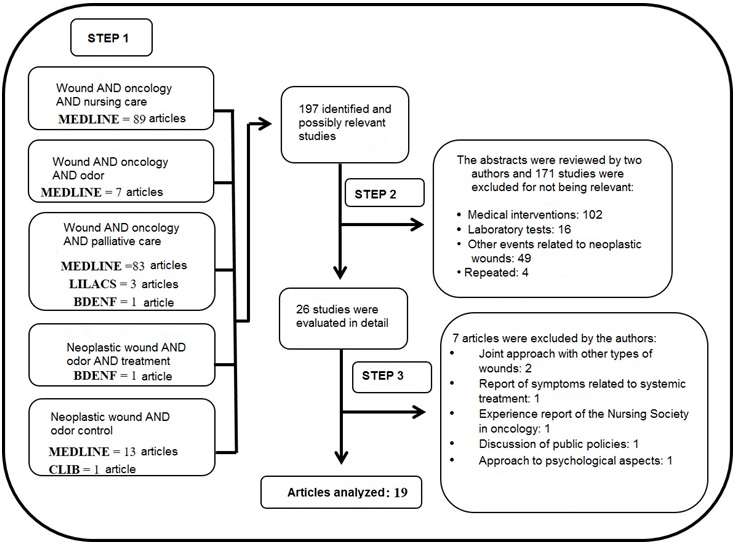
FIGURE 1: Flowchart of article evaluation search strategy. Recife, 2016
REVIEW ARTICLE
Variables associated with neoplastic wound odor control: knowledge for nursing care
Antonio Carlos NarcisoI; Nauã Rodrigues de Souza II; Marcos Antonio de Oliveira SouzaIII; Fátima Maria da Silva AbrãoIV; Givaneide Oliveira de Andrade Luz V; Isabel Cristina Ramos Vieira SantosVI.
I
Nurse. Master student, Associate Program of Post-Graduation in Nursing.
University of Pernambuco/State University of Paraíba. Recife, Pernambuco,
Brazil. E-mail:
profcarlosnarciso@yahoo.com.br
I
Nurse. Master student, University of Pernambuco/State University of
Paraíba. Recife, Pernambuco, Brazil. E-mail: nauan_1@hotmail.com
III
Nurse. PhD student, University of Pernambuco/State University of Paraíba.
Recife, Pernambuco, Brazil. E-mail: socramef@gmail.com
IV
Nurse. PhD student. University of Pernambuco/State University of Paraíba.
Recife, Pernambuco, Brazil. E-mail: abraofatima@gmail.com
V
Nurse. PhD student, University of Pernambuco/State University of Paraíba.
Recife, Pernambuco, Brazil. E-mail: givaneide.giva@gmail.com
VI
Nurse. PhD, University of Pernambuco/State University of Paraíba. Recife,
Brazil. E-mail: tutornad@yahoo.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2017.26036
ABSTRACT
Objective: to analyze variables that are important to building nurses' knowledge of neoplastic wound odor control. Method: this integrative review, conducted in 2016, in Nursing Database, Latin American and Caribbean Health Sciences database, Spanish Bibliographic Index in Health Sciences, Medical Literature Analysis and Retrieval System online and the Cochrane Library, selected 19 articles published on the subject from 2002 to 2015. Results: three knowledge dimensions were identified: self-assessment, scientific and technical knowledge, competences and abilities, and 26 variables related to them. Technical and scientific knowledge was more highly valued, as reflected by the higher number of variables cited. Conclusion: the results may contribute to improving nurses' understanding of the necessary requisites for building and refining knowledge about controlling this symptom which is challenging to health personnel and patients, and will benefit managers and researchers in building performance evaluation tools.
Keywords: Medical oncology; wounds;odor; nursing care.
INTRODUCTION
Neoplastic, malignant or oncological wounds occur when cells from a primary or metastatic cancer invade the epithelium, seep into the supporting blood and lymphatic vessels, and penetrate the epidermis. This results in a loss of vascularization and consequent reduction of nutrition to the skin, leading to tissue necrosis1.
Among the prevalent symptoms, such as pain, exudate, odor, bleeding and necrosis, the unpleasant and foul odor emanating from these wounds, related to necrosis and infection, is a cause of greater discomfort and isolation of the affected patients2-6.
Odor associated with wounds that rarely heal often manifests when the patient is in the palliative phase of the disease process, and may be more devastating than actually living with the cancer diagnosis due to extreme physical, psychological, emotional, and spiritual stress. This brings a greater challenge for their care7-12.
Scientific knowledge of the principles of palliative care is essential for the process of caring for oncological patients affected by wounds 6. In fact, since the perspective of healing of these injures is remote, palliative care focuses on two crucial approaches: physical and psychological. However, the physical symptoms of these injuries are closely related to psychological manifestations6,9,13.
The nurse has a fundamental role in the care of these patients and for this purpose, nurses need to have the knowledge and technical competence to evaluate and treat these injuries, providing an individualized and comprehensive care to them and their families14. Nursing knowledge will enable them to justify actions or even avoid the use of unsafe practices. To this end, there is the additional challenge of continuous professional development, since nursing knowledge is constantly evolving15-17.
Given this, one may ask: what is the body of knowledge that nurses must have to provide quality care to these patients? And what are the dimensions that permeate this knowledge? The answer to these questions will contribute to the practice of nursing as well as to elucidate useful parameters for the research and management of services regarding the evaluation of professional performance.
Thus, the objective of this study was to analyze important variables for the construction of nurses' knowledge on the odor control of neoplastic wounds. It is intended, therefore, to seek a more meaningful understanding of the dimensions understood by this knowledge and its variables.
METHODOLOGY
The search for evidence-based practices has led to an increase in the production of all kinds of literature reviews, and although the systematic review and meta-analysis are the most important and most widely used methods, they often do not comprise essential issues related to nursing care18.
In this perspective, the method used in this research to search for variables associated with odor control in neoplastic wounds was the integrative review of the literature, since the combination of research methods under different epistemological matrices may provide useful results to achieve the goal.
Six different stages were followed, as recommended by experts19. The guiding question was structured from the PICOD system, that is, after considering: the target population (P), the interest of the area (I), types of intervention or care (C), obtaining results and considering the effects to be achieved (O) and study design (D), resulting in the expression: what are the important variables for the construction of nurses' knowledge for odor control of neoplastic wounds?
The following inclusion criteria were used to search for articles: given the relation of the subject of interest and palliative care, the minimum limit for the publication period was the year 2002, set as a milestone in the updated definition of palliative care by the World Health Organization 20, and the maximum limit was the year 2015. Only free access articles published in Portuguese, English and Spanish languages were selected.
Both the terms odor control and neoplastic wound are not registered in the Descriptors in Health Sciences (DeCS) or in Medical Subject Headings (MeSH). Therefore, as a search strategy, we chose the following descriptors: wounds, oncology, odor, treatment, nursing care and palliative care, combined with each other or with the two key words of the guiding question.
We used the Boolean operator and due to the necessity of linking the descriptors in order to integrate the research theme. In the search strategy, the following databases were used: Nursing Database (BDEnf), Latin American and Caribbean Literature in Health Sciences (LILACS), Spanish Bibliographic Index in Health Sciences (IBECS), Medical Literature Analysis and Retrieval System Online (MEDLINE) and the Cochrane Library (CLIB). The data collection was carried out in the months of January and February of 2016.
The search initially found 197 articles and the reading of their abstracts led to the selection of 26 of them. These were read in full in order to verify the compliance with the guiding question, thus totalizing 19 articles to be analyzed, as seen in Figure 1.
FIGURE 1:
Flowchart of article evaluation search strategy. Recife, 2016
The categorization of the studies and the arrangement of the findings were carried out using an instrument built by the authors, using the software Excel 2016, to enable the systematization of the research and to facilitate the individual evaluation of each study, consisting of the following variables: database used, journal, article title, authors, year of publication, type of research/methodology, and variables associated with odor control.
It was interpreted as a variable associated with odor control any reference obtained from the analyzed article, either by citation or deriving from the result thereof. Initially the variables were read by two researchers and then grouped according to the dimensions emanated from the semantic analysis of the word knowledge.
RESULTS AND DISCUSSION
Of the 19 articles analyzed, 14 resulted from MEDLINE, two from LILACS, two from BDENF and only one from CLIB. Comparing with the number originally found in the first stage of selection, we can see the small number of studies addressing the odor control of neoplastic wounds, as shown in Figure 1.
Data have shown that the greater frequency of articles comes from nursing journals, since, of the 19 articles analyzed, 12 had been exclusively elaborated by nurses2-7,10,15-17,21,22, four had been resulting from their association with physicians23-26 and three had been conducted by physicians12, 27. This, a priori, demonstrates that odor control in neoplastic wounds is part of the scope of nursing and has become a concern of nurses and, as such, comprises part of the knowledge collection of this profession, according to Figure 2.
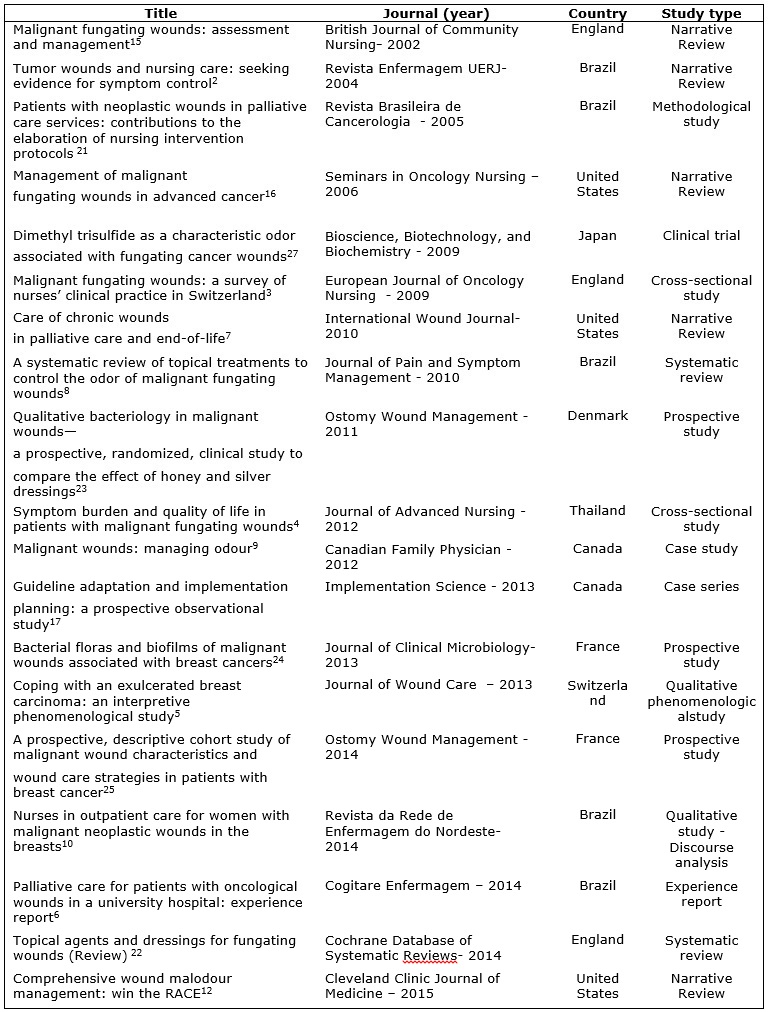
FIGURE 2
: Characteristics of articles included in the integrative review according
to title, journal, year, country and type of study. 2002-2015.
From a broad debate on nursing practices, caring for the patient with neoplastic wound is a challenge that requires knowledge focused on a palliative paradigm, from which the nurse needs to understand and have the skills not only to deal with physical symptoms, but also with the psychological impact associated with the patient's wound and the implications for their families5,6.
It is also observed the occurrence of publications on this theme in all the years considered in the analyzed period. However, there has been a growth of these publications from 2009, with more frequency of articles in the year 2014 (n = 4), as seen in Figure 2.
There has been a larger number of Brazilian publications (n = 5), followed by those from England and the United States, both with three publications. This may denote, at first, the leading position of Brazilian production in comparison with other countries. However, when classifying publications by continents, the Americas (n = 10) predominated with publications on the subject, followed by the Europe (n = 7) and Asia (n = 2).
Also, due to the relationship between cancer and aging, global incidence rates in the developed world are double those seen in the developing world and, in those countries, the relationship between health resources and knowledge application to cancer control have led to a significant increase in survival and the need for palliative procedures, which include those related to odor control in the neoplastic wound, with consequent prior disclosure28,29.
Regarding the type of study, it was evidenced that the theme odor control in neoplastic wounds has been approached in several ways, among which the narrative review is the most frequent (n = 5), followed by quantitative studies: prospective (n = 3), cross-sectional (n = 2), systematic review (n = 2), clinical trial (n = 1), case studies (n = 1) and case series (n = 1). See Figure 2.
So that nurses have adequate control of odor in neoplastic wounds, they need to have knowledge and this results basically from the association between education and experience, and for that, they must interpret and integrate into their practice the best scientific evidence available.
The narrative reviews are among the publications that synthesize findings of primary studies on the phenomenon of interest. In fact, these studies favor the definition of the problem, the field and the disciplines that constitute it, allowing the ready comprehension of the object necessary to the basic and initial knowledge on the subject30. This is a plausible reason for the expressive number of narrative reviews found in this study.
In spite of the significant number of qualitative studies, mainly conducted in Brazil, and its usefulness in understanding the complex relationships existing in the approach of odor in neoplastic wounds, primary or secondary quantitative research provides methodologically robust ways to know the clinical efficacy and cost of treatments, interventions, or other aspects of health care30.
The quantitative researches, mainly produced by nursing, especially in England, France and Canada, highlight the concern and interest of this profession in the search for solutions to the challenging odor control in order to provide high quality palliative care, thus promoting health and restoring the dignity of these patients.
The understanding of the latent trait knowledge has unfolded from the broad definition of the word: familiarity with or understanding of a science, art or technique; jurisdiction to intervene in proceedings; awareness of self and others31. The semantic analysis of these meanings allowed the characterization of three dimensions, namely:self-evaluation, technical-scientific knowledge and skills and abilities to evaluate and control odor in neoplastic wounds. This result is in agreement with the academic assumptions of the area32,33.
The analysis of the 19 studies allowed the identification of 26 variables associated to the three dimensions emanating from the term knowledge, of which we can note the valorization of those associated to the technical-scientific dimension, in 18 variables. This dimension was frequently associated to definition (n = 11) and neoplastic wound appearance (n = 10), main symptoms (n = 10), wound care (n = 9) and use of topcoats with antibacterial properties (n = 12), according to Figure 3.
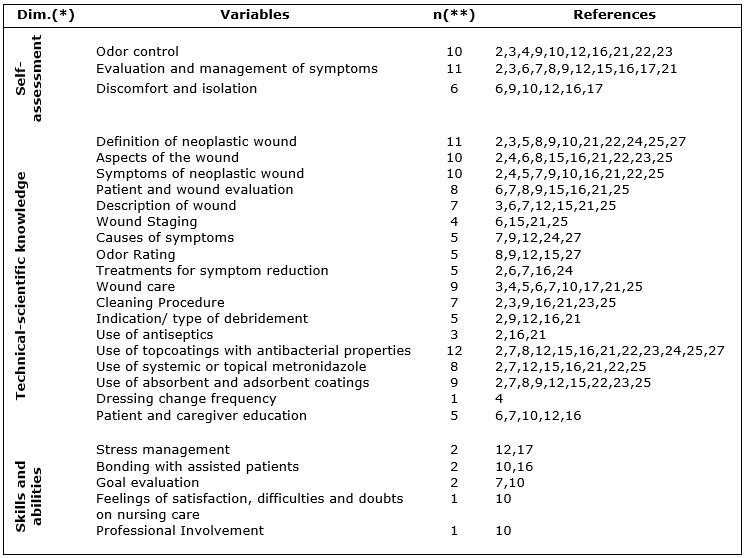
(
*) Dim.: Dimensions of knowledge; (**) n:
simple frequency of citations of variables.
FIGURE 3:
Variables associated with knowledge of odor control in neoplastic wounds.
Recife, 2016.
One possible explanation for this refers to the fact that the technical actions aimed at odor control, although it is a physical symptom, reflect positively on the sociopsychological manifestations.
Thus, for the expected performance of nurses, they need to be aware of the specific care to be provided, based on scientific principles and specific nursing knowledge about the physiology of healing, the available materials, the appropriate treatments and the characteristics of the lesion 14.
Regarding the dimension self-assessment, personal knowledge is an ongoing process that leads to change and growth, expressed by the deliberate actions and choices of the professional in his/her daily life33. In this dimension, three variables have been identified, in which the evaluation and management of symptoms (n = 11) had the highest frequency. See Figure 3.
The third dimension of knowledge - skills and abilities to evaluate and control the odor in neoplastic wounds - presented five variables, among which the most frequently were: stress management, bonding with assisted patients and goal evaluation (n = 2, each). See Figure 3.
Professional competence corresponds to a mixture of knowledge, technical, functional, managerial and behavioral skills. With the updating of information, together with the acquired experience, knowledge evolves and becomes complex, manifesting itself through competence34.
CONCLUSION
For the semantic analysis of the definition of knowledge and evaluation of studies on odor control in neoplastic wounds, three dimensions of knowledge and 26 related variables were detected. The dimension of technical-scientific knowledge was the most valued and the one with the highest number of variables cited by the studies analyzed.
The integrative review allowed us verifying that odor control has been poorly investigated in the last 14 years, although the issue has been a concern of nurses who have invested expressively in the best understanding of the problem and in the search for solutions through more refined methodological research.
This study had as main limitation the temporal cut, considering the possibility of occurrence of higher scientific production in previous years, mainly in developed countries. However, the classification of the dimensions of the latent trait knowledge as well as the identification of associated variables may contribute to a better understanding of nurses regarding the requirements necessary to improve knowledge about the control of this symptom, which is so challenging to the health professional and so uncomfortable for the patient.
We hope to widen the perception of managers and researchers to the importance of the construction of instruments of performance evaluation of nurses who care for cancer patients, mainly regarding the control of the odor of their wounds.
REFERENCES
1. Merz T, Carsten K, Uebach B, Kern M, Ostgathe C, Bükkia J. Fungating wounds – multidimensional challenge in palliative care. BreastCare. 2011;[cited in 2016 Feb 05]6(1):21–4.Available from: https://www.karger.com/Article/Abstract/324923
2. Gomes IP, Camargo TC. Tumoral skin lesions and nursing care: in search of evidences on symptoms management. Rev enferm UERJ. 2004; [cited in 2016 Feb 05]12(2):211-6. Available from: http://www.magonlinelibrary.com/toc/bjcn/7/8
3. Probst S , Arber A , Faithfull S . Malignant fungating wounds: a survey of nurses' clinical practice in Switzerland. Eur J OncolNurs. 2009;[cited in 2016 Jan12] 13(4 ): 295–8. Available from: http://www.ejoncologynursing.com/article/S1462-3889(09)00048-9/pdf
4. Lo SF, Hayter M, Hu WY, Tai CY, Hsu MY, Li YF. Symptom burden and quality of life in patients with malignant fungating wounds. J AdvNurs.2012; [cited in 2016 Jan 10]68(6):1312–21. Available from: http://onlinelibrary.wiley.com/doi/10.1111/j.1365-2648.2011.05839.x/pdf
5. Probst S, Arber A, Faithfull S. Coping with an exulcerated breast carcinoma: an interpretative phenomenological study. J Wound Care. 2013; [cited in 2016 Jan 22]22(7): 352-60. Available from: http://www.magonlinelibrary.com/doi/pdf/10.12968/jowc.2013.22.7.352
6. Castro MCF, Cruz PS, Grellmann MS, Santos WA, Fuly PSC. Palliative care for patients with oncological wounds in a teaching hospital: an experience report. Cogitare Enferm. 2014;[cited in 2016 Jan 15]19(4):841-4. Available from: http://revistas.ufpr.br/cogitare/article/view/37294/23968
7. Chrisman CA. Care of chronic wounds in palliative care and end-of-life patients. Int Wound J. 2010;[cited in 2016 Mar 05]7(4):214-35. Available from: http://onlinelibrary.wiley.com/doi/10.1111/iwj.2010.7.issue-4/issuetoc
8. Costa Santos CM, MattosPimenta CA, NobreMR. A systematic review of topical treatments to control the odor of malignant fungating wounds. J PainSymptomManage. 2010; [cited in 2016 Mar 15] 39(6):1065-76. Available from: http://www.jpsmjournal.com/article/S0885-3924(10)00246-0/pdf
9. O'Brien C. Malignant wounds. Can Fam Physician.2012; [cited in 2016 Mar 15]58(3): 272-4. Available from: http://www.cfp.ca/content/58/3/272.full.pdf+html
10. FirminoF, Alcântara LFFL. Nurses in the provision of outpatient care for women with malignant fungating wounds in the breasts. Rev RENE . 2014; [cited in 2016 Mar 26]15(2): 298-307. Available from: http://www.revistarene.ufc.br/revista/index.php/revista/issue/view/73
11. Grocott P, Gethin G, Probst S. Malignant wound management in advanced illness: new insights. CurrOpin Support Palliat Care. 2013;[cited in 2016 Mar 26]7(1):101-5. Available from: http://journals.lww.com/co-supportiveandpalliativecare/toc/2013/03000
12. Samala RV, Davis MP.Comprehensive wound malodor management: Win the RACE. CleveClin J Med.2015;[cited in 2016 Jan 05]82(8):535-43. Available from: http://www.ccjm.org/view-df.html?file=uploads/media/Samala_WoundMalodorManagement
13. Maida V, Alexander S, Case AA, Fakhraei P. Malignant wound management. Public Health Emerg. 2016;[cited in 2016 Feb 20]1(12): 1-14. Available from: http://phe.amegroups.com/issue/view/209
14. Azevedo IC, Costa RKS, Holanda CSM, Salvetti MG, Torres GV. Family health strategy nurses' kowledge of assessment and treatment of oncologic wounds. Rev brascancerol. 2014;[cited in 2016 Fev 20] 60(2): 119-27. Available from: http://www.inca.gov.br/rbc/n_60/v02/pdf/05-artigo-conhecimento-de-enfermeiros-da-estrategia-saude-da-familia-sobre-avaliacao-e-tratamento-de-feridas-oncologicas.pdf
15. Dowset C. Malignant fungating wounds: assessment and management. Br J CommunityNurs. 2002;[cited in 2016 Mar 05]7(8):394-400. Available from: http://www.magonlinelibrary.com/toc/bjcn/7/8
16. Seaman S. Management of malignant fungating wounds in advanced cancer. SeminOncolNurs. 2006;[cited in 2016 Mar 05]22(3):185–93. Available from: http://www.seminarsoncologynursing.com/article/S0749-2081(06)00060-X/pdf
17. Harrison MB, Graham ID, Hoek J, Dogherty EJ, Carley ME, Angus V. Guideline adaptation and implementation planning: a prospective observational study. ImplementSci.2013; [cited in 2016 Feb 20]8(8):49. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3668213/
18. Soares CB, Hoga LAK, Peduzz M, Sangaleti C, Yonekura T, Silva DRAD. Integrative review: concepts and methods used in nursing. Rev esc enferm USP. 2014; [cited in 2016 Feb 20]48(2):335-45. Available from: http://www.scielo.br/pdf/reeusp/v48n2/0080-6234-reeusp-48-02-335.pdf
19. Botelho LLR, Cunha CCA, Macedo M. The integrative review method in organizational studies 2011; [cited in 2016 Mar 05]5(11):121-36. Available from: https://www.gestaoesociedade.org/gestaoesociedade/article/view/1220
20. National Academy of Palliative Care. Manual of Palliative Care ANCP: expanded and updated. 2nd ed. Sao Paulo: ANCP; 2012.
21. Firmino F. Patients carriers of neoplasic wounds in palliative care services: contributions to elaboration of nursing protocol interventions. Rev brascancerol. 2005; [cited in 2016 Mar 26]51(4): 347-59. Available from: http://www.inca.gov.br/rbc/n_51/v04/pdf/revisao6.pdf
22. Adderley UJ, Holt IG. Topical agents and dressings for fungating wounds. Cochrane DatabaseSyst Rev. 2014;[cited in 2016 Feb 16]15(5). Available from: http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003948.pub3/epdf
23. Lund-Nielsen B, Adamsen L, Gottrup F, Rorth M, Tolver A, Kolmos HJ. Qualitative bacteriology in malignant wounds - a prospective, randomized, clinical study to compare the effect of honey and silver dressings. OstomyWoundManage. 2011;[cited in 2016 Mar 25]57(7):28-36. Available from: http://www.o-wm.com/content/qualitative-bacteriology-malignant-wounds%E2%80%94-prospective-randomized-clinical-study-compare-eff
24. Fromantin I, Seyer D, Watson S, Rollot F, Elard J, EscandeMC,et al. Bacterial floras and biofilms of malignant wounds associated with breast cancers. J ClinMicrobiol. 2013;[cited in 2016 Mar 25]51(10):3368-73. Available from: http://jcm.asm.org/content/51/10/3368.long
25. Fromantin I, Watson S, Baffie A, Rivat A, Falcou MC, KriegelI,et al. A prospective, descriptive cohort study of malignant wound characteristics and wound care strategies in patients with breast cancer. OstomyWoundManage. 2014;[cited in 2016 Mar 06]60(6):38-48. Available from:http://www.o-wm.com/issue/2632
26. Costa Santos CM, Mattos Pimenta CA, Nobre MR. A systematic review of topical treatments to control the odor of malignant fungating wounds. J Pain Symptom Manage. 2010;[cited in 2016 Feb 16]39(6):1065-76. Available from: http://www.jpsmjournal.com/article/S0885-3924(10)00246-0/pdf
27. Shirasu M, Nagai S, Hayashi R, Ochiai A, Touhara K. Dimethyl Trisulfide as a characteristic odor associated with fungating cancer wounds . Biosci Biotechnol Biochem. 2009;[cited in 2016 Feb 16]73(9):2117-20. Available from: http://www.tandfonline.com/doi/pdf/10.1271/bbb.90229?needAccess=true
28. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;[cited in 2016 Feb 16]61(2): 134. Available from: http://onlinelibrary.wiley.com/doi/10.3322/caac.20107/epdf
29. Rossi S, Baili P, Capocaccia R, Caldora M, Carrani E, Minicozzi P, et al. The EUROCARE-5 study on cancer survival in Europe 1999–2007: database, quality checks and statistical analysis methods. EurJCancer. 2015; [cited in 2016 Feb 16]51(15): 2104–19. Available from: http://www.ejcancer.com/article/S0959-8049(15)00776-5/pdf
30. Rapport F, Storey M, Porter A, Snooks H, Jones K, PeconiJ,et al. Qualitative research within trials: developing a standard operating procedure for a clinical trials unit. Trials. 2013;[cited in 2016 Mar 05]14:54-61. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3599333/pdf/1745-6215-14-54.pdf
31. Ferreira ABH. Aurelio Dictionary of the Portuguese Language. 5th ed. Curitiba (PR): Positivo; 2010.
32. Mccluskey P, Mccarthy G. Nurses' knowledge and competence in wound management. Wounds UK. 2012; [cited in 2016 Mar 05]8(2): 37-47. Available from: http://www.wounds-uk.com/pdf/content_10426.pdf
33. Chinn PL, Kramer MK. Knowledge development in nursing. 9th ed. Missouri (EUA): Elsevier; 2015.
34. Broeiro P. Knowledge and competence. Rev Port Med Geral Fam. 2015; [cited in 2016 Mar 05] 31(2):82-4. Available from: http://www.scielo.mec.pt/pdf/rpmgf/v31n2/v31n2a01.pdf