(*) TRS = Renal replacement therapy
ORIGINAL RESEARCH
Dialysis patient satisfaction with nursing care
Ingrid Fernanda de Oliveira VieiraI; Felipe Kaezer dos SantosII; Frances Valéria Costa e SilvaIII; Silvia Maria de Sá Basilio LinsIV; Natasha Cristina Cunha MunizV
I
Nurse. Nursing Trainee, Universidade do Estado do Rio de Janeiro. Brazil.
E-mail:
ingridfoliveira@hotmail.com
II
Nurse. Assistant Professor, Universidade do Estado do Rio de Janeiro.
Brazil. E-mail: felipe.santos@uerj.br
III
Nurse. PhD in Health Sciences. Adjunct Professor, Universidade do Estado do
Rio de Janeiro. Brazil. E-mail: francesvcs@gmail.com
IV
Nurse. PhD in Nursing. Assistant Professor, Universidade do Estado do Rio
de Janeiro. E-mail: silviamarialins@gmail.com
V
Nurse. Nursing Trainee, Universidade do Estado do Rio de Janeiro. Brazil.
E-mail: natasha.cunha84@yahoo.com
DOI: http://dx.doi.org/10.12957/reuerj.2018.26480
ABSTRACT
Objective: to examine dialysis patient satisfaction with related nursing care. Method: this descriptive study was conducted, on a quantitative field approach, from May to August 2016, at a university hospital in Rio de Janeiro. The sample comprised 37 patients over 18 years old, who had been on hemodialysis or peritoneal dialysis at the hospital for three months or more. Data were collected using a patient satisfaction questionnaire. Results: overall patient satisfaction was 3.89 for the three items: education, trust, and theoretical and practical skill, with hemodialysis patients returning 3.69 overall satisfaction, and peritoneal dialysis patients, 4.44. Conclusion: patients in peritoneal dialysis at the hospital were satisfied with the nursing care provided.
Descriptors: Patient satisfaction; nursing; nephrology; nursing care.
INTRODUCTION
Chronic Kidney Disease (CKD) is an abnormality of renal structure or function that consists of a clinical syndrome present for a period of three months or more. The glomerular filtration rate and albuminuria is adopted for staging it.1
To cope with it, it is necessary to intervene with the health team to reduce the morbidity and mortality caused by CKD, allowing the optimization of early diagnosis of the disease, immediate referral for nephrological treatment and implementation of measures to preserve renal function when caring of the patient.2
The nurse, when inserted in the specialty of nephrology, has its field of practice expanded when aiding, management, legal and social responsibility, teaching, research, promotion, contributing to the recovery of the patient's health and coping capacity in each treatment type.3,4 The nurse also has a great commitment to the quality of care provided to the patient, to the institution, based on ethics, laws, professional standards, valuing patient care and satisfaction.5
Nursing care involves acting, thinking and relating their care focused on the human being, identifying the individual needs of each patient and providing means of care that will fit the treatment of the subject, thus contributing to a better quality of life for the patient. Nurses, in providing their assistance, reflect their representations and individualities in different relationships, such as in therapy, trust and technique, thus establishing an interpersonal relationship, which will influence adherence to the treatment and prolongation of the patient's life.6,7
One strategy used by health organizations to learn about patient satisfaction is the Patient Satisfaction Instrument (PSI), which consists of evaluating the patient's perception, expectation and satisfaction regarding the quality of nursing care and the quality of the health service provided under the social aspects of care, the intrapersonal character and the operational aspect of the nurse, which aims to obtain information regarding the quality of care received by the patient.5,8
The main objective of this study was to analyze the satisfaction of patients on dialysis in relation to nursing care. As specific objectives, this study aims to present the degree of satisfaction of patients on dialysis with nursing care and to discuss the differences and similarities of the education, confidence and theoretical-practical knowledge of patients undergoing hemodialysis (HD) and peritoneal dialysis (PD).
Its potential contribution to the area is based on the relationship of teaching, research and practice in seeking to highlight possible facilitators and difficulties of the nurse-patient relationship. By knowing patient satisfaction, nurses can establish a greater understanding of their clients, favoring the construction of a trust link with the subject and consequently an improvement, readaptation or continuity of the care provided, contributing to the evaluation of the institution and nursing care itself.
LITERATURE REVIEW
When nurses' care and assistance in nephrology are related, the professionals' performance stands out in some specific areas of this specialty: in acting with patients still in conservative treatment, in working with patients who will be or are submitted to renal transplantation and in the two modalities of dialysis: hemodialysis and peritoneal dialysis.
When caring for people with CKD, the nurse should pay attention to the complications of the disease, stress and anxiety that involve this condition. Initially, when the subject is still on conservative treatment, the objectives will be based on the aid of reducing the rate of progression of renal disease, maintaining renal function and improving the clinical, psychological and social conditions of the subject.9
The nurse in the context of renal transplantation seeks to guide and assist the patient in adherence to treatment and follow up, find the best way to pass the guidelines, seeking the joint participation of the patient and his family; seek the best way to fight against problems that may be inevitable; exercise the role of care and education in a way that contributes significantly to the success of transplantation and whenever possible, accompany the patient from the beginning of the evolution of his illness to achieve a better quality of life through the procedure and perceive the possible deficiencies found, staying close to the patient and acting strategically.10
PD is the mode of renal replacement therapy (RRT) that stands out most when it comes to self-care. The patient should take control of his own treatment and be aware of his own care through activities developed by him to perform the dialysis procedures, care with the catheter and its surroundings, prevention of complications, among others. In this context, the nurse assumes an important educational role: to prepare patients and family members to take the dialysis procedures, encouraging them to be responsible for their care, with the help of the family and to give autonomy to this care.11
In HD, the nurse, when preparing the individual for the procedure, should establish a relationship of trust with the him and seek to encourage him to question, learn to avoid complications, ask questions and promote self-care, which will specifically contribute to the integrity, balance of organic functions and preservation of vascular access. The professional should encourage the patient to be non-passive in the treatment, prompting him to pay attention to the physical and physiological changes that occur during CKD.12
By listening to what patients must report on the care they are given and their satisfaction, the chance of constructing an outcome indicator that points managers to some decisional paths of change and innovation is evident. The nurse, in turn, can become aware of his/her responsibility towards the quality of care provided to the patient, institution, ethics, laws and standards of the profession, as well as contributing to the appreciation and performance of patient care and satisfaction.5
METHODOLOGY
This is a quantitative approach descriptive and transversal study carried out in a university institution located in the city of Rio de Janeiro, State of Rio de Janeiro, where the specialty of nephrology is divided into three sectors: HD, PD and clinical nephrology and renal transplant ward.
The sample consisted of 37 subjects, being used as inclusion criteria the carriers of CKD who perform the dialytic treatments (PD and HD) associated with the institution with treatment time equal to or greater than three months, of both genders and over 18 years old. Patients in HD with acute renal disease, transplant patients who did not require HD and/or PD, and patients who failed to respond to the questionnaire were excluded from the study.
Data were collected from May to August 2016 in the nephrology sector. The study participants were the patients who attended the site for consultations of PD or for the performance of HD.
After explaining the study objectives and, in case of positive participation, the signing of the Informed Consent Form (ICF) was requested and the questionnaire to be answered was handed out.
If the patient had a deficiency (visual, for example) or some difficulty in understanding the questionnaire, which interfered with their self-application, the researcher's help was requested.
The project was approved by the Ethics and Research Committee of Hospital Universitário Pedro Ernesto /UERJ, under opinion No. 1,436,717. The aspects of Resolution No. 466/2012 of the National Health Council were respected.
For the data collection, the following questionnaire was used: Patient Satisfaction Instrument (PSI). It is an instrument adapted and validated in Brazil, from the original developed by Hinshaw and Atwood (1982) to be applied in hospitalized patients, denominated Patient Satisfaction Instrument (PSI). It aims to measure patient satisfaction with nursing care.8
It consists of 25 closed questions that seek to assess patient satisfaction in relation to the following domains: technical-professional area, educational relationship and trust; the items are answered using scores from the five-point scale of the Likert type, ranging from totally agree (five points) to totally disagree (one point), and the higher the score, the higher the level of satisfaction. 13
For the technical-professional and trust domain, the research has seven items for each, which addresses technical issues of care and situations related to the nurse's attitudes, respectively. For the trust domain, the research presents 11 items about situations involving the interpersonal relationship between the nurse and the patient.13
The answers to the questionnaires were typed, constituting a database in the Excel 2007® software. For the descriptive statistical analysis, the STATA MP 13.0 software was used, which provided the arithmetic mean and the confidence interval of the results of the variables obtained.
RESULTS AND DISCUSSION
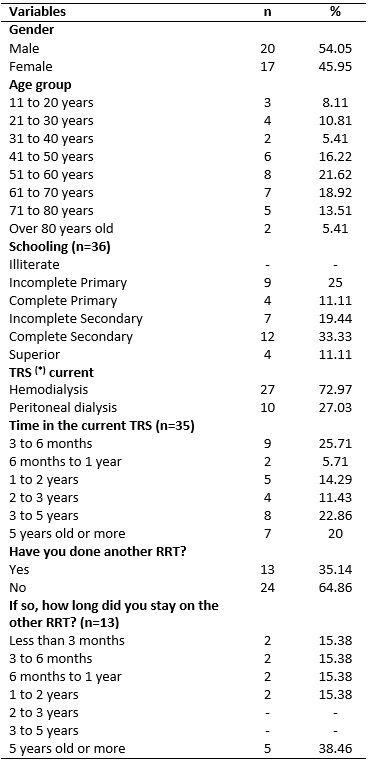
The results showed that most of the interviewees were male, with 20 (54.05%) subjects. The predominant age group was between 51 and 60 years old, with 8 (21.62%) patients, followed by the age group from 61 to 70 years old, with 7 (18.92%). Most of the interviewees had a complete secondary education, with 12 (33.33%) people, followed by incomplete primary education, with 9 (25%) people, as shown in Table 1.
TABLE 1:
Characterization of subjects interviewed. Rio de Janeiro, 2016. (37)
(*)
TRS = Renal replacement therapy
The largest number of patients interviewed underwent HD, 27 (72.97%). Patients who underwent PD therapy were 10 (27.03%).
The arithmetic mean and confidence intervals of the values found on the satisfaction of the patients interviewed regarding nursing care in renal replacement therapies are listed in Table 2.
TABLE 2:
Overall satisfaction of patients regarding nursing care in renal
replacement therapies. Rio de Janeiro, 2016.
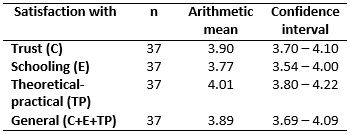
Patients, in general, were satisfied in the three aspects analyzed: confidence, education, theoretical-practical, with a mean of 3.89 on a scale ranging from 1 to 5, and the higher the score, the greater the level of satisfaction of the interviewees.
The data reinforce the importance of the role of the nurse during the care process. When building a bond with the patient, the professional created a relationship of trust and safety with the care received. This favors communication and consequent improvement in the quality of care provided. It is worth noting that the evaluation of the patient regarding the care provided is based on situations that involve the attention, trust, empathy and involvement on the part of the professional that provides his assistance and not only in the accomplishment of the technical procedures and that the assessment occurs in different ways because it depends on the individuality of each subject.8
It is observed that the aspect with the lowest score was related to education. The individual with CKD needs to be guided on various aspects of their treatment: the illness itself, the forms of renal replacement therapy, risks and benefits of each therapy modality, diet, medication use, water restriction, among others. The guidance provided through educational actions is essential to enable self-care, to increase adherence to the therapeutic regimen, to reduce the complications resulting from the treatment and to help identify the client's needs, which interfere with their quality of life.14
The nurse has the responsibility of actively participating in the implementation of educational programs that meet the individual needs of patients, follow their journey, evolution and reflect on their behaviors to help them enjoy the quality of life possible within their health status and condition.14
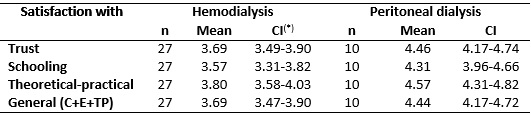
Patient satisfaction in each of the modalities of renal replacement therapy, hemodialysis and peritoneal dialysis is shown in Table 3.
TABLE 3:
Satisfaction of patients in each modality of renal replacement therapies in
relation to the nurse's care. Rio de Janeiro, 2016.
(*)
CI = Confidence Interval
Despite the non-quantitative equivalence of patients in each modality, PD patients have a higher overall satisfaction rate (4.44) than HD patients (3.69). In each of the three aspects, if analyzed separately, PD patients also presented higher means than HD patients.
One of the factors that can justify the difference in the values found is the PD dynamic, which service is anchored in a close relationship between nurse and patient, from the qualification process to home dialysis, strengthening support and accountability bonds. Another finding is in the fact that the patients who undergo PD have twice a month contact with the clinic professionals. On the other hand, HD patients undergo on-site therapy three times a week, with an average duration of four hours, which allows greater stress situations between patients and employees. 15
The systematization of the autonomous interventions of the nurse in the great areas of the specialty of nephrology are realized when the professional starts to integrate a holistic approach in the representation of a global perspective of the care. This allows to include other areas of attention directed to the person in its dimensions, with the aim of providing the capacity for self-care, identification of complications and the accomplishment of the treatment in the context of nephrology. 16
In the PD context, nurses consider as the focus of their care the specific training of the patient and his caregiver for the procedure and self-care, in addition to routine follow-up of this practice, through nursing consultations. By informing, encouraging and supporting the process of adaptation to the requirements of the method, the professional provides the reach of a good general level of information regarding PD and its peculiarities, the patient is led to the understanding that a method is a universe endowed with innumerable specificities.17
The nurse will help in the existence of a protection factor, which will culminate in a better quality of the dialysis technique. By having a patient-professional relationship, it is possible to deepen, in a unique and specific way, the patient's expectations, desires and feelings, which will culminate in the deepening of questions related to PD, their care and peculiarities.17,18
In HD, the focus of care is mainly during dialysis, where the patient, the dialyzer and the dialysate need constant monitoring and evaluation. The nurse performs the important surveillance function to avoid complications that may occur during the procedure, such as gas embolism, inadequate or excessive ultrafiltration (hypotension, cramps, vomiting), blood leakage and contamination of the route, which demands constant attention and time on the part of the professional.12
A major challenge for the nurse working in HD is the preparation of the patient, who may not understand the impact of dialysis and the learning needs may go unnoticed, which makes self-care difficult, which establishes actions that follow a model of recommendations, contributing in a specific way in the integrity, in the balance of the organic functions and in the preservation of the vascular access.12 The nurse, besides working with the patients in the implementation of this procedure, plays an important role in the education of this subject in guiding him about the functioning of HD, which will facilitate actions for the search of self-care, in the implementation of drug and nutritional therapy, helping him understand the importance of adherence to treatment so that the patient can live well.14
Finally, it should be emphasized that professionals should be concerned with studying the quality of their care, because it is through the patients' perception that a change is made between the practice of care, which allows to know the aspects considered most significant when being assisted. Considering that nurses' perceptions of care vary according to patients' characteristics, culture, expectations, personal factors and illness, it is necessary for nurses to measure these influences to adjustand to follow up with the assistance offered, in order to examine the low points and overcome them, thus guaranteeing the quality of care and customer satisfaction.19-22
CONCLUSION
It is concluded that the patients in the hospital's dialysis treatment are satisfied with the nursing care provided to them.
However, it is necessary that professionals working in the area know the results obtained and their meanings, so that they can reflect, review them or continue their care, ensuring their quality.
The aspects of trust, education and theoretical-practical knowledge analyzed by the research are items that are a constant part of the nurse's care. It is worth mentioning that the item that reached the lowest index of satisfaction, whether in the general index or in the index of each of the two dialytic modalities was the education. The following question is pertinent: are the strategies used enough to carry out health education with patients? Are there enough resources (personal, material, financial) to practice health education with these patients? Is there a real interest on the part of the professional to carry out health education?
The study had as limitations the non-quantitative equivalence of subjects interviewed in each dialytic modality, and the small sample, which does not allow the generalization of the findings.
Finally, recognizing the results presented in the study contributes to the recognition of the quality of service of the nurses working in the HD and DP units of the health institution, even before the difficulties faced by the hospital and the service.
REFERENCES
1.Magalhães FG, Goulart RMM. Doença renal crônica e tratamento em idosos: uma revisão integrativa. Rev. Bras. Geriatr. Gerontol. 2015; 18: 679-92.
2.Bastos MG, Kirsztajn GM. Doença renal crônica: importância do diagnóstico precoce, encaminhamento imediato e abordagem interdisciplinar estruturada para melhora do desfecho em pacientes ainda não submetidos à diálise. J. Bras. Nefrol. 2011; 33: 93-108.
3.Pennafort VPS, Furtado AM, Fialho AVM, Moreira TMM, Freitas MC, Queiroz MVO. Produção do conhecimento científico de Enfermagem em Nefrologia. Rev. Bras. Enferm. (Online). 2010; 63: 830-36.
4.Carvalho IMP, Melo RL, Andraus LMS. Produção científica de enfermagem em nefrologia, no Brasil, no período de 1989 até 1999. Rev.eletron. enferm. 2001 [Access 2017 Sep 18]; 3. Available from: http://www.fen.ufg.br/revista
5.Freitas JS, Silva AEBC, Minamisava R, Bezerra ALQ, Sousa MRG. Qualidade dos cuidados de enfermagem e satisfação do paciente atendido em um hospital de ensino. Rev. latino-am enferm. (Online). 2014; 22: 528-30.
6.Rodrigues TA, Botti NCL. Cuidar e o ser cuidado na hemodiálise. Acta Paul. Enferm. (Online). 2009; 22: 528-30.
7.Bisca MM, Marques IR. Perfil de diagnósticos de enfermagem antes de iniciar o tratamento hemodialítico. Rev. bras. enferm. 2010; 63: 435-9.
8.Oliveira AML, Guirardello EB. Satisfação do paciente com os cuidados de enfermagem: comparação entre dois hospitais. Rev. Esc. Enferm. USP. 2006; 40: 71-7.
9.Roso CC, Beuter M, Kruse MHL, Girardon-Perlini NMO, Jacobi CS, Cordeiro FR. O cuidado de si de pessoas em tratamento conservador da insuficiência renal crônica. Texto & contexto enferm. 2013; 22: 739-45.
10.Furtado AMO, Souza SROS, Oliveira BL, Garcia CN. El enfermero asistencial y educador en una unidad de trasplante renal: un desafío. Enfermería Global. 2012; 27: 346-50.
11.Sadala MLA, Bruzos GAS, Pereira ER, Bucuvic EM. A experiência vivida pelos pacientes em DP domiciliar: uma abordagem fenomenológica. Rev. latino-am enferm. 2012; 20: 68-75.
12.Moreira AGM, Araújo STC, Torchi TS. Preservação da fístula arteriovenosa: ações conjuntas entre enfermagem e cliente. Esc. Anna Nery Rev. Enferm. 2013; 17: 256-62.
13.Oliveira AML. Satisfação do paciente com os cuidados de enfermagem: adaptação cultural e validação do Patient Satisfaction Instrument [master thesis]. Campinas (SP): Universidade Estadual de Campinas; 2004.
14.Santos I, Rocha RPF, Berardinelli LMM. Necessidades de orientação de enfermagem para o autocuidado de clientes em terapia de hemodiálise. Rev. bras. enferm. 2011; 64: 335-42.
15.Gonçalves FA, Dalosso IF, Borba JMC, Bucaneve J, Valerio NMP, Okamoto CT, et al. Qualidade de vida de pacientes renais crônicos em hemodiáliseou diálise peritoneal: estudo comparativo em um serviço de referência de Curitiba - PR. J. Bras. Nefrol. 2015; 37: 467-74.
16.Sousa CN. Cuidar da pessoa com fístula arteriovenosa: modelo para a melhoria contínua. Revista Portuguesa de Saúde Pública. 2012; 30: 11-7.
17.Santos FK, Valadares GV. Conhecendo as estratégias de ação e interação utilizadas pelos clientes para o enfrentamento da DP. Esc. Anna Nery. Rev. Enferm. 2013; 17: 423-31.
18.Santos FK, Valadares GV. Conhecendo o mundo do ser que enfrenta a diálise peritoneal: nexos simbólicos presentes no cotidiano. Rev. enferm. UERJ. 2011; 19:473-8.
19.Contreras CCT. Percepción de la calidad del cuidado de enfermería en pacientes hospitalizados. Avances en enfermería. 2010; 28: 98-110.
20.Abreu IS, Santos CB. Qualidade de vida relacionada à saúde de pacientes em hemodiálise. Rev. enferm. UERJ. 2013; 21(1):95-100.
21.Sousa MRG, Silva AEBC, Bezerra ALQ, Freitas JS, Neves GE, Paranaguá TTB. Prevalência de eventos adversos em uma unidade de hemodiálise. Rev. enferm. UERJ. 2016; 24(6):e18237.