FIGURE 1: Comprehensiveness devices, their concepts and analysis line. Fortaleza-CE, 2013.
ORIGINAL RESEARCH
Association between antihypertensive treatment adherence and comprehensive nursing care
Antônia Sylca de Jesus SousaI, Thereza Maria Magalhães MoreiraII, Ana Larissa Gomes MachadoIII, Ana Zaira da SilvaIV
I
Nurse. MS in Clinical Care in Nursing and Health. Ceará, Brazil. E-mail: sylcasousa88@hotmail.com
II
Nurse. PhD. Adjunct Professor. Ceará State University. Ceará, Brazil.
E-mail:
tmmmoreira@pq.cnpq.br
III
Nurse. PhD. Adjunct Professor. Federal University of Piauí. Piauí, Brazil.
E-mail:
analarissa2001@yahoo.com.br
IV
Nurse. MS. PhD student in Collective Health. Federal University of Ceará.
Ceará, Brazil. E-mail: anazaira18@hotmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2018.25250
ABSTRACT
Objective: to examine the association between client adherence to antihypertensive treatment and comprehensive nursing care. Methodology: quantitative study conducted Fortaleza, Ceará, with 602 hypertensive patients treated at a Secondary Health Care Center. Treatment adherence was identified by applying Morisky-Green test and the comprehensiveness of care was assessed using a checklist based on Starfield's principles (accessibility, placement, involvement and family approach). Variables were correlated using Pearson's Chi-Square Test (X2). The study was approved by the research ethics committee. Results: no association was found between treatment adherence and the comprehensiveness of nursing care (p = 0.758). Conclusion: there was found to be a need to provide nursing care centered on comprehensiveness, with a view always to improving treatment adherence among hypertensive patients.
Descriptors: Integrality in health; comprehensive health care; medication adherence; nursing.
INTRODUCTION
Conceptualized as a set of diseases that present high rates of mortality, morbidity and disability, the Chronic Non-communicable Diseases (CNCDs) are a public health problem that has perpetuated over the years, especially in developing countries such as Brazil. Among the most important CNCDs, the Systemic Arterial Hypertension (SAH) stands out because it has a high incidence and prevalence in contemporary societies, constituting the main reason for consultations in primary care, as well as in other levels of health care.1-3
The pharmacological treatment combined with non-pharmacological measures favors the control of the blood pressure (BP). However, scientific evidence has revealed that the lack of adherence to treatment is one of the main factors that hinder the effective control of hypertension, since about 40% to 60% of the patients do not use the prescribed medications, and this percentage increases when the lack of adherence is related to the lifestyle, a fact that converges with the results of recent research that indicates that only half of people with SAH can maintain blood pressure levels.4,5,6
As a professional category directly linked to care and therefore very close to the client at all the care levels of the system, nursing plays a fundamental role, especially regarding the implementation of comprehensive care.7 As it represents one of the three guidelines of the Unified Health System-SUS ("Sistema Único de Saúde", in Portuguese) contemplated in the Federal Constitution of 1988, the comprehensiveness is an effective means of achieving excellence in results through the development of actions that are part of its basis, among other instruments, on health education, developed in the different scenarios of nurses' performance.
Considering the influence that the care provided by the nurses, based especially on the comprehensiveness, exerts on the life and health of the people, the objective was to verify the association between the level of adherence of the clients to the antihypertensive treatment and the comprehensiveness in the care provided by nurses.
LITERATURE REVIEW
The adherence to treatment is directly related to its acceptance and recognition of the disease, in this case, the SAH, since its treatment in a situation of chronic illness does not only influences the personal motivation of the patient. Different nuances interfere in this process, such as low socioeconomic status, deficiency of self-care and knowledge about the disease, among others.8 Thus, in order to have adherence to treatment, the behavior of each subject must be in accordance with the guidelines established by the health professionals, who must be closely linked to the drug therapy and changes in lifestyle. 5,9,10
In this context, it is emphasized that the effective participation of health professionals is necessary for adherence to the antihypertensive treatment. The nurse, as a member of the health team, assumes co-responsibility for the actions of care for the health promotion and prevention of injuries regarding the life and health of the subjects, especially when they need to live with some type of chronic illness. Through scientific knowledge and their role as educator, this professional has the possibility to lead the patients to the accomplishment of a satisfactory treatment, which will result in the improvement of their well-being.11,12
Comprehensiveness in health goes beyond a guideline, one of its dimensions is the observance of the expanded concept in health, which should pay attention not only to the aspects of disease, but also to the social and psychological aspects. It also emerges as a principle of continuous organization of the work process, by the expansion of possibilities that seek to apprehend the health needs of a given population group. Thus, when speaking in comprehensiveness, it is also spoken of interdisciplinarity of care, referring to the accomplishment of inter subjective practices through the establishment of interpersonal relations between the subjects, through which success is achieved through dialogical health practices, especially when they are established among nurses and people living with SAH, because in this case, the relationship is more intense and narrow.13,14,15
METHODOLOGY
This is an analytical study, with a quantitative approach, carried out at a reference center in Fortaleza-CE, with data collection from April to June 2013. The study population consisted of hypertensive patients treated in the unit and it was calculated by the formula for infinite population, 16 being of 602 hypertensive people.
In order to analyze the presence or absence of adhesion, the Morisky and Green test was applied17, composed of four questions: Do you sometimes have trouble remembering to take your medication? Do you sometimes neglect to take your medicine? When you are feeling well, do you sometimes stop taking your medicine? Sometimes, if you feel worse while taking the medication, do you stop taking it?
Thus, the patient was classified into the adherence group when the answers to all the questions were negative. However, when at least one of the answers was affirmative, the patient was classified as non-adherent. 18
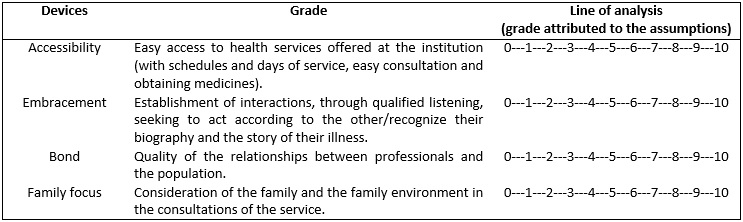
Then, it was verified how the comprehensiveness of the care was configured. To obtain this result, we evaluated the comprehensiveness based on the devices proposed by Starfield,19 operationalized as horizontal comprehensiveness (access, embracement, bond and family focus). 19,20
The comprehensiveness devices, the concept presented and the analysis line used to assign a grade to the device, according to the user's view, are described in Figure 1.
FIGURE 1:
Comprehensiveness devices, their concepts and analysis line. Fortaleza-CE,
2013.
The analysis line proposes grades for the comprehensiveness devices, to which the participants gave a grade based on the perception they have regarding the care received in the service. This was done by means of a checklist instrument with a Likert-type scale, with a score from zero to ten (0---1---2---3---4---5---6---7---8---9---10). From this point, it was sought to classify the presence of comprehensiveness when it was obtained a grade seven in 50% of the devices, in the total score of each questionnaire. Otherwise, the absence of comprehensiveness was considered.
With the results of the presence of adherence/non-adherence to the antihypertensive treatment and the investigation of the presence/absence of comprehensiveness in the nursing care provided to the patients, it was verified if there was an association between these variables. In order to do so, the variables were cross-linked by means of the Pearson Qui-square statistical test (X2). The data collected were tabulated and organized using the Statistical Package for Social Sciences (SPSS) version 20.0. After being grouped, the results were presented in figure and table, and the discussion was carried out according to the pertinent literature.
The project was approved by the Committee of Ethics in Research with human beings of the Ceará State University, with opinion No. 400,990.
RESULTS AND DISCUSSION
The association between adherence to the antihypertensive treatment and comprehensiveness in care by the nurse can be observed in Table 1:
TABLE 1:
Analysis of adherence to the antihypertensive treatment according to the
presence and absence of comprehensive care. Fortaleza-Ceará-Brazil, 2013.
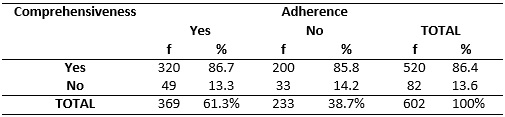
It was verified that of the 369 (61.3%) patients who adhered to the treatment, 320 (86.7%) reported presence of comprehensiveness in care. Of the 233 (38.7%) patients who did not adhere to the treatment, 200 (85.8%) of them also reported the presence of comprehensiveness.
When cross-linking adherence and comprehensiveness of care, it was found that almost two-thirds of the patients adhered to the treatment of SAH, being the comprehensiveness verified by patients with and without adherence to the treatment; thus, it can be stated that there was no association between adherence and comprehensiveness in the antihypertensive treatment, because no statistically significant association was found (p=0.758).
It was also verified that adherence was 1% higher in the patients who reported comprehensiveness. This may reflect a low accuracy in the presence or absence of comprehensiveness, due to the criterion adopted to verify its presence (obtain grade seven in fifty percent of the devices) or difficulty of the people to assign grades to the care received.
It should be emphasized that the comprehensive evaluation instrument had seven grades for negative evaluation (0-6) and only four for positive ones (7-10) and that, nevertheless, only 82 patients (13.6%) were in the category of absence of comprehensiveness.
In a study carried out to evaluate adherence to drug treatment in users enrolled in the Hiperdia Program in the city of Teresina - Piauí (PI), the authors used the Morisky-Green test to assess adherence and non-adherence to treatment, which was also used in this study and found that almost half of the participants did not forget to use the drug.21
Among the factors that influence the low adherence, researches show that socioeconomic factors stand out with high frequency, since the lower their levels, the lower the adherence rates to the antihypertensive treatment, considering that the knowledge of the disease is more superficial and access to the health services is difficult.9,22
A good strategy to encourage patients to adhere to the treatment is to make them aware of the harm that high blood pressure can cause when not treated properly. In addition to the risks inherent to the treatment, its benefits and peculiarities must be evidenced, favoring that the individual becomes an active subject in their own treatment.23,24
When investigating the presence of comprehensiveness in the nursing care provision to patients with hypertension, it was confirmed that there are many the senses for comprehensiveness, among them the universal right to have the health needs of the user met, seeking resolution in the actions and adequate responses to the problems identified. The comprehensiveness seeks to meet to the organic, emotional, social and spiritual aspects related to the illness of the people within a social context, aiming at the restoration of the vitality of individuals and collectivities.7
With regard to Regarding the embracement, this is a tool that allows universal access to services, making them humanized, comprehensive, with resoluteness and quality, making the health problems of users the responsibility of professionals. Embracing well is a key strategy for establishing a bond between health team and users, and it is considered a working tool capable of producing satisfactory results at reduced intervals.5,25
As the establishment of links, the embracement is a tool of fundamental importance in the context of health professionals caring for people with some type of chronic illness, such as hypertension. Both are part of the goals set by the National Humanization Policy, through the broadening of the access and valuing the user as the main actor in the health-disease process. From the bond, it is possible to establish affection between professionals and patients, through which it will be possible to develop democratic relationships focused on the care provided.26
Regarding the Family Focus, it is known that non-adherence to the medical treatment of a chronic disease involves much more than the conflicts related to the disease. This is a complex issue that includes, among other aspects, the lack of family support, which is of fundamental importance for facing the health condition. The support manifests itself in several ways, such as: remembering the person with hypertension of the medication schedule and guiding them regarding the diet; or even regarding the willingness to accompany the hypertensive patient to the consultations. 27
In fact, nursing care involves more than just doing, it involves commitment, responsibility, knowledge, bonding and acceptance. It should be emphasized that the establishment of an adequate relationship between professional and user, dialogue/communication, comfort from the companions, care with a focus on patient safety and comprehensiveness in the health maintained in intra and extra-hospital environments contribute to humanization of care, because caring presupposes, in addition to the technical knowledge, a broad view that makes it possible to know the human being in its totality, to relate.28,29
Therefore, it is worth emphasizing the need for a more rigorous and individualized care for patients with hypertension, through a multidisciplinary team that seeks to assess them in a holistic way, covering all the social and political context in which they are inserted.
CONCLUSION
Based on the use of the Morisky-Green test, the prevalence of adherence to the treatment of hypertension among the participants of this study was verified. However, when cross-linking adherence and comprehensiveness of care, there was no statistical association.
Thus, it is concluded that maintaining comprehensiveness in the daily life of health practices is to defend that the provision of care is adequately inserted in the particular context of each moment. It should be emphasized that any perspective of change that aims at improving the quality of the nursing care should focus on processes of interaction between users and professionals, identifying obstacles and potentialities through experiences, which aim at comprehensive care and pertinent to the most varied realities.
The need to establish bonds in the relationships between professionals and users is highlighted, and this constitutes the great challenge of comprehensive care; as well as the production of health promotion actions aimed at the (re)construction of the care centered on the subject.
It is necessary to promote a nursing care centered in the comprehensiveness of care, that increasingly seeks the adherence of the subjects to the treatment, through an environment that favor the accessibility and embracement, and the integrality devices should be surrounded by a wide network of professional relations whose center of action should be the client and their health needs.
As a limitation of the study, it is emphasized the lack of specific instruments to measure the comprehensiveness in the care provided by the nurses, thus, the proposed scores to classify the presence of comprehensiveness did not present pre-defined cut-off points in the literature. In addition, there is little literature on the comprehensiveness of nurses' care provision.
REFERENCES
1.Martins LN, Souza LS, Silva CF, Machado RS, Silva CEF, Vilagra MM, et al. Fatores de risco cardiovascular em adultos admitidos na unidade de dor torácica em Vassouras, RJ. Rev. Bras. Cardiol. 2011; 24(5):299-307.
2.Ministério da Saúde (Br). Cadernos de Atenção Básica: Estratégias para o cuidado da pessoa com doença crônica – Hipertensão Arterial Sistêmica. Brasília; 2013.
3.Santos MVR, Oliveira DC, Arraes LB, Oliveira DAGC, Medeiros L, Novaes MA. Adesão ao tratamento anti-hipertensivo: conceitos, aferição estratégias inovadoras de abordagem. Rev. Bras. Clin. Med. 2013; 11(1):55-61.
4.Motter FR, Olinto MTA, Paniz VMV. Avaliação do conhecimento sobre níveis tensionais e cronicidade da hipertensão: estudo com usuários de uma Farmácia Básica no sul do Brasil. Cad. Saúde Pública (Online). 2015; 31(2):395-404.
5.Dougados M, Soubrier M, Perrodeau E, Gossec L, Fayet F, Gilson M, et al. Impact of a nurse-led programme on comorbidity management and impact of a patient selfassessment of disease activity on the management of rheumatoid arthritis: results of a prospective, multicentre, randomised, controlled trial (COMEDRA). Ann Rheum. Dis. 2015; 74:1725-33.
6.Silva TC, Dantas AB, Menezes BD, Silveira EVS, Reis HG, Silveira JP, et al.Método de adesão ao tratamento de pacientes hipertensos. Arch Health Invest. 2017; 6(4):155-158.
7.Coutinho AT, Popim RC, Carregã K, Spiri WC. Integralidade do cuidado com o idoso na Estratégia de Saúde da Família: visão da equipe. Esc. Anna Nery. 2013; 17(4):628-37.
8.Souza NPG, Oliveira GYM, Girão ALA, Souza LM, Maniva SJCF, Freitas CHA. Adoecimento por hipertensão arterial e diabetes mellitus: concepções de um grupo de pacientes hospitalizados. Rev. enferm. UERJ. 2015; 23(1):52-7.
9.Hanus JS, Simões PW, Amboni G, Ceretta LB, Tuon LGB. Associação entre a qualidade de vida e adesão à medicação de indivíduos hipertensos. Acta Paul. Enferm. (Online). 2014; 28(4):381-7.
10.Tavares DMS, Guimarães MO, Ferreira PCS, Dias FA, Martins NPF, Rodrigues LR. Qualidade de vida e adesão ao tratamento farmacológico entre idosos hipertensos. Rev. bras. enferm. (Online) 2016; 69(1):134-41.
11.Costa YF, Araújo OC, Almeida LBM, Viegas SMF. O papel educativo do enfermeiro na adesão ao tratamento da Hipertensão Arterial Sistêmica: revisão integrativa da literatura. O Mundo da Saúde. 2014; 38(4):473-81.
12.Wang W, Lau Y, Chow A, Thompson DR, He HG. Health-related quality of life and social support among Chinese patients with coronary heart disease in mainland China. European Journal of Cardiovascular Nursing. 2014; 13(1):48-54.
13.Santos FPA, Nery AA, Matumoto S. A produção do cuidado a usuários com hipertensão arterial e as tecnologias em saúde. Esc. Enferm. USP. 2013; 47(1):107-14.
14.Guedes MBOG, Lima KC, Caldas CP, Veras RP. Apoio social e o cuidado integral à saúde do idoso. Physis Revista de Saúde Coletiva. 2017; 27940:1185-1204.
15.Almeida RT, Ciosak SI. Comunicação do idoso e equipe de Saúde da Família: há integralidade?. Rev. latinoam. enferm. (Online). 2013; 21(4):1-7.
16.Pocock SJ. Clinical trials-a practical approach. New York: John Wiley & Sons; 1989.
17.Morisky DE, Green LW, Levine DM. Concurrent and predective validity of self-reported measure of medication adherence. Med. Care. 1986; 24(1):67-74.
18.Sewitch MJ, Abrahamowicz M, Barkun A, Bitton A, Wild GE, Cohen A, et al. Patient nonadherence to medication in inflammatory Bowel disease. Am J Gastroenterol. 2003; 98(7):1535-44.
19.Starfield B. Atenção primária: equilíbrio entre necessidades de saúde, serviços e tecnologia. Brasília: Unesco, MS, 2002.
20.Sala A, Luppi CG, Simões O, Marsiglia RG. Integralidade e Atenção Primária à Saúde: avaliação na perspectiva dos usuários de unidades de saúde do município de São Paulo. Saúde Soc. São Paulo. 2011; 20(4):948-60.
21.Carvalho AKM, Leopoldino RWD, Silva JEG, Cunha CP. Adesão ao tratamento medicamentoso em usuários cadastrados no Programa Hiperdia no município de Teresina (PI). Ciência & Saúde Coletiva. 2012; 17(7):1885-92.
22.Silva LFRS, Marino JMR, Guidoni CM, Girotto E. Fatores associados à adesão ao tratamento anti-hipertensivo por idosos na atenção primária. Rev. Ciênc. Farm. Básica Apl. 2014; 35(2):269-76.
23.Nascimento ACG, Alves ACP, Almeida AIM, Oliveira CJ. Características da adesão terapêutica em pessoas com hipertensão arterial e identificação do diagnóstico de enfermagem "falta de adesão" na atenção primária. Rev. APS. 2013; 16(4):365-77.
24.Schmieder R, Gitt AK, Koch C, Bramlage P, Ouarrak T, Tschõpe D, et al. Achievement of individualized treatment targets in patients with comorbid type-2 diabetes and hypertension: 6 months results of the dialogue registry. BMC Endocrine Disorders. 2015; 15(23):2-12.
25.Machado LM, Colomé JS, Silva RM, Sangoi TP, Freitas NQ. Significados do fazer profissional na estratégia de saúde da família: atenção básica enquanto cenário de atuação. J Res Fundam Care Online. 2016; 8(1):4026-35.
26.Lima LL, Moreira TMM, Jorge MSB. Produção do cuidado a pessoas com hipertensão arterial: acolhimento, vínculo e corresponsabilização. Rev. bras. enferm. (Online). 2013; 66(4):514-22.
27.Faquinello P, Marcon SS. Amigos e vizinhos: uma rede social ativa para adultos e idosos hipertensos. Esc. Enferm. USP. 2012; 45(6):1345-52.
28.Silva-Costa A, Griep RH, Rotenberg L. Disentangling the effects of insomnia and night work on cardiovascular diseases: a study in nursing professionals. Braz J Med Biol Res. 2015; 48(2):120-7.
29. Santos CKR, Moraes JRMM, Santos NLP, Souza TV, Morais RCM, Azevedo SD. Qualidade da assistência de enfermagem em uma emergência pediátrica: perspectiva do acompanhante. Rev. enferm. UERJ. 2016; 24(4):e17560.