidegger M. Being and time. Translation by Fausto Castilho. Campinas (SP): Unicamp; 2012.
19.Caetano EA, Gradim CVC, Santos LES. Breast cancer: reactions and coping when receiving the diagnosis. Rev. enferm. UERJ. [Internet]. 2009 [cited in Oct 27, 2017]; 17 (2): 257-61. Available from: www.facenf.uerj.br/v17n2/v17n2a21.pdf
20. Federal Government (Br). Law No. 12,732, of November of 2012. It provides on the first treatment of patients with proven malignant neoplasia and establishes term for its beginning. Brasília (DF): Graph of the Senate; 2012.
21. Sousa CBS, Fustinoni SM, Amorim MHC, Zandonade E, Matos JC, Schirmer J. Study of the time between the diagnosis and the beginning of the treatment of breast cancer in the elderly women of a reference hospital in São Paulo, Brazil. Ciênc. Saúde coletiva. [Internet]. 2015 [cited Oct 27, 2017]; 20(12): 3805-16. Available from: http://www.scielo.br/pdf/csc/v20n12/1413-8123-csc-20-12-3805.pdf
22.Guimarães AGC, Angels ACY. Sociodemographic characterization and quality of life evaluation in women with breast cancer in adjuvant chemotherapy treatment. Rev. Bras. Cancerol. [Internet]. 2012 [cited in Oct 28, 2017]; 58(4): 581-92. Available from: http://www.inca.gov.br/rbc/n_58/v04/pdf
23. Gozzo TO, Moysés AMB, Silva PR, Almeida AM. Nausea, vomiting and quality of life of women with breast cancer undergoing chemotherapy. Rev. gaúch enferm. [Internet]. 2013 [cited Oct. 28, 2017]; 34 (3): 110-6. Available from: http://www.scielo.br/pdf/rgenf/v34n3/a14v34n3.pdf
24.Lôbo SA, Fernandes AFC, Almeida PC, Carvalho CML, Sawada NO. Quality of life in women with breast neoplasms undergoing chemotherapy. Acta paul. enferm [Internet]. 2014 [cited in Oct 28, 2017]; 27 (6): 554-9. Available from: http://www.scielo.br/pdf/ape/v27n6/1982-0194-ape-027-006-0554.pdf
25.Azevedo RF, Lopes RLM. Body design in Merleau-Ponty and mastectomized women. Rev. bras. enferm [Internet]. 2010 [cited in Oct 27, 2017]; 63 (6): 1067-70. Available from: http://www.scielo.br/pdf/reben/v63n6/31.pdf
26.Merleau-Ponty M. Phenomenology of perception.4th ed. São Paulo: Martins Fontes; 2015.
27.Seenandan-Sookdeo KA, Hack TF, Lobchuk M, Murphy L, Marles S. Parental decision making regarding the disclosure or nondisclosure of a mutation-positive BRCA1/2 test result to minors. Oncol. Nurs. Forum. [Internet]. 2016 [cited in Oct 29, 2017]; 43 (3): 330-41. Available from: https://www.ncbi.nlm.nih.gov/pubmed/27105194
28. Underhill ML, Dickerson SS. Engaging in medical surveillance: understanding the personal meaning of breast surveillance. Oncol. Nurs. Forum. [Internet] 2011 [cited 2017 Oct 29]; 38 (6): 686-94. Available from: https://www.ncbi.nlm.nih.gov/pubmed/22037331
29.Rosa LM, Radünz V. From symptom to adjuvant treatment of women with breast cancer. Text & context enferm. [Internet]. 2013 [cited in Oct 27, 2017]; 22 (3): 713-21. Available from: http://www.scielo.br/pdf/tce/v22n3/v22n3a18.pdf
30.Marques CAV, Silva VRS, Gutiérrez MGR. Nurse actions in the early detection of breast cancer. Rev. enferm. UERJ. [Internet]. 2017. [cited in Jan 13, 2018]; 25: e22639. Available from: http://www.epublicacoes.uerj.br/index.php/enfermagemuerj/article/view/22639/22340